Professional Documents
Culture Documents
2 Airway
2 Airway
Uploaded by
Alex RodrigoOriginal Description:
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
2 Airway
2 Airway
Uploaded by
Alex RodrigoCopyright:
Available Formats
PART
PART I CRITICAL CARE PROCEDURES, MONITORING, AND PHARMACOLOGY I
CHAPTER
Chapter 2
Airway Management in
2
Airway Management in the Critically Ill Adult
the Critically Ill Adult
G. G. Lavery and C. A. Jamison
mation can be gained from a variety of sources.1-5 The
Structure and Function of the Normal Airway
airway begins at the nose and oral cavity and continues
The Nose
The Oral Cavity as the pharynx and larynx, which lead to the trachea
The Pharynx (beginning at the lower edge of the cricoid cartilage) and
The Larynx then the bronchial tree. The airway1 provides a pathway
The Tracheobronchial Tree for airflow between the atmosphere and the lungs2; facili-
Overview of Airway Function tates filtering, humidification, and heating of ambient air
Assessing Adequacy of the Airway before it reaches the lower airway3; prevents nongaseous
Patency material from entering the lower airway6; and allows pho-
Protective Reflexes
nation by controlling the flow of air through the larynx
Inspired Oxygen Concentration
Respiratory Drive
and oropharynx.4
Management of the Airway
Providing an Adequate Inspired Oxygen Concentration The Nose
Establishing a Patent and Secure Airway The nose has a midline septum separating two cavities
Providing Ventilatory Support that communicate externally via the external nares (nos-
Physiologic Sequelae and Complications of Tracheal trils). Each cavity has a roof formed by the nasal carti-
Intubation lages, frontal bones, cribriform plate, ethmoid, and body
The Difficult Airway of sphenoid. Portions of the maxilla and palatine bones
Recognizing the Potentially Difficult Airway make up the nasal floor (which also forms part of the roof
The Airway Practitioner and the Clinical Setting of the oral cavity). The medial wall of each nasal cavity
Managing the Difficult Airway is formed by the nasal septum, the vomer, and ethmoid
Confirming Tube Position in the Trachea bones. The lateral wall lies medial to the orbit, the ethmoid,
Surgical Airway and maxillary sinuses and has three horizontal bony pro-
Cricothyrotomy jections—the superior, middle and inferior nasal conchae.
Tracheostomy
These greatly increase the surface area, and the overly-
Extubation in the Difficult Airway Patient ing mucosa is highly vascular, supplied by the maxillary
(Decannulation)
arterial branch of the external carotid artery and the
Tube Displacement in the Critical Care Unit ethmoidal branch of the ophthalmic artery. The (nonolfac-
Endotracheal Tube
Tracheostomy Tube
tory) sensory innervation of the nasal mucosa is by two
divisions of the trigeminal nerve.
Common Problems in Airway Management
The Oral Cavity
The teeth form the lateral wall of the oral cavity, while
Appropriate management of the airway is the corner-
the floor is the tongue—a mass of horizontal, vertical, and
stone of good resuscitation. It requires judgment (airway
transverse muscle bundles attached to the mandible and
assessment), skill (airway maneuvers), and constant reas-
the hyoid bone. The sulcus terminalis, a V-shaped groove,
sessment of the patient’s condition. Although complex
divides the anterior two thirds of the tongue (sensory
procedures sometimes are life-saving and always carry the
innervation from the lingual nerve and taste from the
potential to impress, the timely use of simple airway
chordae tympani) from the posterior one third (sensory
maneuvers often is very effective and may avoid the need
supply from the glossopharyngeal nerve). All intrinsic and
for further intervention.
extrinsic muscles of the tongue are supplied by the hypo-
glossal nerve, except the palatoglossus, which is supplied
STRUCTURE AND FUNCTION OF by the vagus nerve.
THE NORMAL AIRWAY
Critical care staff require an understanding of structure The Pharynx
and function in order to successfully manage the airway The adult pharynx is a midline structure, running anterior
and the conditions that may affect it. The relevant infor- to the cervical prevertebral fascia, from the base of the
17
Ch002-A04841.indd 17 9/13/2007 9:56:04 AM
PART
I
skull to the level of the sixth cervical vertebrae (approxi- tension of the vocal cords, while sliding and rotational
mately 14 cm), and continuing as the esophagus. It is a movements of the arytenoid cartilages can alter the shape
CRITICAL CARE PROCEDURES, MONITORING, AND PHARMACOLOGY
muscular tube with three portions: the nasopharynx, oro- of the glottic opening between the vocal cords. Fine
pharynx, and laryngopharynx (or hypopharynx). It con- control of the muscles producing these movements allows
tains three groups of lymphoid tissue: the adenoids, the vocalization as air passes between the vocal cords in
pharyngeal tonsil (on the posterior wall), and the palatine expiration. The sound volume is increased by resonance
(lingual) tonsils and has the inner opening of the eusta- in the sinuses of the face and skull.
chian tube on each lateral wall. The vagus nerve supplies
all but one of the pharyngeal muscles. Sensory supply is The Tracheobronchial Tree
via branches of the glossopharyngeal and vagus nerves. The trachea is a fibrous tube, 2 cm in diameter, running
The pharynx provides a common pathway for the upper in the midline for 10 to 15 cm from the level of the sixth
alimentary and respiratory tracts and is concerned with cervical vertebra to its bifurcation (carina) at the level of
swallowing and phonation. the fourth thoracic vertebra. The walls include 15 to 20
incomplete cartilaginous rings limited posteriorly by
The Larynx fibroelastic tissue and smooth muscle.
The larynx sits anterior to the laryngopharynx and the The cervical trachea lies anterior to the esophagus, with
fourth to the sixth cervical vertebrae and is posterior to the recurrent laryngeal nerve in the groove between the
the infrahyoid muscles, the deep cervical fascia, and the two. Anteriorly lie the cervical fascia, infrahyoid muscles,
subcutaneous fat and skin that cover the front of the neck. isthmus of the thyroid, and the jugular venous arch. Later-
Laterally lie the lobes of the thyroid gland and carotid ally lie the lobes of the thyroid gland and the carotid
sheath. The larynx acts as a sphincter at the upper end of sheath. In the thorax, the trachea is traversed anteriorly
the respiratory tract and is the organ of phonation. The by the brachiocephalic artery and vein (which may be
epiglottis and the thyroid, cricoid, and paired arytenoid, damaged or eroded by the tracheostomy tube). To the left
cuneiform, and corniculate cartilages, together with the are the common carotid and subclavian arteries and the
interconnecting ligaments, make up the skeleton of the aortic arch. To the right are the vagus nerve, the azygos
larynx, which has a volume of 4 mL. Two pairs of parallel vein, and the pleura. The carina lies anterior to the esoph-
horizontal folds project into the lumen of the larynx—the agus behind the bifurcation of the pulmonary trunk.
false vocal cords (lying superiorly) and the true vocal The bronchial tree is similar in structure to the trachea.
cords (inferiorly). The opening between the true cords is Two main bronchi diverge from the carina. The right main
called the glottis. The larynx communicates above with bronchus is shorter, wider, and more vertical and runs
the (laryngo)pharynx and below with the trachea, which close to the pulmonary artery and the azygos vein. The
begins at the lower edge of the cricoid ring. left main bronchus passes under the arch of the aorta,
The superior aspect of the epiglottis is innervated by anterior to the esophagus, thoracic duct, and descending
the glossopharyngeal nerve, whereas the vagus, via its aorta.7
superior laryngeal (SLN) and recurrent laryngeal (RLN)
branches, innervates the larynx, including the inferior Overview of Airway Function
surface of the epiglottis. The external (motor) branch of In the nose, inspired gas is filtered, humidified, and warmed
the SLN supplies the cricothyroid muscle, and the internal before entering the lungs. Resistance to gas flow through
branch is the sensory supply to the larynx down to the the nose is twice that of the mouth, explaining the need to
vocal cords. The RLN supplies all of the intrinsic laryngeal mouth-breathe during exercise when gas flows are high.
muscles and is the sensory supply to the larynx below the Warming and humidification continue in the pharynx and
cords. Injury to the SLN causes hoarseness secondary to tracheobronchial tree. Between the trachea and the alveo-
a loss of tension in the ipsilateral vocal cord. Complete lar sacs, airways divide 23 times. This increases the cross-
unilateral RLN palsy inactivates both ipsilateral adductor sectional area for the gas exchange process but also reduces
and abductor muscles. Vocal cord adduction, however, is the velocity of gas flow. Hairs on the nasal mucosa filter
maintained by the unopposed SLN-innervated cricothy- inspired air, trapping particles greater than 10 µm in diam-
roid muscle. With bilateral RLN palsy, both cords are in eter. Many particles settle on the nasal epithelium. Parti-
adduction as a result of the unopposed action of the cri- cles 2 to 10 µm in diameter fall on the mucus-covered
cothyroid muscle. On inspiration, the adducted vocal bronchial walls (as airflow slows), initiating reflex bron-
cords then act like a Venturi device, generating a negative choconstriction and coughing. Ciliated columnar epithe-
pressure that pulls the cords together, producing inspira- lium lines the respiratory tract from the nose to the
tory stridor—the characteristic sign of upper airway respiratory bronchioles (except at the vocal cords). The
obstruction. Laryngospasm, a severe form of airway cilia beat at a frequency of 1000 to 1500 cycles per minute,
obstruction, may be triggered by mechanical stimulation enabling them to move particles away from the lungs at a
of the larynx or by cord irritation due to aspiration of oral rate of 16 mm per minute. Particles less than 2 µm in diam-
secretions, blood, or vomitus. eter may reach the alveoli, where they are ingested by
In health, the laryngeal abductor muscles contract early macrophages. If ciliary motility is defective as a result of
in inspiration, separating the vocal cords and facilitating smoking or an inherited disorder (e.g., Kartagener’s syn-
airflow into the tracheobronchial tree. Movements of the drome or another ciliary dysmotility syndrome), the
thyroid and arytenoid cartilages alter the length and “mucus escalator” does not work, so more particles are
18
Ch002-A04841.indd 18 9/13/2007 9:56:04 AM
CHAPTER
2
allowed to reach the alveoli, thereby predisposing the exist to safeguard airway patency and to prevent foreign
patient to chronic pulmonary inflammation.8 material from entering the lower respiratory tract, involve
Airway Management in the Critically Ill Adult
The larynx prevents food and other foreign bodies from the epiglottis, the vocal cords, and the sensory supply to
entering the trachea. Reflex closure of the glottic inlet the pharynx and larynx.10 Patients who can swallow
occurs during swallowing6 and periods of increased intra- normally have intact airway reflexes, and normal speech
thoracic (e.g., coughing, sneezing) or intra-abdominal makes absence of such reflexes unlikely. Patients with a
(e.g., vomiting, micturition) pressure. In unconscious decreased level of consciousness (LOC) should be assumed
patients, these reflexes are lost, so glottic closure may not to have inadequate protective reflexes.
occur, with an increased risk of pulmonary aspiration.
Inspired Oxygen Concentration
Oxygen demand is elevated by the increased work of
ASSESSING ADEQUACY OF THE AIRWAY breathing associated with respiratory distress11 and by
Adequacy of the airway should be considered in four the increased metabolic demands in critically ill or injured
aspects: patients. Often, higher inspired oxygen concentrations are
required to satisfy tissue oxygen demand and to prevent
■ Patency. Partial or complete obstruction will compro- critical desaturations during maneuvers for managing
mise ventilation of the lungs and likewise gas the airway. A cuffed ET, connected to a supply of oxygen,
exchange. is a sealed system in which the delivered oxygen concen-
■ Protective reflexes. These help maintain patency and tration also is the inspired concentration. A patient wearing
prevent aspiration of material into the lower airways. a facemask, however, inspires gas from the mask and sur-
■ Inspired oxygen concentration. Gas entering the pul- rounding ambient air. Because the patient will generate
monary alveoli must have an appropriate oxygen an initial inspiratory flow in the region of 30 to 60 L per
concentration. minute, and the fresh gas flow to a mask is on the order
■ Respiratory drive. A patent, secure airway is of little of 5 to 15 L per minute, much of the tidal inspiration will
benefit without the movement of gas between the be “room air” entrained from around the mask. The
atmosphere and the pulmonary alveoli effected through entrained room air is likely to dilute the concentration
the processes of inspiration and expiration. of oxygen inspired to less than 50%, even when 100%
oxygen is delivered to the mask.12 This unwelcome reduc-
Patency tion in inspired oxygen concentration can be combatted
Airway obstruction most frequently is due to reduced by (1) using a mask with a reservoir bag, (2) ensuring that
muscle tone, allowing the tongue to fall backwards against the mask is fitted firmly to the patient’s face, (3) using a
the postpharyngeal wall, thereby blocking the airway. high rate of oxygen flow to the mask (15 L per minute),
Loss of patency by this mechanism often occurs in an and (4) supplying a higher oxygen concentration. Even if
obtunded or anesthetized patient lying supine. Other 100% oxygen is delivered to such a system, the patient
causes include the presence of blood, mucus, vomitus, or may be inspiring significantly less than 50% oxygen.
a foreign body in the lumen of the airway or edema,
inflammation, swelling, or enlargement of the tissues Respiratory Drive
lining or adjacent to the airway. A patent, protected airway will not produce adequate
Upper airway obstruction has a characteristic presenta- oxygenation or excretion of carbon dioxide without ade-
tion in the spontaneously breathing patient: noisy inspira- quate respiratory drive. Changing arterial carbon dioxide
tion (stridor), poor expired airflow, intercostal retraction, tension (PCO2), by changing H+ concentration in cerebro-
increased respiratory distress, and paradoxical rocking spinal fluid (CSF), stimulates the respiratory center, which
movements of the thorax and abdomen.9 These resolve in turn controls minute volume and therefore arterial
quickly if the obstruction is removed. In total airway PCO2 (negative feedback).11,13 This assumes that increased
obstruction, sounds of breathing are absent entirely, owing respiratory drive can produce an increase in minute ven-
to complete lack of airflow through the larynx. Airway tilation (increased respiratory rate or tidal volume, or
obstruction may occur in patients with an endotracheal both, per breath), which may not occur if respiratory
tube (ET) or tracheostomy tube in situ due to mucous mechanics are disturbed. Brain injury and drugs such as
plugging or kinking of the tube or the patient’s biting opioids, sedatives, and alcohol are direct-acting respira-
down on a tube placed orally. If such patients are sponta- tory center depressants.
neously breathing, they will have the same symptoms Ventilation can be assessed qualitatively by looking,
and signs as just described. Patients on assisted (positive- listening, and feeling. In a spontaneously breathing patient,
pressure) breathing modes will have high inflation pres- listening to (and feeling) air movement while looking at
sures, decreased tidal and minute volumes, increased the extent, nature, and frequency of thoracic movement
end-tidal carbon dioxide levels, and decreased arterial will give an impression of ventilation. These parameters
oxygen saturation. may be misleading, however. Objective assessment of
minute ventilation requires PCO2 measurement in arterial
Protective Reflexes blood or monitoring of end-tidal carbon dioxide, which
The upper airway shares a common pathway with the can be used as a realtime measure of the adequacy of
upper gastrointestinal tract.6 Protective reflexes, which minute ventilation.13 If respiratory drive or minute venti-
19
Ch002-A04841.indd 19 9/13/2007 9:56:04 AM
PART
I
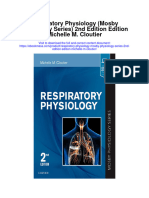
lation is inadequate, positive-pressure respiratory support ■ Venturi mask (C in Fig. 2-1)—a facemask with vents
may be required, and any underlying factors should be that entrain a known proportion of ambient air when
CRITICAL CARE PROCEDURES, MONITORING, AND PHARMACOLOGY
addressed if possible (e.g., depressant effect of sedatives a set flow of 100% oxygen passes through a Venturi
or analgesics). device.14 Thus, the inspired oxygen concentration
(usually 24% to 35%) is known.
MANAGEMENT OF THE AIRWAY Establishing a Patent and Secure Airway
The aims of airway management are to provide an ade- Establishing a patent and secure airway can be achieved
quate inspired oxygen concentration; to establish a patent, using simple airway maneuvers, further airway adjuncts,
secure airway; and to support ventilation if required. tracheal intubation, or a surgical airway.
Providing an Adequate Inspired Airway Maneuvers
Oxygen Concentration Simple airway maneuvers involve appropriate position-
Although oxygen can be administered via nasal cannula, ing, opening the airway, and keeping it open using artifi-
this method does not ensure delivery of more than 30% cial airways if needed.
to 40% oxygen (at most). Other disadvantages include
lack of humidification of gases, patient discomfort with Positioning for Airway Management
use of flow rates greater than 4 to 6 L per minute, and In the absence of any concerns about cervical spine stabil-
predisposition to nasal mucosal irritation and potential ity (e.g., with trauma, rheumatoid arthritis, or severe
bleeding.14 Therefore, despite being more intrusive for osteoporosis), raising the patient’s head slightly (5 to
patients, facemasks are superior for oxygen administra- 10 cm) by means of a small pillow under the occiput can
tion. The three main types of facemask are shown in help in airway management. This adjustment extends the
Figure 2-1: atlanto-occipital joint and moves the oral, pharyngeal, and
■ Anesthesia-type facemask (mask A in Fig. 2-1)—a solid laryngeal axes into better alignment, providing the best
mask (with no vents) with a cushioned collar to provide straight line to the glottis (“sniffing” position).15,16
a good seal. This is suitable for providing very high
oxygen concentrations (approaching 100%) because Clearing the Airway
entrainment is minimized and the anesthetic circuit Acute airway obstruction in the obtunded patient often
normally includes a reservoir of gas. They become due to the tongue or extraneous material—liquid (saliva,
unacceptable for many awake patients within a few blood, gastric contents) or solid (teeth, broken dentures,
minutes, because of the association with heat, mois- food) in the pharynx. In the supine position, secretions
ture, and claustrophobia. usually are cleared under direct vision using a laryngo-
■ Simple facemask—a facemask with vents that allow scope and a rigid suction catheter.17 In some cases, a
heat or humidity out but that also entrain room air. flexible suction catheter, introduced through the nose and
These masks have no seal and are relatively loose- nasopharynx, may be the best means of clearing the
fitting. Such masks may have a reservoir bag (approxi- airway. A finger sweep of the pharynx may be used to
mately 500 mL), sitting inferior to the mask (B2 in Fig. detect and remove larger solid material in unconscious
2-1), or have no reservoir (B1 in Fig. 2-1). Without a patients without an intact gag reflex. During all airway
reservoir bag, it is difficult to deliver an inspired oxygen interventions, if cervical spine instability cannot be
concentration of 50% even with tight application. ruled out, relative movement of the cervical vertebrae
must be prevented—most often by manual in-line
immobilization.17,18
Triple Airway Maneuver
The triple airway maneuver often is beneficial in obtunded
patients if it is not contraindicated by concerns about
cervical spine instability. As indicated by its name, this
maneuver has three components: head tilt (neck exten-
sion), jaw thrust (pulling the mandible forward), and
mouth opening.19 The operator stands behind and above
the patient’s head. Then the maneuver is performed as
follows:
■ Extend the patient’s neck with the operator’s hands
on both sides of the mandible.
■ Elevate the mandible with the fingers of both hands,
thereby lifting the base of the tongue away from the
Figure 2-1. Facemasks: anesthesia mask (A); simple posterior pharyngeal wall.
facemask (B1); simple facemask with reservoir bag (B2); ■ Open the mouth by pressing caudally on the ante-
Venturi mask (C). rior mandible with the thumbs or forefingers.
20
Ch002-A04841.indd 20 9/13/2007 9:56:04 AM
CHAPTER
2
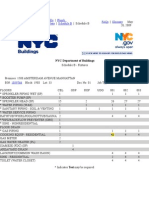
Artificial Airways useful in semiconscious patients in whom the gag reflex
If the triple airway maneuver or any of its elements is partially preserved. These artificial airways should be
Airway Management in the Critically Ill Adult
reduces airway obstruction, the benefit can be maintained considered to be a temporary adjunct—to be replaced
for a prolonged period by introducing an artificial airway with a more secure airway if the patient fails to improve
into the pharynx between the tongue and the posterior rapidly to the point at which an artificial airway no longer
pharyngeal wall (Fig. 2-2). is needed. Such airways should not be used in association
The oropharyngeal airway (OPA) is the most commonly with prolonged positive-pressure ventilation.
used artificial airway. Simple to insert, it is used temporar-
ily to help facilitate oxygenation or ventilation before Advanced Airway Adjuncts
tracheal intubation. The OPA should be inserted with the Advanced airway adjuncts fill the gap between simple
convex side toward the tongue and then rotated through airway maneuvers and the insertion of a tracheal tube or
180 degrees. Care must be taken to avoid pushing the surgical airway. These devices can be used to facilitate safe
tongue posteriorly, thereby worsening the obstruction. The reliable airway management and manual ventilation in
nasopharyngeal airway (NPA) has the same indications as the prehospital or emergency resuscitation setting, often
for the OPA but significantly more contraindications20 without expert medical presence.
(Box 2-1). It is better tolerated than the OPA, making it The laryngeal mask airway (LMA) is a small latex mask
mounted on a hollow plastic tube.121-126 It is placed
“blindly” in the lower pharynx overlying the glottis. The
inflatable cuff helps wedge the mask in the hypopharynx,
Box 2-1 sitting obliquely over the laryngeal inlet. Although the
LMA produces a seal that will allow ventilation with
Contraindications to Insertion of gentle positive pressure, it does not definitively protect
Oropharyngeal and Nasopharyngeal Airways the airway from aspiration. Indications for use of the LMA
Contraindications to Oropharyngeal Airways in critical care are (1) as an alternative to other artificial
Inability to tolerate (gagging, vomiting) airways, (2) the difficult airway, particularly the “can’t
Airway swelling (burns, toxic gases, infection) intubate–can’t ventilate” scenario, and (3) as a conduit for
Bleeding into the upper airway bronchoscopy. It is possible to pass a 6.0-mm ET through
Absence of pharyngeal or laryngeal reflexes a standard LMA into the trachea, but the LMA must be
Impaired mouth opening (e.g., with trismus or left in situ. The intubating LMA (ILMA), which was devel-
temporomandibular joint dysfunction) oped specifically to aid intubation with a tracheal tube,
has a shorter steel tube with a wider bore, a tighter curve,
Contraindications to Nasopharyngeal Airways and a distal silicone laryngeal cuff.27-30 A bar present near
Narrow nasal airway in young children the laryngeal opening is designed to lift the epiglottis
Blocked or narrow nasal passages in adults anteriorly. The ILMA allows the passage of a specially
Airway swelling (burns, toxic gases, infection) designed size 8.0 ET.
Bleeding into the upper airway The Combitube (esophageal-tracheal double-lumen
Absence of pharyngeal or laryngeal reflexes airway) is a combined esophageal obturator and tracheal
Fractures of the mid-face or base of skull tube, usually inserted blindly.31-35 Whether the “tracheal”
Clinical scenarios in which nasal hemorrhage would be lumen is placed in the trachea or esophagus, the Combi-
disastrous tube will allow ventilation of the lungs and give partial
protection against aspiration. The Combitube also is a
potential adjunct in the “cannot intubate–cannot venti-
late” situation. Disadvantages include the inability to
suction the trachea when the device is sitting in its com-
monest position (in the esophagus). Insertion also may
cause trauma, and the Combitube is contraindicated in
patients with known esophageal pathology or intact laryn-
geal reflexes and in persons who have ingested caustic
substances.
Tracheal Intubation
If the foregoing interventions are not effective or are
contraindicated, tracheal intubation is required. This
modality will provide (1) a secure, potentially long-term
airway; (2) a safe route to deliver positive-pressure venti-
lation if required; and (3) significant protection against
pulmonary aspiration. Orotracheal intubation is the most
widely used technique for clinicians practiced in direct
Figure 2-2. Artificial airways: oropharyngeal airway (OPA); laryngoscopy (indications and contraindications in Box
nasopharyngeal airway (NPA,); laryngeal mask airway (LMA). 2-2). Normally, anesthesia with or without neuromuscular
21
Ch002-A04841.indd 21 9/13/2007 9:56:05 AM
PART
I
Box 2-2 Box 2-3
CRITICAL CARE PROCEDURES, MONITORING, AND PHARMACOLOGY
Orotracheal Intubation: Indications and Procedure: Orotracheal Intubation
Relative Contraindications
■ Position patient and induce anesthesia ± neuromus-
Indications cular blockade (if needed).
Long-term correction or prevention of airway ■ Perform manual ventilation using triple airway
obstruction maneuver and oropharyngela airway.
Securing the airway and protecting against pulmonary ■ Hold laryngoscope handle (left hand) near the junc-
aspiration tion with blade.
Facilitating positive-pressure ventilation ■ Insert the blade along the right side of the tongue—
Enabling bronchopulmonary toilet moving tongue to the left.
Optimizing access to pharynx, face, or neck at ■ Advance tip of the blade in the midline between
surgery tongue and epiglottis.
■ Pull upwards and along the line of the handle of the
Contraindications (Relative)
laryngoscope.
Possibility of cervical spine instability
■ Lift the epiglottis upward and visualize the vocal
Impaired mouth opening (e.g., trismus, temporo-
cords.
mandibular joint dysfunction)
■ Do not use the patient’s teeth as a fulcrum when
Potential difficult airway
attempting to visualize the glottis.
Need for surgical immobilization of maxilla or mandible
■ Pass tracheal tube through the vocal cords into the
(wires, box frame)
trachea (right hand).
■ Stop advancing tube when cuff is 2 to 3 cm beyond
the cords.
blockade is necessary for this procedure, which is sum- ■ Connect to a bag-valve system and pressurize it by
marized in Box 2-3. squeezing bag.
Tracheal intubation requires lack of patient awareness ■ Inflate cuff until audible leak around tube stops.
(as in the unconscious state or with general anesthesia) ■ Check correct tube position (auscultation) and assess
and the abolition of protective laryngeal and pharyngeal cuff pressure.
reflexes. The drugs commonly used to achieve these states ■ Check end-tidal CO2 trace.
are shown in Table 2-1. Anesthesia is achieved using an
intravenous induction agent, although intravenous seda-
tives (e.g., midazolam) theoretically may be used. Opioids
often are used in conjunction with induction agents Table 2-1. Drugs Used to Facilitate Tracheal Intubation
because they may reduce the cardiovascular sequelae
Drug Dose (Intravenous)
of laryngoscopy and intubation (tachycardia and
hypertension) and also may contribute to the patient’s Induction Agent
unconsciousness. Propofol 1-2.5 mg/kg
Abolition of protective laryngeal and pharyngeal reflexes Opioids
sometimes is achieved by inducing a deep level of uncon- Fentanyl 1.0-1.5 µg/kg
Morphine 0.15 mg/kg
sciousness using one or more of the aforementioned agents,
followed by inhalation of high concentrations of a volatile Nondepolarizing Agents
anesthetic agent (e.g., sevoflurane, isoflurane). This tech- Atracurium 0.4-0.5 mg/kg
Vecuronium 0.1 mg/kg
nique sometimes is used in the difficult airway scenario Rocuronium 0.45-0.6 mg/kg
to obtain conditions suitable for tracheal intubation in a
Depolarizing Agent
patient who is still breathing spontaneously.
Succinylcholine (suxamethonium) 1.0-1.5 mg/kg
More usually, a muscle relaxant is used to abolish the
protective reflexes, abduct the vocal cords, and facilitate
tracheal intubation. In the elective situation, nondepolar-
izing neuromuscular blocking agents are used. These have Nasotracheal intubation shares the problems and con-
the disadvantage of requiring several minutes to exert traindications associated with the nasopharyngeal airway.20
their effect, during which the patient must receive ventila- The technique usually is employed when there are relative
tion via a mask, thus allowing the possibility of gastric contraindications to the oral route (e.g., anatomic abnor-
dilation and pulmonary aspiration. In patients at high risk malities, cervical spine instability). Nasotracheal intuba-
of the latter (e.g., nonfasting patients), a depolarizing tion may be achieved under direct vision or with use of
muscle relaxant (succinyl choline) is used because it pro- a blind technique, either with the patient under general
duces suitable conditions for intubation within 15 to 20 anesthesia or in the awake or lightly sedated patient with
seconds, and mask ventilation is not required. Succinyl- appropriate local anesthesia (Table 2-2). If orotracheal or
choline has several side effects—among them hyperkale- nasotracheal intubation is required but cannot be achieved,
mia, muscle pains and (rarely) malignant hyperpyrexia. then a surgical airway is required (see later).
22
Ch002-A04841.indd 22 9/13/2007 9:56:06 AM
CHAPTER
2
Table 2-2. Procedure: Nasotracheal Intubation (Blind and under Direct Vision)
Airway Management in the Critically Ill Adult
Prepare and Assess the Patient
1. Use a nasal decongestant such as phenylephrine to reduce bleeding
2. Provide local anaesthesia to nasal mucosa
3. Examine each nostril for patency and deformity
4. Choose the most patent nostril and choose appropriate sized ET
5. After induction of anaesthesia, position as for oral intubation
Blind Nasotracheal Intubation Nasotracheal Intubation (Direct Vision)
Keep patient breathing spontaneously. Patient may be apneic with or without relaxants.
Insert well-lubricated ET into the nostril (concavity forward, Gently advance ET through the nose.
bevel lateral). When ET tip is in oropharynx, perform laryngoscopy.
While passing ET along nasal floor, listen for audible Visualize ET in pharynx and advance toward glottis.
breathing through the tube. Advance ET through cords into trachea, under direct
Advance ET, rotating as needed to maintain clear breath vision if possible.
sounds. Use Magill forceps if required to guide tip while
ET will pass through cords, and patient may cough. advancing ET.
Technique takes time so it is not suitable for a Try to avoid damaging cuff if using forceps to help
desaturating patient. passage through cords.
Do not force passage of ET because this could cause bleeding.
With a need for isolation of one lung from another, a ble upward toward the mask with the other three fingers.
double-lumen tube (having one cuffed tracheal lumen and The other hand is used to squeeze the reservoir bag, gen-
one cuffed bronchial lumen fused longitudinally) can be erating positive pressure. Excessive pressure from the C-
used.36 The main indications are (1) to facilitate some grip on the mask may lead to backward movement of the
pulmonary or thoracic surgical procedures; (2) to isolate mandible with subsequent airway obstruction, or a tilt of
a lung containing contaminated fluid (e.g., in lung abscess) the mask with leakage of gas. If a proper seal is difficult
or blood, thereby preventing contralateral spread; and (3) to attain, placing a hand on each side of the mask and
to enable differential or independent lung ventilation mandible is advised, with a second person manually com-
(ILV). ILV allows each lung to be treated separately—for pressing the reservoir bag (four-handed ventilation). Bag-
example, to deliver positive-pressure ventilation with high valve-mask systems have a self-reinflating bag, which
positive end-expiratory pressure (PEEP) to one lung while springs back after compression, thereby drawing gas in
applying low levels of continuous positive airway pressure through a port with a one-way valve. It is important
(CPAP) only to the other. Such a strategy may be advanta- to have a large reservoir bag with a continuous flow of
geous in cases of pulmonary air leak (bronchopleural oxygen attached to this port in order to ensure a high
fistula, bronchial tear, or severe lung trauma) or in severe inspired oxygen concentration.39,40 Bag-valve-mask venti-
unilateral lung disease requiring ventilatory support.37,38 lation usually is a short-term measure in urgent situations
or is used in preparation for tracheal intubation.
Providing Ventilatory Support
If a patient has no (or inadequate) spontaneous ventila- Prolonged Ventilation Using a Sealed Tube in
tion, then a means of generating gas flow to the lower the Trachea
respiratory tract must be provided. Negative pressure, Ventilation of the lungs with a bag-valve-mask arrange-
mimicking the actions of the respiratory muscles, occa- ment is difficult if required for more than a few minutes or
sionally is used in some patients who require long-term if the patient needs to be transported. In these instances,
ventilation. In acute care, however, ventilation is achieved ventilation through a sealed tube in the trachea is indi-
using positive pressure, which requires an unobstructed cated. Orotracheal or nasotracheal intubation, surgical cri-
airway; in the nonintubated patient, this is best achieved cothyrotomy, and tracheostomy all achieve the same result:
by proper positioning, the triple airway maneuver, and a cuffed tube in the trachea, allowing the use of positive-
use of an OPA or NPA. In a patient without an ET in pressure ventilation and protecting the lungs from aspira-
place, particularly if some degree of airway obstruction tion. Mechanical ventilation is discussed in Chapter 9.
exists, positive-pressure ventilation often will cause gastric
distention and (potentially) regurgitation and pulmonary Apneic Oxygenation
aspiration. Apneic oxygenation is achieved using a narrow catheter
that sits in the trachea and carries a flow of 100% oxygen.
Bag-Valve-Mask Ventilation The catheter may be passed into the trachea via an ET or
Ventilation with a mask requires an (almost) airtight fit under direct vision through the larynx. This apparatus can
between mask and face. This is best achieved by firmly be set up as a low-flow open system (gas flow rate of 5
pressing the mask against the patient’s face using the to 8 L per minute) or as a high-pressure (jet ventilation)
thumb and index finger (C-grip) while pulling the mandi- system41 and can be used to maintain oxygenation with a
23
Ch002-A04841.indd 23 9/13/2007 9:56:06 AM
PART
I
difficult airway either at intubation or at extubation (see geal cartilages). Dislodged structures such as teeth or den-
later). tures may be aspirated, blocking the airway more distally.
CRITICAL CARE PROCEDURES, MONITORING, AND PHARMACOLOGY
Less common complications include perforation of the
airway with the potential for the development of a retro-
PHYSIOLOGIC SEQUELAE pharyngeal abscess or mediastinitis. Over time, erosions
AND COMPLICATIONS OF due to pressure and ischemia may develop on the lips or
TRACHEAL INTUBATION tongue (or external nares and anterior nose in patients
Laryngoscopy is a noxious stimulus that, in an awake with a nasotracheal tube) and in the larynx or upper
or lightly sedated patient, would provoke coughing, retch- trachea.44 These lesions result in a breach of the mucosa
ing, or vomiting and laryngospasm. In clinical practice, with the potential for secondary infection. In the case of
however, laryngoscopy and tracheal intubation usually are the lips and tongue, such lesions are (temporarily) disfig-
performed after induction of anesthesia, and in emer- uring and painful and may inhibit attempts to talk or
gency situations, the patient often is hypoxic and hyper- swallow.
carbic, with increased sympathetic nervous system activity The mucosa of the upper trachea (subglottic area) is
(SNA). Thus, the physiologic effects of laryngoscopy and subjected to the pressure of the cuff of the ET. This pres-
tracheal intubation tend to be masked. sure reduces perfusion of the tracheal mucosa and, com-
Laryngoscopy and intubation cause an increase in cir- bined with the mechanical movement of the tube (from
culating catecholamines and increased SNA, leading to patient head movements, nursing procedures, or rhythmic
hypertension and tachycardia. This represents an increase flexion with action of the ventilator), tends to cause
in myocardial work and myocardial oxygen demand, mucosal damage and increase the risk of superficial infec-
which may provoke cardiac dysrhythmias and myocardial tion. These processes may lead to ulceration of the tra-
hypoxia or ischemia. Laryngoscopy increases cerebral cheal mucosa, fibrous scarring, contraction, and ultimately
blood flow and intracranial pressure—particularly in stenosis, which can be a life-limiting or life-threatening
patients who are hypoxic or hypercarbic at the time of problem. Although irrefutable evidence is lacking, most
intubation.42 This rise in intracranial pressure will be exag- clinicians believe that limiting the period of orotracheal
gerated if cerebral venous drainage is impeded by violent or nasotracheal intubation and reducing cuff pressures
coughing, bucking, or breath-holding. may reduce the frequency of this complication.44
Coughing and laryngospasm occur frequently in patients Any tube in the trachea has a significant effect on the
undergoing laryngoscopy and intubation when muscle mechanisms protecting the airway from aspiration and
relaxation and anesthesia are inadequate. Increased bron- infection. The mucus escalator may be inhibited by
chial smooth muscle tone, which increases airway resis- mucosal injury and by the lack of warm humidified airflow
tance, may occur as a reflex response to laryngoscopy or over the respiratory epithelium.45 The disruption of normal
may be due to the physical presence of the ET in the swallowing results in the pooling of saliva and other
trachea; in its most severe form, termed bronchospasm, debris in the pharynx and larynx above the upper surface
this increased tone causes audible wheeze and ventilatory of the tube’s inflatable cuff, which may become the source
difficulty. Increased resistance to gas flow will occur of respiratory infection if the secretions become colonized
because the cross-sectional area of the ET is less than with microorganisms, or may pass beyond the cuff into
that of the airway. This difference usually is unimportant the lower airways—that is, pulmonary aspiration (silent
with positive-pressure ventilation but causes a significant or overt).46,47 The former may occur due to (1) coloniza-
increase in work of breathing in spontaneously breathing tion of the gastric secretions and the regurgitation
patients. Resistance is directly related to 1/r4 (where r is of this material up the esophagus to the pharynx or (2)
the radius of the ET) and will be minimized by use of a transmission of microorganisms from the health care envi-
large-bore ET. Gas passing through an ET, bypassing the ronment to the pharynx via medical equipment or the
nasal cavity, also loses the beneficial effects of warming, hands of hospital staff or visitors (cross-infection).45,47-50
humidification, and the addition of traces of nitric oxide The presence of a tube traversing the larynx and sealing
(NO).43 the trachea makes phonation impossible. The implications
The effects of intubation on functional residual capacity of this limitation for patients and their families often are
(FRC) are complex. In patients under anesthesia, a fall in ignored. If patients cannot tell caregivers about pain,
FRC is well documented. This decrease may be due to the nausea, or other concerns, they may become frustrated,
loss of respiratory muscle tone following induction of agitated, or violent. This may result in the excessive use
anesthesia and the relatively unopposed effect of the of sedative or psychoactive drugs, which prolong time on
elastic recoil in the lungs.43 The increased resistance to gas ventilation and stay in the intensive care unit (ICU), with
flow due to the presence of the ET may slow expiration, the risk of infection increased accordingly.51 The inability
producing intrinsic PEEP (and therefore an increase in to communicate may therefore be a real threat to patient
FRC) if the next inspiration begins before expiration is survival. Potential solutions involve the use of letter and
complete. picture boards, “speaking valves” (with tracheostomy),
Laryngoscopy and intubation may cause bruising, abra- laryngeal microphones, or computer-based communica-
sion, laceration, bleeding or displacement or dislocation tion packages. The involvement and innovations of disci-
of the structures in and near the airway (e.g., lips, teeth plines such as the speech and language center may be
or dental prostheses, tongue, epiglottis, vocal cords, laryn- advantageous.
24
Ch002-A04841.indd 24 9/13/2007 9:56:06 AM
CHAPTER
65-67
2
THE DIFFICULT AIRWAY related, and such incidents may occur at intubation,
at extubation, or during the course of treatment (as with
Airway Management in the Critically Ill Adult
The difficult airway has been defined as “the clinical
the acutely displaced or obstructed ET or tracheostomy
situation in which a conventionally trained anesthetist
tube).
experiences difficulty with mask ventilation of the upper
airway, tracheal intubation, or both.”52 It has been a com-
monly documented cause of adverse events including Recognizing the Potentially
airway injury, hypoxic brain injury, and death under anes- Difficult Airway
thesia.53-59 The frequency of difficulty with mask ventila- Many conditions are associated with airway difficulty
tion has been estimated to be between 1.4% and 7.8%,60-62 (Table 2-3), including anatomic abnormalities, which may
while tracheal intubation using direct laryngoscopy is result in an unusual appearance, thereby alerting the
difficult in 1.5% to 8.5% and impossible in up to 0.5% examiner. The goal is to identify the potentially difficult
of general anesthetics.58,63 The incidence of failed intuba- airway and develop a plan to secure it. Factors including
tion is approximately 1 : 2000 in the nonobstetric popula- age older than 55 years, body mass index greater than
tion and 1 : 300 in the obstetric population.64 In the critical 26 kg/m2, presence of a beard, lack of teeth, and a history
care unit, up to 20% of all critical incidents are airway of snoring have been identified as independent variables
Table 2-3. Conditions Associated with Difficult Airway
Causative Factor Associated Conditions/Disorders
Abnormal facial anatomy/development Small mouth and/or large tongue
Dental abnormality
Prognathia
Obesity
Advanced pregnancy
Acromegaly
Congenital syndromes*
Inability to open mouth Masseter muscle spasm (dental abscess)
Temporomandibular joint dysfunction
Facial burns
Postradiotherapy fibrosis
Scleroderma
Cervical immobility/abnormality Short neck/obesity
Poor cervical mobility (e.g., ankylosing spondylitis)
Previous cervical spine surgery
Presence of cervical collar
Postradiotherapy fibrosis
Pharyngeal or laryngeal abnormality High or anterior larynx
Deep vallecula: inability to reach base of epiglottis with blade of scope
Anatomic abnormality of epiglottis or hypopharynx (e.g., tumor)
Subglottic stenosis
Injury Traumatic debris
Obstructing foreign bodies
Basilar skull fracture
Bleeding into airway or adjacent swelling/hematoma
Fractured maxilla/mandible
Cervical spine instability (confirmed or potential)
Laryngeal fracture or disruption
Infections Epiglottitis
Abscess
Croup, brochiolitis
Laryngeal papillomatosis
Tetanus—trismus
Connective tissue/inflammatory Rheumatoid arthritis—temporomandibular joint or cervical spine involvement,
cricoarytenoid arthritis
Ankylosing spondylitis
Scleroderma
Sarcoidosis
Endocrine disorders Goiter: airway compression or deviation
Hypothyroidism, acromegaly: large tongue
*Visit http://www.erlanger.org/craniofacial and http://www.faces-cranio.org for specific details.
Data from Criswell JC, Parr MJA, Nolan JP: Emergency airway management in patients with cervical spine injuries. Anaesthesia 1994;49:900-903;
and Morikawa S, Safar P, DeCarlo J: Influence of head position upon upper airway patency. Anaesthesiology 1961;22:265.
25
Ch002-A04841.indd 25 9/13/2007 9:56:06 AM
PART
I
predicting difficulty with mask ventilation—in turn asso- 15% of severely injured patients have maxillofacial
ciated with difficult tracheal intubation.61,68 involvement, and 5% to 10% of patients with blunt
CRITICAL CARE PROCEDURES, MONITORING, AND PHARMACOLOGY
Mallampati69 developed a grading system (subsequently trauma have an associated cervical spine injury (often
modified64) that predicted ease of tracheal intubation at associated with head injury).80
direct laryngoscopy. The predictive value of the Mallam- Problems encountered in trauma patients include pres-
pati system has been shown to be limited70,71 because ence in the airway of debris or foreign bodies (e.g., teeth),
many factors that have no influence on the Mallampati vomitus, or regurgitated gastric contents; airway edema;
classification—mobility of head and neck, mandibular tongue swelling; blood and bleeding; and fractures (maxilla
or maxillary development, dentition, compliance of neck and mandible). Patients must be assumed to have a full
structures, and body shape—can influence laryngeal stomach (requiring bimanual cricoid pressure and a rapid-
view.53,66,72,73 A study of a complex system including some sequence induction for intubation) and many will have
of these factors found the rate of difficult intubation to be pulmonary aspiration before the airway in secured. An
1.5%, but with a false-positive rate of 12%.74 A risk index important consideration in most cases is the need to avoid
based on the Mallampati classification, a history of diffi- movement of the cervical spine at laryngoscopy or intuba-
cult intubation, and five other variables lacked sufficient tion.17,18 Direct injury to the larynx is rare but may result
sensitivity and specificity.75 Airway management should in laryngeal disruption, producing progressive hoarseness
be based on the fact that the difficult airway cannot be and subcutaneous emphysema. Tracheal intubation, if
reliably predicted.76,77 This is a particularly important con- attempted, requires great care and skill because it may
sideration in the critical care environment. cause further laryngeal disruption. With Le Fort fractures,
airway obstruction or compromised respiration requiring
The Obstructed Airway immediate airway control is present in 25% of cases.81
Although the most common reason for an obstructed Postoperative bleeding after operations to the neck
airway in the un-intubated patient is posterior displace- (thyroid gland, carotid, larynx) may compress or displace
ment of the tongue in association with a depressed level the airway, leading to difficulty in intubation.
of consciousness, it is the less common causes that provide
the greatest challenges. It is important to elucidate the The Airway Practitioner and
level at which the obstruction occurs and the nature of the Clinical Setting
the obstructing lesion. This may be due to infection or Although airway difficulties often are due to anatomic
edema (epiglottis, pharyngeal or tonsillar abscess, medi- factors as discussed, it is important to recognize that the
astinal abscess), neoplasm (primary malignant or benign inability to perform an airway maneuver also may be due
tumor, metastastic spread, direct extension from nearby to a practitioner’s inexperience or lack of skill.82-87 Expert
structures), thyroid enlargement, vascular lesions, trauma, opinion and clinical evidence also identify lack of skilled
or foreign body or impacted food.14,78 assistance as a factor in airway-related adverse events.88-91
Airway lesions above the level of the vocal cords are As might be expected, inexperience and lack of suitable
considered to lie in the upper airway and commonly help may contribute to failure in optimizing the conditions
manifest with stridor.79 If breathing is labored and associ- for laryngoscopy (Box 2-4). Airway and ventilatory man-
ated with difficulties at night, rather than just noisy, then agement performed in the prehospital setting or in the
the narrowing probably is more than 50%. Patients with hospital but outside an operating room (OR) carries a
these lesions usually fall into one of two groups: (1) those higher frequency of adverse events and a higher mortality
who can be intubated, usually under inhalational induc- rate when compared with anesthesia in an OR.92-96 In the
tion, with the ENT surgeon immediately available to critical care unit, all invasive airway maneuvers are poten-
perform rigid bronchoscopy or tracheostomy if required, tially difficult.97 Positioning is more difficult on an ICU bed
or (2) those who require a tracheostomy placed using than on an OR table. The airway structures may be edema-
local anesthesia. In patients with mid-tracheal obstruc- tous after previous laryngoscopy or presence of an ET.
tion, CT imaging usually is necessary to discover the exact Neck immobility, or the need to avoid movement in a
level and nature of the obstruction and to allow planning
of airway management for nonemergency clinical presen-
tations.79 Tracheostomy often is not beneficial because the Box 2-4
tube may not be long enough to bypass the obstruction.
In such instances, fiberoptic intubation often may be Common Errors Compromising
useful.79 Lower tracheal obstruction often is due to space- Successful Intubation
occupying lesions in the mediastinum and necessitates ■ Poor patient positioning
multidisciplinary planning involving ENT, cardiothoracic ■ Failure to ensure appropriate assistance
surgery, anesthesia, and critical care. ■ Faulty light source in laryngoscope or no alternative
scope
Trauma and the Airway ■ Failure to use a longer blade in appropriate
Airway management in the trauma victim provides patients
additional challenges because the victim often has other ■ Use of inappropriate tracheal tube (size or shape)
life-threatening conditions and preparation time for man- ■ Lack of immediate availability of airway adjuncts
agement of the difficult airway is limited. Approximately
26
Ch002-A04841.indd 26 9/13/2007 9:56:06 AM
CHAPTER
2
potentially unstable cervical spine, may be other contrib-
Box 2-5
uting factors.98-100 Poor gas exchange in ICU patients
Airway Management in the Critically Ill Adult
reduces the effectiveness of preoxygenation and increases Indications for Fiberoptic Intubation
the risk of significant hypoxia before the airway is
secured.101 Cardiovascular instability may produce hypo- ■ Anticipated difficult intubation
tension or hypoperfusion, or may lead to misleading oxim- ■ Avoidance of dental damage in high-risk patient
etry readings (including failure to record any value at all), ■ Direct laryngeal trauma
a further confounding factor for the attending staff.102,103 ■ Other need for awake intubation
Managing the Difficult Airway
Management of the difficult airway can be considered in
the framework of three possible clinical scenarios with the trachea, and the endoscope is withdrawn. An informed
progressively increasing risks for the patient: (1) the antic- patient, trained assistance, and adequate preparation time
ipated difficult airway; (2) the unanticipated difficult make fiberoptic intubation less stressful. The nasotracheal
airway; and (3) the difficult airway resulting in a “cannot route is used most often and requires the use of nasal
intubate and cannot ventilate” situation. vasoconstrictors. Nebulized local anesthetic is delivered
Requirements for clinicians involved in airway manage- to the airway via facemask. Sedation may be given, but
ment include the following: ideally the patient should remain breathing spontaneously
and responsive to verbal commands. The procedure often
■ Expertise in recognition and assessment of the poten- is time-consuming and tends to be used in elective situa-
tially difficult airway. This involves the use of the tions107 (Box 2-5).
assessment techniques above and a “sixth sense.”76
■ The ability to formulate a plan (with alterna- Retrograde Intubation For retrograde intubation,108,109
tives).52,53,104-106 local anesthesia is provided and the cricothyroid mem-
■ Familiarity with algorithm(s) that outline a sequence brane is punctured by a needle through which a wire or
of actions designed to maintain oxygenation, ventila- catheter is passed upward through the vocal cords. When
tion, and patient safety. The ASA guidelines52 and the it reaches the pharynx, the wire is visualized, brought out
composite plan from the Difficult Airway Society through the mouth, and then used to guide the ET through
(DAS)104 are shown in Figures 2-3 and 2-4. The latter the vocal cords before it is withdrawn. This technique also
summarizes four airway plans (A-D), available from can be used to guide a fiberoptic scope through the vocal
the DAS website (www.das.uk.com). cords. Owing to time constraints, it is not suitable
■ The skills and experience to use a number of airway for emergency airway access and is contraindicated in
adjuncts, particularly those relevant to the unantici- any patient with an expanding neck hematoma or
pated difficult airway. coagulopathy.
The Anticipated Difficult Airway Intubation under Anesthesia
The anticipated difficult airway is the “least lethal” of the It may be decided, in spite of the safety advantage of
three scenarios—with time to consider strategy, optimize awake intubation, to anesthetize the patient before
patient status, and obtain appropriate adjuncts and per- attempted intubation. Preparation of the patient, equip-
sonnel. The key questions are as follows: ment, and staff is paramount (Box 2-6). Adjuncts such
as those described later should be available, either to
1. Should the patient be kept awake or be anesthetized improve the chances of intubation or to provide a safe
for intubation? alternative airway if intubation cannot be achieved.
2. Which technique should be used for intubation?
Unanticipated Airway Difficulty
Awake Intubation
The unanticipated difficult airway allows only a short
Awake intubation is more time-consuming, requires expe-
period to solve the problem if significant hypoxemia,
rienced personnel, is less pleasant for the patient (com-
hypercarbia, and hemodynamic instability are to be
pared with intubation under anesthesia), and may have
avoided. The patient usually is anesthetized, may be
to be abandoned as a result of the patient’s inability or
apneic, and may have received muscle relaxants, and pre-
unwillingness to cooperate. Because spontaneous breath-
vious initial attempt(s) at intubation may have been
ing and pharyngeal or laryngeal muscle tone is main-
unsuccessful. If appropriate equipment, assistance, and
tained, however, it is significantly safer. The techniques
experience are not immediately to hand, little time is
available are fiberoptic and retrograde intubation. It also
available to obtain them. Nevertheless, it is essential to
may be used in patients judged to be at risk for a difficult
maintain oxygenation and avoid hypercarbia if possible—
airway, whereupon an initial direct laryngoscopic view
commonly by mask ventilation with 100% oxygen. The
allows intubation.
four-handed technique often is used.
Fiberoptic Intubation Fiberoptic intubation is a tech- If the practitioner is inexperienced, if the patient has
nique in which a flexible endoscope with a tracheal tube had no (or a relatively short-acting) muscle relaxant, and
loaded along its length is passed through the glottis. The if ventilation is not a problem, it may be appropriate to
tracheal tube is then pushed off the endoscope and into let the patient recover consciousness. An awake intubation
27
Ch002-A04841.indd 27 9/13/2007 9:56:06 AM
PART
I
DIFFICULT AIRWAY ALGORITHM
1. Assess the likehood and clinical impact of basic management problems:
CRITICAL CARE PROCEDURES, MONITORING, AND PHARMACOLOGY
• Difficult ventilation
• Difficult intubation
• Difficulty with patient cooperation or consent
• Difficult tracheostomy
2. Actively pursue opportunities to deliver supplemental oxygen throughout the process of difficult airway management.
3. Consider the relative merits and feasibility of basic management choices:
A. Awake Intubation vs. Intubation Attempts after Induction of
General Anesthesia
B. Noninvasive Technique for Initial vs. Invasive Technique for Initial
Approach to Intubation Approach to Intubation
C. Preservation of Spontaneous Ventilation vs. Ablation of Spontanous Ventilation
4. Develop primary and alternative strategies:
A. AWAKE INTUBATION B. INTUBATION ATTEMPTS AFTER
INDUCTION OF GENERAL ANESTHESIA
Airway Approached by Invasive
Noninvasive Intubation Airway Access(b)* Initial Intubation Initial Intubation
Attempts Successful* Attempts Unsuccessful
Succeed* Fail FROM THIS POINT
ONWARD, CONSIDER:
Cancel Consider Feasibility Invasive 1. Calling for help
Case of Other Options(a) Airway Access(b)* 2. Returning to spontaneous
ventilation
3. Awakening the patient
Face mask ventilation adequate Face mask ventilation not adequate
Consider/attempt LMA
LMA adequate* LMA not adequate
or not feasible
Nonemergency pathway Emergency pathway
Ventilation Adequate, Intubation Unsuccessful Ventilation Not Adequate, Intubation Unsuccessful
IF BOTH
FACE MASK
Alternative Approaches Call for Help
AND LMA
to Intubation(c)
VENTILATION
Emergency Noninvasive Airway Ventilation(e)
BECOME
Successful Fail After INADEQUATE
Ventilation* Multiple Attempts Successful Ventilation* Fail
Emergency
Invasive Consider Feasibility Awaken Invasive Airway
Airway Access(b)* of Other Options(a) Patient(d) Access(b)*
* Confirm ventilation, tracheal intubation, or LMA placement with exhaled CO2.
a. Other options include (but are not limited to) surgery utilizing face c. Alternative noninvasive approaches to difficult intubation include
mask or LMA anesthesia, local anesthesia infiltration, and regional (but are not limited to) use of different laryngoscope blades, LMA
nerve blockade. Pursuit of these options usually implies that mask as an intubation conduit (with or without fiberoptic guidance),
ventilation will not be problematic. Therefore, these options may be fiberoptic intubation, intubating stylet or tube changer, light wand,
of limited value if this step in the algorithm has been reached via retrograde intubation, and blind oral or nasal intubation.
the Emergency Pathway. d. Consider re-preparation of the patient for awake intubation or
b. Invasive airway access includes surgical or percutaneous canceling surgery.
tracheostomy and cricothyrotomy. e. Options for emergency noninvasive airway ventilation include (but
are not limited to) rigid bronchoscope, esophageal-tracheal
Combitube ventilation, and transtracheal jet ventilation.
Figure 2-3. Algorithm for managing the difficult airway. (Adapted from Practice guidelines for management of the difficult
airway: An updated report by the American Society of Anesthesiologists Task Force on Management of the Difficult Airway.
Anaesthesia 2003;98:1269.)
can then be planned either after a short period of recov- when it has been decided to intubate with the patient
ery or on another occasion. With an experienced practi- under anesthesia.
tioner, it may be appropriate to continue, using techniques
to improve the chances of visualizing and intubating the Bimanual Laryngoscopy
larynx. As discussed next, various adjuncts may be useful Application of pressure on the cricoid area or the upper
in this situation and also in the anticipated difficult airway anterior tracheal wall, or both, by the laryngoscopist (a
28
Ch002-A04841.indd 28 9/13/2007 9:56:06 AM
CHAPTER
Figure 2-4. A four-
2
Plan A:
succeed component algorithm
Airway Management in the Critically Ill Adult
Initial tracheal Direct laryngoscopy Tracheal intubation
intubation plan for managing the
failed intubation difficult airway. (From
Difficult Airway
Society: Difficult Airway
Plan B: Confirm—then fiberoptic Society Composite Plan.
succeed
Secondary tracheal ILMA or LMA tracheal intubation through
Anaesthesia 2004;59:
intubation plan ILMA or LMA
failed oxygenation 675-694.)
failed intubation
Plan C:
Maintenance of oxygenation, Revert to face mask succeed Postpone surgery
ventilation; postponement of Oxygenate & ventilate Awaken patient
surgery and awakening
failed oxygenation
Plan D: improved
Rescue techniques oxygenation
LMA Awaken patient
for “can’t intubate–
can’t ventilate” situation increasing hypoxemia
or
Cannula cricothyrotomy Surgical cricothyrotomy
fail
technique sometimes termed bimanual laryngoscopy) may
Box 2-6
improve laryngeal view.110,111 When the view is optimized,
Checklist for Anticipated Difficult Intubation of an assistant maintains the pressure and thus the position
Patient under General Anesthesia of the larynx, freeing the hand of the laryngoscopist to
perform the intubation. The use of “blind” cricoid pressure,
Prepare and assess the patient. or BURP (backward, upward, and rightward pressure), by
Prepare and test the equipment. an assistant may impair laryngeal visualization.112-114
Ensure skilled assistance with knowledge of BURP/
bimanual laryngoscopy. Stylet (“Introducer”) and Gum Elastic Bougie
Have available: The stylet is a smooth, malleable metal or plastic rod that
A range of tracheal tubes lubricated and cuffs tested is placed inside an ET to adjust the curvature—typically
for patency (women: 7.0 to 7.5 mm in internal into a J or hockey-stick shape to allow the tip of the ET
diameter; men: 7.5 to 9.0 mm in internal tube to be directed through a poorly visualized or unseen
diameter). glottis.115 The stylet must not project beyond the end of the
Endotracheal tube stylets ET, to avoid potential laceration or perforation of the
Laryngeal mask airway (LMA) airway.
A range of laryngoscopes including specialized The gum elastic bougie is a blunt-ended, malleable rod
blades and handles which at direct laryngoscopy may be passed through the
poorly or nonvisualized larynx by putting a J-shaped bend
Check battery and bulb function. at the tip and passing it blind in the mid-line upward
Check functioning of suction devices. beyond the base of the epiglottis. Then, keeping the laryn-
Use optimal patient position. goscope in the same position in the pharynx, the ET can
Preoxygenation with 100% oxygen for 3 to 5 minutes be “railroaded” over the bougie, which is then withdrawn.
if possible For many critical care practitioners, it is the first-choice
Provide other equipment as desired: adjunct in the difficult intubation situation.111,116
Gum elastic bougie*
Lighted stylet* Different Laryngoscope or Blade
Combitube* Greater than 50 types of curved and straight laryngoscope
Intubating LMA* blades are available, the most commonly used being the
Fiberoptic scope* curved Macintosh blade.20 Using specific blades in certain
circumstances has been both encouraged117-119 and dis-
*Depending on choice of individual practitioner.
couraged.120 In patients with a large lower jaw or “deep
BURP, backward, upward, and rightward pressure. pharynx,” the view at laryngoscopy is often improved
significantly, by using a size 4 Macintosh blade (rather
than the more common adult size 3). This ensures the tip
of the blade can reach the base of the vallecula to lift the
29
Ch002-A04841.indd 29 9/13/2007 9:56:06 AM
PART
I
epiglottis. Other blades, such as the McCoy, may be Cannot Intubate/Cannot Ventilate
advantageous in specific situations.121,122
CRITICAL CARE PROCEDURES, MONITORING, AND PHARMACOLOGY
Help
Lighted Stylet Additional personnel needed for
ventilation, for bimanual laryngoscopy,
A lighted stylet (light wand) is a malleable fiberoptic light and as runner/communicator
source that can be passed along the lumen of an ET to (at least 2 others preferred)
facilitate blind intubation by transillumination. It allows
the tracheal lumen to be distinguished from the (more
posterior) esophagus on the basis of the greater intensity Oxygenate
Oral/nasal airway
of light visible through anterior soft tissues of the neck as Good seal (two hands)
the ET passes beyond the vocal cords.123 In elective anes- Ventilate with 100% O2
thesia, the intubation time and failure rate with light Speak calmly and quietly
wand–assisted intubation were similar to those with direct
laryngoscopy,124 and in a large North American survey, the
light wand was the preferred alternative airway device in Last laryngoscopy
Good light/blade
the difficult intubation scenario.125 A potential disadvan- Best position
tage is the need for low ambient light, which may not be Gum elastic bougie
desirable (or easily achieved) in a critical care setting. Bimanual laryngoscopy
Fiberoptic Intubation
LMA
The fiberoptic bronchoscope can be used in the unantici- or ILMA or Combitube
pated difficult airway if it is readily available and the Insert and attempt ventilation
operator is skilled.58,126,127 With an anesthetized patient,
the technique may be more difficult. Loss of muscle tone
will tend to allow the epiglottis and tongue to fall back Surgical airway
against the pharyngeal wall. This can be counteracted by Bag ventilation—if beneficial
Cricothyrotomy—needle or surgical
lifting the mandible. Ventilate with O2
Awaken patient
Cannot Intubate–Cannot Ventilate
Figure 2-5. Flow chart for the cannot intubate–cannot
“Cannot intubate–cannot ventilate” is an uncommon but
ventilate scenario.
life-threatening situation best managed by adherence to an
appropriate algorithm.52,53,104 All personnel involved will be
pressured (and motivated) by the potential for severe injury also may occur with esophageal intubation. The absence of
to the patient. Efficient teamwork will be more likely in an water vapor usually is indicative of esophageal intubation.
environment that is relatively calm. Although it may be Auscultation of breath sounds (in both axillae) supports
difficult, shouting, impatience, anger, and panic should be correct tube positioning but is not absolute confirmation.130
avoided in such situations. Figure 2-5 presents a simple Apparent inequality of breath sounds heard in the axillae
flow sheet summarizing the appropriate actions.128 may suggest intubation of a bronchus by an ET which has
passed beyond the carina. Of note, after emergency intuba-
tion and clinical confirmation of the ET in the trachea, 15%
CONFIRMING TUBE POSITION IN of ETs may still be inappropriately close to the carina.131
THE TRACHEA The use of capnography to detect end-tidal carbon
A critical factor in the difficult airway scenario, poten- dioxide is the most reliable objective method of confirm-
tially leading to death or brain injury, is failure to recog- ing tube position and is increasingly available in critical
nize misplacement of the ET. Attempted intubation of the care.132 False-positive results may be obtained initially
trachea may result in esophageal intubation. This alone is when exhaled gases enter the esophagus during mask
not life-threatening unless it goes unrecognized.129 Thus, ventilation133 or when the patient is generating carbon
confirmation of ET placement in the trachea is essential. dioxide in the gastrointestinal tract (as with recent in-
Visualizing the ET as it passes between the vocal cords gestion of carbonated beverages or bicarbonate-based
into the trachea is the definitive means of assessing correct antacids).134 A false-negative result (ET in trachea but no
tube positioning. This may not always be possible, however, carbon dioxide gas detected) may be obtained when pul-
owing to poor visualization. In addition, the laryngosco- monary blood flow is minimal, as in cardiac arrest.135
pist may be reluctant to accept that the ET is not in the Visualizing the trachea or carina through a fiberoptic
trachea. Several clinical observations support the pres- bronchoscope, which may be readily available in critical
ence of the ET in the trachea. care, also will confirm correct placement of the ET.
Chest wall movement with positive-pressure ventilation
(manual or mechanical) is usual but may be absent in
patients with chronic obstructive pulmonary disease SURGICAL AIRWAY
(COPD), obesity, or decreased compliance (e.g., in severe The indication for a surgical airway is inability to intubate
bronchospasm. Although condensation of water vapor in the trachea in a patient who requires it, and the techniques
the ET suggests that the expired gas is from the lungs, this available are cricothyrotomy and tracheostomy.
30
Ch002-A04841.indd 30 9/13/2007 9:56:07 AM
CHAPTER
136-140
2
Cricothyrotomy neously. The indications for and contraindications to
tracheostomy are summarized in Box 2-7. In comparison
Airway Management in the Critically Ill Adult
Cricothryotomy may be performed as a percutaneous
(needle) or open surgical procedure (Table 2-4). The with long-term orotracheal or nasotracheal intubation,
indication for both these techniques is the cannot intu- tracheostomy often contributes to a patient who is less
bate–cannot ventilate situation. Although needle cricothy- agitated, requires less sedation, and who may wean from
rotomy is an emergency airway procedure, the technique ventilation more easily.51,141 This increased ability to wean
is similar to that for “mini-tracheostomy,” which is per- is sometimes attributed to reduced anatomic dead space.
formed electively. Unlike the other surgical airway tech- The potential reduction in sedation after tracheostomy,
niques, a needle cricothyrotomy does not create a however, is a much greater advantage to weaning than the
definitive airway. It will not allow excretion of carbon small reduction in dead space. The benefits and complica-
dioxide but will produce satisfactory oxygenation for tions of tracheostomy are listed in Box 2-8. Percutaneous
30 to 40 minutes. It can be viewed as a form of apneic tracheostomy is becoming increasingly common and typi-
ventilation (see later on). There are several methods of cally is carried out by medical staff in the ICU (Box
connecting the intravenous cannula to a gas delivery 2-9).
circuit with the facility to ventilate, using equipment Another technique involving retrograde (inside-out)
and connections readily available in the hospital. The intubation of the trachea has been developed: A spe-
appropriate method thus should be thought out in advance cially designed tracheal tube is used to keep the neck
and available on the difficult airway trolley or bag. New tissues under tension until tube placement has been
commercial kits that come preassembled also are accomplished.138 It is a more time-consuming technique
available. that at present is not widely practiced.
A surgical cricothyrotomy allows a cuffed tube to be Although no consensus exists on what defines pro-
inserted through the cricothyroid membrane into the longed tracheal intubation, or when tracheostomy should
lower larynx or upper trachea. This allows positive- be performed,142 most ICUs convert the intubated airway
pressure ventilation for considerable periods and also pro- to a tracheostomy after 1 to 3 weeks, with earlier trache-
tects against pulmonary aspiration. ostomy becoming increasingly favored.141,142
Conventional wisdom states that the tracheostomy pro-
cedure is more complex and time-consuming than a surgi-
Tracheostomy cal cricothyrotomy and should be performed only by a
A tracheostomy is an opening in the trachea—usually surgeon.143 Studies in the elective ICU situation suggest
between the second and third tracheal rings or one space that cricothyrotomy is simpler and (at worst) has a
higher—that may be created surgically or made percuta- similar complication rate.144,145 Although needle cricothy-
rotomy has long been advocated as a life-saving emer-
gency intervention,146 recent work suggests that surgical
Table 2-4. Procedure: Needle and Surgical Cricothyrotomy
The cricothyroid membrane is diamond-shaped and lies
between the thyroid and the cricoid cartilages. Inject
Box 2-7
subdermal lidocaine and adrenaline for local anesthesia.
Tracheostomy: Indications and
Needle Cricothyrotomy Surgical Cricothyrotomy Contraindications
Identify the cricothyroid Make a 1.5-cm skin incision
membrane and the over the cricothyroid
Indications for Tracheostomy
midline. membrane. Inability to maintain a patent airway
Suspected cervical spine instability (percutaneous
Insert a 14-gauge intravenous Incise the superficial fascia
cannula and syringe and subcutaneous fat. technique only)
through the skin and Prevention of damage to vocal cords and (possibly)
membrane. subglottic stenosis
Continuously apply negative Divide the cricothyroid Abnormal anatomy (percutaneous only)
pressure until air enters membrane (short blade, Upper airway obstruction
the syringe. blunt forceps, or the High inotrope or ventilatory requirement (relative)
handle of a scapel often Requirement for tracheobronchial toilet with
is used).
suctioning
Stop at this point and push the Insert (6.0) cuffed Part of larger surgical procedure (e.g., laryngectomy)
cannula off the needle into tracheostomy tube
the trachea. through membrane Contraindications to Tracheostomy
between the thyroid and Prolonged orotracheal or nasotracheal intubation
cricoid cartilages.
Local inflammation
The insertion of the cannula Failure to wean from ventilation
into the trachea allows Bleeding disorder (relative)
apneic (low-pressure)
ventilation or jet (high-
Absence of protective airway reflexes
pressure) ventilation. Arterial bleeding in neck/upper thorax
31
Ch002-A04841.indd 31 9/13/2007 9:56:07 AM
PART
I
Box 2-8 EXTUBATION IN THE DIFFICULT AIRWAY
CRITICAL CARE PROCEDURES, MONITORING, AND PHARMACOLOGY
PATIENT (DECANNULATION)
Tracheostomy: Benefits and Complications The patient with a difficult airway still poses a problem
Benefits at extubation, because reintubation (if required) may be
Comfort even more difficult than the original procedure. Between
Reduced need for sedation 4% and 12% of surgical ICU patients require reintuba-
Improved weaning from ventilation tion152 and may be hypoxic, distressed, and uncooperative
Improved ability to suction trachea at the time of reintubation. The presence of multiple risk
Prevention of ulceration of lips and tongue or healing factors for difficult intubation,100 as well as acute factors
of such ulcers such as airway edema and pharyngeal blood and secre-
Reduced upper airway injury tions, makes reestablishing the airway in such patients
Potential for speech and oral nutrition challenging. Before extubation of any critical care patient,
the critical care team should have formulated a strategy
Complications that includes a plan for reintubation.
Misplacement of tube Stylets (airway exchange catheters) that allow gas
Primary hemorrhage exchange either by jet ventilation or by insufflation
Pneumothorax or tension pneumothorax; hemothorax of oxygen may be useful in the difficult extubation
Surgical emphysema patient.53,153,154 The stylet is placed through the ET, with
Infection care taken to ensure that the distal end has not reached
Late hemorrhage—erosion of innominate (or other) as far as the carina. The ET can then be removed after a
vessels successful leak test. The stylet may remain in situ until the
Tracheoesophageal fistula situation is judged to be stable.100
TUBE DISPLACEMENT IN THE CRITICAL
Box 2-9 CARE UNIT
Procedure: Bronchoscopy-Assisted Endotracheal Tube
Percutaneous Tracheostomy ET displacement in the ICU is a life-threatening emer-
gency that may result in significant morbidity.155 Although
■ Withdraw ET until the cuff lies at or just below the
tube dislodgement sometimes is viewed as unavoidable,
cords.
often preventable factors are involved.156-158 Changes in
■ Pass a flexible bronchoscope down ET to distal
patient posture or head position cause significant move-
end.
ment of the tube within the trachea.159,160 The frequency
■ Make a 1.5- to 2-cm transverse incision at midpoint
of tube displacement can be reduced by good medical and
between cricoid cartilage and suprasternal notch.
nursing practice,161 attention to the arrangements and
■ Strip away tissue down to pretracheal fascia using
ergonomics around the bed, achieving appropriate seda-
blunt dissection (forceps).
tion levels, and ensuring adequate ICU nurse staffing.162,163
■ Under direct vision, use a 14-gauge cannula to punc-
Experience and the ability to anticipate possible glitches
ture anterior tracheal wall (in midline).
constitute an important part of prevention. The manage-
■ Advance cannula into trachea, aspirate air, and
ment of ET displacement starts with an assessment of
insert Seldinger guidewire.
whether the patient can manage without the ET.158 If
■ Dilate around guidewire using dilator(s) or special
replacement is required, preparations for a potentially
forceps.
difficult reintubation are indicated.
■ Pass tracheostomy tube over guidewire into
trachea.
■ Pass bronchoscope through tracheostomy to check Tracheostomy Tube
position. Adverse events with tracheostomy tubes are quite
common.158,164 Displacement may be a life-threatening
event,165 especially if the tube has been in place less than
5 to 7 days142 (before a well-defined tract between skin
cricothyrotomy is the more advantageous procedure.147 and trachea is formed) or if the procedure has been per-
In patients with unfavorable anatomy, surgical cricothy- formed percutaneously (so that the external opening of
rotomy is a viable alternative to elective tracheos- the tract may not easily admit a new tube of the same
tomy.144 Surgical cricothyrotomy has been viewed as a size). The option to leave the patient without a tube
temporary airway that should be converted to tracheos- should be considered, and if this option is pursued, the
tomy within a few days, but it may be used successfully tracheostomy opening should be dressed to make it (to
as a definitive (medium-term) airway,148,149 thereby avoid- some degree) “airtight”—thus facilitating effective cough-
ing conversion from cricothyrotomy to tracheostomy, ing. If the patient needs a tube but replacing the trache-
which can cause significant morbidity.150,151 ostomy is not possible, then oral reintubation should be
32
Ch002-A04841.indd 32 9/13/2007 9:56:07 AM
CHAPTER
2
performed, after which the tracheostomy should be
Problem 2-3 Unilateral Chest Movements in
dressed. With a more mature tracheostomy (more than 7
Airway Management in the Critically Ill Adult
the Intubated Ventilated Patient
days old), it usually is possible to insert a new tube through
the mature tract between skin and trachea.142 Potential Causes
Tracheostomy tubes may be displaced from the lumen 1. Bronchial intubation
of the trachea but appear to be normal when viewed 2. Bronchial obstruction
externally. Difficulty with breathing, ventilation, or tra- 3. Lung collapse, pneumothorax
cheal suctioning or the presence of a pneumothorax, 4. Hemothorax, pleural effusion
5. Consolidation, absent lung (pneumonectomy)
pneumomediastinum, or surgical emphysema may be due
to tracheostomy tube displacement. Fiberoptic assessment Action
of the tube position and patency may be very useful. If bronchial intubation is suspected, deflate the tracheal
tube cuff and slowly withdraw the tube 1 to 2 cm.
Assessing tracheostomy tube position on the chest x-ray
Reinflate the cuff and manually ventilate the patient
film is of no value. while auscultating both sides of the chest. Is air entry
present and equal on both sides? Be suspicious if the
tube has to be withdrawn more than 3 to 4 cm or if the
COMMON PROBLEMS IN tube length at the teeth is much less than the expected
AIRWAY MANAGEMENT correct length; another underlying cause may be
involved. In an adult, the average distance from the
vocal cords to the carina is 12 cm. The tip of an 8.0
(adult) tracheal tube typically is 6.5 cm below the upper
Problem 2-1 Ineffective (Spontaneous) Breathing surface of the balloon, which must sit below the vocal
despite Artificial Airway cords. Therefore, if the upper surface of a cuff is only
3 cm below the vocal cords, the tip will be within 2 to
Underlying Causes 3 cm of the carina. It is easy to inadvertently intubate a
1. Obstructed airway bronchus or leave the tip of the tube close enough to
2. Depressed respiratory drive (influence of drugs) enter the bronchus with head movement or in moving
3. Inefficient respiratory effort (e.g., from fractured ribs the patient. In adults with normal bronchial anatomy,
or diaphragmatic injury) the tube tip usually will pass into the right main
4. Pulmonary pathologic process (pneumonitis, bronchus.
contusion, collapse, consolidation)
Action
Attempt to deliver 100% oxygen. Check airway. When
airway obstruction has been corrected or ruled out, the Problem 2-4 Sudden Airway or Ventilatory
patient’s respiratory status should improve unless Compromise in Ventilated Patient with
another underlying pathologic process is present. If no Orotracheal Tube
improvement is obtained, manually ventilate the patient.
If respiratory status still fails to improve, proceed to
A ventilated patient with an orotracheal tube in place
tracheal intubation with manual or mechanical
may suddenly develop dyspnea, hypoxemia,
ventilation. Investigate and treat any underlying
hypercarbia, and a see-saw respiratory pattern. The
condition.
mechanical ventilator alarm will sound.
Potential Causes
1. Failure of oxygen or air supply to the ventilator
2. Ventilator disconnection or obstruction in ventilator
circuit
Problem 2-2 Ineffective Manual Ventilation despite 3. Obstructed tracheal tube
Artificial Airway • Plugged by mucus or clot
• Kink in tracheal tube
Potential Causes • Biting on tube (previous biting may have
1. Obstructed airway narrowed the tube)
2. Poor seal or poor technique with mask or manual • Obstruction of tube tip by side wall of lower
ventilation airways or carina
3. Pulmonary pathologic process (pneumonitis, 4. Patient’s fighting against ventilator
contusion, collapse, consolidation) 5. Respiratory fatigue (e.g., with weaning from
Action mechanical support or new infection)
Attempt to deliver 100% oxygen at 15 to 20 L/min. 6. Pneumothorax or tension pneumothorax
Check and readjust airway and patient head position. 7. Rapid development of large hemothorax or pleural
When airway obstruction has been corrected or ruled effusion
out, use a two-handed approach for mask and airway, Action
with an assistant squeezing the bag. If no improvement Disconnect the patient from the ventilator, and ventilate
is obtained, check for availability of someone with more through the tracheal tube manually. Have the ventilator
airway experience. If no such person is available, and circuit checked by another appropriate staff
proceed to tracheal intubation with manual or member. High resistance or inability to inflate the lungs
mechanical ventilation. Investigate and treat any suggests tube obstruction or an intrathoracic problem.
underlying condition. The (recent) inability to pass a suction catheter down
33
Ch002-A04841.indd 33 9/13/2007 9:56:07 AM
PART
I
the lumen is suggestive of tube obstruction. If the double-skinned tubes are safer for patients discharged to
CRITICAL CARE PROCEDURES, MONITORING, AND PHARMACOLOGY
patient’s condition is stable or improving, a small general wards. Tracheostomy tubes also may become
fiberoptic bronchoscope or laryngoscope (if readily obstructed when the distal opening is blocked by a
available) may be passed down the tube. An obstruction mucosal flap, the side wall of the trachea, or (rarely) the
may be removed by suction catheter, or removal of the carina.
tube and use of mask ventilation (to reverse hypoxemia
and hypercarbia), followed by reintubation, may be
required. If no answer to the problem is found, consider KEY POINTS
whether the patient’s condition could be due to a
■ The difficult airway may be unanticipated despite
tension pneumothorax. If appropriate, use needle
decompression. Otherwise, order emergency chest film expert preassessment. Airway practitioners must have
and continue either manual or mechanical ventilation as plans to deal with this scenario.
appropriate. ■ Use of the appropriate size and type of laryngoscope
blade in conjunction with other adjuncts and
techniques is an important element of successful
Problem 2-5 Sudden Airway or Ventilatory tracheal intubation—particularly with the
Compromise in Ventilated Patient with Tracheostomy unanticipated difficult airway.
■ Airway difficulty in critical care is common and may
A ventilated patient with a tracheostomy may suddenly be precipitated long after intubation by acute events
develop dyspnea, hypoxemia, hypercarbia, and a see- such as tube dislodgement or obstruction.
saw respiratory pattern. The mechanical ventilator alarm
■ Tube dislodgement in critical care is potentially
will sound.
avoidable and may be influenced by staffing levels,
Potential Causes sedation policy, and other bedside factors.
Causes may include all those listed for Problem 2-4.
■ Surgical cricothyrotomy is a relatively simple
Action procedure and may be used to establish a medium-
Appropriate interventions are the same as for Problem term airway, avoiding the need for tracheostomy.
2-4, with an appreciation of the fact that tracheostomy ■ In critical care, removal of a tracheal tube may
tubes are shorter, more curved, and more rigid than
precipitate an acute difficult airway scenario. A
tracheal tubes. They rarely kink but may become
protocol for handling a difficult reintubation should
blocked with secretions or blood.31,166 Suctioning the
always be in place.
tube may resolve this. Double-skinned tracheostomy
tubes may be unblocked by removing the inner tube ■ All critical care physicians should be familiar with one
(containing the obstruction) for washing, leaving the or more difficult airway algorithms and the practical
outer tube in place to maintain a clear airway. Such skills they require.
REFERENCES
1. Finucane BT, Santora AH: Anatomy of ed. Philadelphia, Lippincott Williams & 17. Watson D: ABC of major trauma.
the airway. In Principles of Airway Wilkins, 1993, pp 485-491. Management of the upper airway. BMJ
Management, 2nd ed. St. Louis, 11. Hinds CJ, Watson D: Applied 1990;300:1388-1391.
Mosby–Year Book, 1996, pp 1-18. cardiovascular and respiratory 18. Criswell JC, Parr MJA, Nolan JP:
2. Standring S (ed): Gray’s Anatomy. The physiology. In Hinds CJ, Watson D Emergency airway management
Anatomical Basis of Clinical Practice, (eds): Intensive Care. A Concise in patients with cervical spine
39th ed. London, Churchill- Textbook, 2nd ed. London, WB injuries. Anaesthesia 1994;49:
Livingstone, 2004. Saunders, 1996, pp 19-39. 900-903.
3. Case Western Reserve University 12. Sassoon CSH, McGovern GP: 19. Morikawa S, Safar P, DeCarlo J:
School of Medicine, Cleveland, Ohio: Oxygenation strategy. In Shoemaker Influence of head position upon upper
http://metrohealthanesthesia.com/ WC, Ayres SM, Grenvik A, Holbrook PR airway patency. Anaesthesiology
edu/airway/anatomy1.htm (eds): Textbook of Critical Care, 4th 1961;22:265.
4. University of Virginia Health System: ed. Philadelphia, WB Saunders, 1999, 20. Castello DA, Smith HS, Lumb PD:
http://www.healthsystem.virginia.edu/ pp 1308-1323. Conventional airway access. In
Internet/Anesthesiology-Elective/ 13. Burchardi H, Richter DW: Control of Shoemaker WC, Ayres SM, Grenvik A,
airway/anatomy.cfm breathing. In Webb AR, Shapiro MJ, Holbrook PR (eds): Textbook of Critical
5. Institute of Rehabilitation Research and Singer M, Suter PM (eds): Oxford Care,. 4th ed. Philadelphia, WB
Development, Ottawa, Ontario, Textbook of Critical Care. Oxford, Saunders, 1999, pp 1232-1246.
Canada: http://www.irrd.ca/education/ Oxford University Press, 1999, 21. Brain AI: The development of the
presentation.asp?refname22 pp 45-47. laryngeal mask—a brief history of the
6. Intellimed International Corporation: 14. Hinds CJ, Watson D: Respiratory invention, early clinical studies and
http://www.innerbody.com/anim/ failure. In Hinds CJ, Watson D (eds): experimental work from which the
mouth.html Intensive Care. A Concise Textbook, laryngeal mask evolved. Eur J
7. Intellimed International Corporation: 2nd ed. London, WB Saunders, 1996, Anaesthesiol Suppl 1991;4:5-17.
http://www.innerbody.com/image/ pp 125-159. 22. Maltby JR, Loken RG, Watson NC: The
cardov.html 15. Civetta JM, Taylor RW, Kirby RR laryngeal mask airway: Clinical
8. Cowan MJ, Gladwin MT, Shelhamer (eds): Critical Care, 3rd ed. appraisal in 250 patients. Can J
JH: Disorders of ciliary motility. Am J Philadelphia, Lippincott-Raven, 1997, Anaesth 1990;37:509-513.
Med Sci 2001;321:3-10. p. 760. 23. Pennant JH, White PF: The laryngeal
9. http://www.aafp.org/afp/ 16. Stone DJ, Gal TJ: Airway management. mask airway. Its uses in anesthesiology.
991115ap/2289.html In Miller RD (ed): Anesthesia, 5th ed, Anesthesiology 1993;79:144.
10. Byron J, Bailey JB (eds): Head and vol 1. Philadelphia, Churchill 24. Ramachandran K, Kannan S: Laryngeal
Neck Surgery—Otolaryngology, 3rd Livingstone, 2000. mask airway and the difficult airway.
34
Ch002-A04841.indd 34 9/13/2007 9:56:07 AM
CHAPTER
Curr Opin Anaesthesiol 2004;17: management of traumatic 55. Caplan RA, Posner KL, Ward RJ, et al:
2
491-493. bronchopleural fistula. Am Surg Adverse respiratory events in
Airway Management in the Critically Ill Adult
25. Ezri T, Szmuk P, Warters RD, et al: 2006;72:530-533. anaesthesia: A closed claims analysis.
Difficult airway management practice 39. Bateman NT, Leach RM: ABC of Anesthesiology 1990;72:828-833.
patterns among anesthesiologists oxygen. Acute oxygen therapy, BMJ 56. Rose DK, Cohen MM: The airway:
practicing in the United States: Have 1998;317:798. problems and predictions in 18,500
we made any progress? J Clin Anesth 40. Campbell TP, Stewart RD, Kaplan RM, patients. Can J Anaesth
2003;15:418-422. et al: Oxygen enrichment of bag- 1994;41:372-383.
26. Parmet JL, Colonna-Romano P, Horrow valve-mask units during positive- 57. Peterson GN, Domino KB, Caplan RA,
JC, et al: The laryngeal mask airway pressure ventilation: A comparison of et al: Management of the difficult
reliably provides rescue ventilation in various techniques. Ann Emerg Med airway: A closed claims analysis.
cases of unanticipated difficult tracheal 1988;17:22-25. Anesthesiology 2005;103:33-39.
intubation along with difficult mask 41. Hartmannsgruber MW, Loudermilk E, 58. Burkle CM, Walsh MT, Harrison BA,
ventilation. Anesth Analg Stoltzfus D: Prolonged use of a Cook et al: Airway management after failure
1998;87:661-665. airway exchange catheter obviated the to intubate by direct laryngoscopy:
27. Brain AI, Verghese C, Addy EV, et al: need for postoperative tracheostomy Outcomes in a large teaching hospital.
The intubating laryngeal mask. II: A in an adult patient. J Clin Anesth Can J Anaesth 2005;52:634-640.
preliminary clinical report of a new 1997;9:496-498. 59. Domino KB, Posner KL, Caplan RA,
means of intubating the trachea. Br J 42. Turner BK, Wakim JH, Secrest J, et al: et al: Airway injury during anesthesia:
Anaesth 1997;79:699. Neuroprotective effects of thiopental, A closed claims analysis.
28. Joo HS, Kapoor S, Rose DK, et al: The propofol, and etomidate. AANA J Anesthesiology 1999;91:1703-1711.
intubating laryngeal mask airway after 2005;73:297-302. 60. Kheterpal S, Han R, Tremper KK, et al:
induction of general anesthesia versus 43. Hedenstierna G: Physiology of the Incidence and predictors of difficult
awake fiberoptic intubation in patients intubated airway. In Webb AR, Shapiro and impossible mask ventilation.
with difficult airways. Anesth Analg MJ, Singer M, Suter PM (eds): Oxford Anesthesiology 2006;105:885-891.
2001;92:1342-1346. Textbook of Critical Care. Oxford, 61. Langeron O, Masso E, Huraux C, et al:
29. Combes X, Sauvat S, Leroux B, et al: Oxford University Press, 1999, Prediction of difficult mask ventilation.
Intubating laryngeal mask airway in pp 1293-1295. Anesthesiology 2000;92:1229.
morbidly obese and lean patients: A 44. Hinds CJ, Watson D: Respiratory 62. Yildiz TS, Solak M, Toker K: The
comparative study. Anesthesiology support. In Intensive Care. A Concise incidence and risk factors of difficult
2005;102:1106-1109. Textbook, 2nd ed. London, WB mask ventilation. J Anesth
30. Combes X, Le Roux B, Suen P, et al: Saunders, 1996, pp 161-192. 2005;19:7-11.
Unanticipated difficult airway in 45. Levine SA, Niederman MS: The impact 63. Crosby ET, Cooper RM, Douglas MJ,
anesthetized patients: Prospective of tracheal intubation on host defenses et al: The unanticipated difficult airway
validation of a management and risks for nosocomial pneumonia. with recommendations for
algorithm. Anesthesiology Clin Chest Med 1991;12:523-543. management. Can J Anaesth
2004;100:1146-1150. 46. Fleming CA, Balaguera HU, Craven DE: 1998;45:757-776.
31. Lavery GG, McCloskey B: Airway Risk factors for nosocomial 64. Samsoon GLT, Young JRB: Difficult
management. In Patient Centred pneumonia. Focus on prophylaxis. tracheal intubation: A retrospective
Acute Care Training (PACT) 2003. Med Clin North Am. 2001;85: study. Anaesthesia 1987;42:487.
European Society of Intensive Care 1545-1563. 65. Needham DM, Thompson DA,
Medicine, Brussels, 2003. 47. Craven DE: Preventing ventilator- Holzmueller CG, et al: A system factors
32. Krafft P, Schebesta K: Alternative associated pneumonia in adults: analysis of airway events from the
management techniques for the Sowing seeds of change. Chest Intensive Care Unit Safety Reporting
difficult airway: Esophageal-tracheal 2006;130:251-260. System (ICUSRS). Crit Care Med
Combitube. Curr Opin Anaesthesiol 48. Safdar N, Crnich CJ, Maki DG: The 2004;32:2227-2233.
2004;17:499-504. pathogenesis of ventilator-associated 66. Beckmann U, Baldwin I, Hart GK, et al:
33. Rabitsch W, Schellongowski P, pneumonia: Its relevance to The Australian Incident Monitoring
Staudinger T, et al: Comparison of a developing effective strategies for Study in Intensive Care: AIMS-ICU. An
conventional tracheal airway with the prevention. Respir Care analysis of the first year of reporting.
Combitube in an urban emergency 2003;50:725-739. Anaesth Intensive Care 1996;24:
medical services system run by 49. Crnich CJ, Safdar N, Maki DG: The 320-329.
physicians. Resuscitation role of the intensive care unit 67. Beckmann U, Baldwin I, Durie M,
2003;57:27-32. environment in the pathogenesis and et al: Problems associated with nursing
34. Mort TC: Laryngeal mask airway and prevention of ventilator-associated staff shortage: An analysis of the first
bougie intubation failures: The pneumonia. Respir Care 3600 incident reports submitted to
Combitube as a secondary rescue 2005;50:813-836. the Australian Incident Monitoring
device for in-hospital emergency 50. Lorente L, Lecuona M, Jimenez A, Study (AIMS-ICU). Anaesth Intensive
airway management. Anesth Analg et al: Ventilator-associated pneumonia Care 1998;26:396-400.
2006;103:1264-1266. using a heated humidifier or a heat 68. Ezri T, Weisenberg M, Khazin V, et al:
35. Rumball CJ, MacDonald D: The PTL, and moisture exchanger: A Difficult laryngoscopy: Incidence and
Combitube, laryngeal mask, and oral randomized controlled trial. Crit Care predictors in patients undergoing
airway: A randomized prehospital 2006;10:R116. coronary artery bypass surgery versus
comparative study of ventilatory 51. Lavery GG: Optimum sedation and general surgery patients. J
device effectiveness and cost- analgesia in critical illness: we need to Cardiothorac Vasc Anesth
effectiveness in 470 cases of keep trying. Crit Care 2004;8:433- 2003;17:321-324.
cardiorespiratory arrest. Prehosp 434. Epub 2004 Nov 3. 69. Mallampati SR, Gatt SP, Gugino LD,
Emerg Care 1997;1:1-10. 52. Practice guidelines for management of et al: A clinical sign to predict difficult
36. Campos JH: Which device should be the difficult airway: an updated report tracheal intubation: A prospective
considered the best for lung isolation: by the American Society of study. Can Anaesth Soc J 1985;
Double-lumen endotracheal tube Anesthesiologists Task Force on 32:429.
versus bronchial blockers? Curr Opin Management of the Difficult Airway. 70. Cattano D, Panicucci E, Paolicchi A,
Anaesthesiol 2007;20:27-31. Anesthesiology 2003;98:1269-1277. et al: Risk factors assessment of the
37. Wendt M, Hachenberg T, Winde G, 53. Benumof JL: Management of the difficult airway: An Italian survey of
Lawin P: Differential ventilation with difficult adult airway. With special 1956 patients. Anesth Analg
low-flow CPAP and CPPV in the emphasis on awake tracheal 2004;99:1774-1779.
treatment of unilateral chest trauma. intubation. Anesthesiology 71. Lee A, Fan LT, Gin T, et al: A
Intensive Care Med 1989;15:209-211, 1991;75:1087-1110. systematic review (meta-analysis) of
1989. 54. Rashkin MC, Davis T: Acute the accuracy of the Mallampati tests
38. Cheatham ML, Promes JT: complications of endotracheal to predict the difficult airway. Anesth
Independent lung ventilation in the intubation Chest 1986;89:165-167. Analg 2006;102:1867-1878.
35
Ch002-A04841.indd 35 9/13/2007 9:56:07 AM
PART
I 72. Pilkington S, Carli F, Dakin MJ, et al: emergency departments. Arch Emerg 105. Benumof JL: Laryngeal mask airway
Increase in Mallampati score during Med 1988;5:151-155. and the ASA difficult airway algorithm.
CRITICAL CARE PROCEDURES, MONITORING, AND PHARMACOLOGY
pregnancy. Br J Anaesth 1995;74:638. 90. Kluger MT, Bukofzer M, Bullock M, Anaesthesiology 1996;84:686-699.
73. Benumof JL: Obesity, sleep apnea, the et al: Anaesthetic assistants: Their 106. Heidegger T, Gerig HJ: Algorithms for
airway and anesthesia. Curr Opin role in the development and resolution management of the difficult airway.
Anaesthesiol 2004;17: 21-30, 2004. of anaesthetic incidents. Anaesth Curr Opin Anaesthesiol 2004;17:
74. Wilson ME, Spiegelhalter D, Robertson, Intensive Care 1999;27:269-274. 483-484.
JA, et al: Predicting difficult intubation. 91. Kluger MT, Bullock MF: Recovery room 107. Cobley M, Vaughan RS: Recognition
Br J Anaesth 1988;61:211. incidents: A review of 419 reports and management of difficult airway
75. El-Ganzouri AR, McCarthy RJ, Tuman from the Anaesthetic Incident problems. Br J Anaesth 1992;68:90-97.
KJ, et al: Preoperative airway Monitoring Study (AIMS). Anaesthesia 108. Gupta B, McDonald JS, Brooks JH,
assessment predictive value of a 2002;57:1060-1066. et al: Oral fiberoptic intubation over
multivariate risk index. Anesth Analg 92. Robbertze R, Posner KL, Domino KB: a retrograde guidewire. Anesth
1996;82:1197. Closed claims review of anesthesia for Analg 1989;68:517-519.
76. Rosenblatt WH: Preoperative planning procedures outside the operating 109. Finucane BT, Santora AH: Fibreoptic
of airway management in critical care room. Curr Opin Anaesthesiol intubation in airway management. In
patients. Crit Care Med 2004;32: 2006;19: 436-442. Finucane BT, Santora AH (eds):
S186-S192. 93. Wang HE, Seitz SR, Hostler D, et al: Principles of Airway Management,
77. Yentis SM: Predicting difficult DM. Defining the learning curve for 2nd ed. St. Louis, Mosby–Year Book,
intubation—worthwhile exercise or paramedic student endotracheal 1996, p 102.
pointless ritual? Anaesthesia intubation. Prehosp Emerg Care 110. Levitan RM, Mickler T, Hollander JE:
2002;57:105-109. 005;2:156-162. Bimanual laryngoscopy: A
78. Field JM, Baskett PJF: Basic airway 94. Wang HE, Kupas DF, Paris PM, et al: videographic study of external
management. In Webb AR, Shapiro Multivariate predictors of failed laryngeal manipulation by novice
MJ, Singer M, Suter PM (eds): Oxford prehospital endotracheal intubation. intubators. Ann Emerg Med
Textbook of Critical Care. Oxford, Acad Emerg Med 2003;10:717-724. 2002;40:30-37.
Oxford University Press, 1999, 95. Krisanda TJ, Eitel DR, Hess D, et al: An 111. Latto IP, Stacey M, Mecklenburgh J,
pp 1-6. analysis of invasive airway et al: Survey of the use of the gum
79. Mason RA, Fielder CP: The obstructed management in a suburban elastic bougie in clinical practice.
airway in head and neck surgery. emergency medical services system. Anaesthesia 2002;57:379-384.
Anaesthesia 1999;54:625-628. Prehospital Disaster Med 112. Yentis SM: The effects of single-
80. Morris CG, McCoy EP, Lavery GG: 1992;7:121-126. handed and bimanual cricoid pressure
Spinal immobilisation for unconscious 96. Wang HE, Sweeney TA, O’Connor RE, on the view at laryngoscopy.
patients with multiple injuries. BMJ et al: Failed prehospital intubations: Anaesthesia 1997;52:332-335.
2004;329:495-499. An analysis of emergency department 113. Snider DD, Clarke D, Finucane BT: The
81. Ardekian L, Rosen D, Klein Y, et al: Life courses and outcomes. Prehosp Emerg “BURP” maneuver worsens the glottic
threatening complications and Care 2001;5:134-141. view when applied in combination
irreversible damage following 97. Schwartz DE, Matthay MA, Cohen NH: with cricoid pressure. Can J Anaesth
maxillofacial trauma. Injury Death and other complications of 2005;52:100-104.
1998;29:253-256. emergency airway management in 114. Levitan RM, Kinkle WC, Levin WJ,
82. Awad Z, Pothier DD: Management of critically ill adults. A prospective et al: Laryngeal view during
surgical airway emergencies by junior investigation of 297 tracheal laryngoscopy: A randomized trial
ENT staff: A telephone survey. J intubations. Anesthesiology comparing cricoid pressure, backward-
Laryngol Otol 2006;1-4 [Epub ahead 1995;82:367-376. upward-rightward pressure, and
of print]. 98. Brimacombe J, Keller C, Kunzel KH, bimanual laryngoscopy. Ann Emerg
83. Rosenstock C, Ostergaard D, et al: Cervical spine motion during Med 2005;47:548-555. Epub 2006
Kristensen MS, et al: Residents lack airway management: A Mar 14.
knowledge and practical skills in cinefluoroscopic study of the 115. Finucane BT, Santora AH: Difficult
handling the difficult airway. Acta posteriorly destabilized third cervical intubation. In Principles of
Anaesthesiol Scand 2004;48: vertebrae in human cadavers. Anesth Airway Management. 2nd ed.
1014-1018. Analg 2000;91:1274-1278. St Louis: Mosby–Year Book, 1996,
84. Schwid HA, Rooke GA, Carline J, et al: 99. Waltl B, Melischek M, Schuschnig C, pp 187-226.
Evaluation of anesthesia residents et al:.Tracheal intubation and cervical 116. Bokhari A, Benham SW, Popat MT:
using mannequin-based simulation: A spine excursion: Direct laryngoscopy Management of unanticipated difficult
multiinstitutional study. Anesthesiology vs.intubating laryngeal mask. intubation: A survey of current
2002;97:1434-1444. Anaesthesia 22001;56:221-226. practice in the Oxford region. Eur J
85. Sagarin MJ, Barton ED, Chang YM, 100. Loudermilk EP, Hartmannsgruber M, Anaesthesiol 2004;21;123-127.
et al: Airway management by US and Stoltzfus DP, et al: A prospective study 117. MacQuarrie K, Hung OR, Law JA:
Canadian emergency medicine of the safety of tracheal extubation Tracheal intubation using Bullard
residents: A multicenter analysis of using a pediatric airway exchange laryngoscope for patients with a
more than 6,000 endotracheal catheter for patients with a known simulated difficult airway. Can J
intubation attempts. Ann Emerg Med difficult airway. Chest 1997;111: Anaesth 1999;46:760-765.
2005;46:328-336. 1660-1665. 118. Yardeni IZ, Gefen A, Smolyarenko V,
86. Kluger MT, Short TG: Aspiration 101. Mort TC: Preoxygenation in critically ill et al: Design evaluation of commonly
during anaesthesia: A review of 133 patients requiring emergency tracheal used rigid and levering laryngoscope
cases from the Australian Anaesthetic intubation. Crit Care Med blades. Acta Anaesthesiol Scand
Incident Monitoring Study (AIMS). 2005;33:2672-2675. 2002;1003-1009.
Anaesthesia 1999;54:19-26. 102. Jensen LA, Onyskiw JE, Prasad NG: 119. McIntyre JW: Laryngoscope design
87. Mayo PH, Hackney JE, Mueck JT, et al: Meta-analysis of arterial oxygen and the difficult adult tracheal
Achieving house staff competence in saturation monitoring by pulse intubation. Can J Anaesth
emergency airway management: oximetry in adults. Heart Lung 1989;36:94-98.
Results of a teaching program using a 1998;27:387-408. 120. Sethuraman D, Darshane S, Guha A,
computerized patient simulator. Crit 103. Van de Louw A, Cracco C, Cerf C, et al: A randomised, crossover study of
Care Med 2004;32:2422-2427. et al: Accuracy of pulse oximetry in the Dorges, McCoy and Macintosh
88. Vickers MD: Anaesthetic team and the the intensive care unit. Intensive Care laryngoscope blades in a simulated
role of nurses—European perspective. Med 2001;27:1606-1613. difficult intubation scenario.
Best Pract Res Clin Anaesthesiol 104. Henderson JJ, Popat MT, Latto IP, et al: Anaesthesia 1989;61:482-487.
2002;16:409-421. Difficult Airway Society guidelines for 121. Cook TM, Tuckey JP: A comparison
89. James MR, Milsom PL: Problems management of the unanticipated between the Macintosh and the
encountered when administering difficult intubation. Anaesthesia McCoy laryngoscope blades.
general anaesthetics in accident and 2004;59:675-694. Anaesthesia 1996;51:977-980.
36
Ch002-A04841.indd 36 9/13/2007 9:56:07 AM
CHAPTER
122. Chisholm DG, Calder I: Experience 138. Konopke R, Zimmermann T, Volk A, 151. Altman KW, Waltonen JD, Kern RC:
2
with the McCoy laryngoscope in et al: Prospective evaluation of the Urgent surgical airway intervention: A
Airway Management in the Critically Ill Adult
difficult laryngoscopy. Anaesthesia retrograde percutaneous translaryngeal 3 year county hospital experience.
1997;52:906-908. tracheostomy (Fantoni procedure) in a Laryngoscope 2005;115:2101-2104.
123. Mehta S: Transtracheal illumination surgical intensive care unit: Technique 152. Demling RH, Read T, Lind LJ, et al:
for optimal tracheal tube placement. and results of the Fantoni Incidence and morbidity of extubation
A clinical study. Anaesthesia tracheostomy. Head Neck 2006;28: failure in surgical intensive care
1989;44:970-972. 355-359. patients. Crit Care Med 1988;16:
124. Hung OR, Pytka S, Morris I: Clinical 139. Westphal K, Byhahn C, Wilke HJ, et al: 573-577.
trial of a new lightwand device Percutaneous tracheostomy: A clinical 153. Bedger RC Jr, Chang JL: A jet-stylet
(Trachlight) to intubate the trachea. comparison of dilatational (Ciaglia) endotracheal catheter for difficult
Anesthesiology 1995;83:509-514. and translaryngeal (Fantoni) intubation airway management.
125. Wong DT, Lai K, Chung FF, et al: techniques. Anesth Analg 1999;89: Anaesthesiology 1987;66:221-223.
Cannot intubate-cannot ventilate and 938-943. 154. Cooper RM: The use of an
difficult intubation strategies: Results 140. Groves DS, Durbin CG, Jr: endotracheal ventilation catheter in
of a Canadian national survey. Anesth Tracheostomy in the critically ill: the management of difficult
Analg 2005;100:1439-1446. Indications, timing and techniques. extubations. Can J Anaesth 1996;43:
126. Morris IR: Continuing medical Curr Opin Crit Care 2007;13:90-97. 90-93.
education: Fibreoptic intubation. Can J 141. Schweikert WD, Gelbach BK, Pohlman 155. Epstein SK, Nevins ML, Chung J: Effect
Anesthes 1994;41:996-1008. AJ, et al: Daily interruption of sedative of unplanned extubation on outcome
127. Jolliet P, Chevrolet JC: Bronchoscopy in infusions and complications of critical of mechanical ventilation. Am J Respir
the intensive care unit. Intensive Care illness in mechanically ventilated Crit Care Med 2000;161:1912-1916.
Med 1992;18:160-169. patients. Crit Care Med 2004;32: 156. Rothschild JM, Landrigan CP, Cronin
128. Lavery GG, McCloskey BV: The difficult 1272-1276. JW, et al: The Critical Care Safety
airway in the critical care unit. Crit 142. Hazard PB: Tracheostomy. In Webb AR, Study: The incidence and nature of
Care Med (in press). Shapiro MJ, Singer M, Suter PM (eds): adverse events and serious medical
129. Schwartz DE, Matthay MA, Cohen NH: Oxford Textbook of Critical Care. errors in intensive care. Crit Care Med
Death and other complications of Oxford, Oxford University Press, 1999, 2005;33:1694-1700.
emergency airway management in pp 1305-1308. 157. Beckmann U, Gillies DM: Factors
critically ill adults. A prospective 143. Finucane BT, Santora AH: Surgical associated with reintubation in
investigation of 297 tracheal approaches to airway management. In intensive care: An analysis of causes
intubations. Anesthesiology Finucane BT, Santora AH (eds): and outcomes. Chest
1995;82:367-376. Principles of Airway Management, 2nd 2001;120:538-42.
130. Birmingham PK, Cheney FW, Ward RJ: ed. St. Louis: Mosby–Year Book, 1996, 158. Kapadia FN, Bajan KB, Raje KV: Airway
Esophageal intubation: A review of pp 251-284. accidents in intubated intensive care
detection techniques. Anesth Analg 144. Rehm CG, Wanek SM, Gagnon EB, unit patients: An epidemiological
1986;65:886-891. et al: Cricothyroidotomy for elective study. Crit Care Med 2000;28:659.
131. Schwartz DE, Lieberman JA, Cohen airway management in critically ill 159. Conrardy PA, Goodman LR, Lainge F,
NH: Women are at greater risk than trauma patients with technically et al: Alteration of endotracheal tube
men for malpositioning of the challenging neck anatomy. Crit position: Flexion and extension of the
endotracheal tube after emergent Care 2002;6:531-535. Epub 2002 Sep neck. Crit Care Med 1976;4:7.
intubation. Crit Care Med 17. 160. Yap SJ, Morris RW, Pybus DA:
1994;22:1127-1131. 145. Francois B, Clavel M, Desachy A, et al: Alterations in endotracheal tube
132. Erasmus PD: The use of end-tidal Complications of tracheostomy position during general anaesthesia.
carbon dioxide monitoring to confirm performed in the ICU: Subthyroid Anaesth Intensive Care 1994;22:
endotracheal tube placement in adult tracheostomy vs surgical 586-88.
and paediatric intensive care units in cricothyroidotomy. Chest 161. Birkett KM, Southerland KA, Leslie GD:
Australia and New Zealand. Anaesth 2003;123:151-158. Reporting unplanned extubation.
Intensive Care 2004;32:672-675. 146. Smith RB, Schaer WB, Pfaeffle Intensive Crit Care Nurs 2005;21:
133. Linko K, Paloheimo M, Tammisto T: H: Percutaneous transtracheal 65-75.
Capnography for detection of ventilation for anaesthesia and 162. Morrison AL, Beckmann U, Durie M,
accidental oesophageal intubation. resuscitation: A review and report of et al: The effects of nursing staff
Acta Anaesthesiol Scand 1983;27: complications. Can Anaesth Soc J inexperience (NSI) on the occurrence
199-202. 1975;22:607-612. of adverse patient experiences in ICUs.
134. Sum Ping ST, Mehta MP, Symreng T: 147. Scrase I, Woollard M: Needle vs Aust Crit Care 2001;14:116-121.
Reliability of capnography in surgical cricothyroidotomy: A short cut 163. Chevron V, Menard JF, Richard JC, et
identifying esophageal intubation to effective ventilation. Anaesthesia al: Unplanned extubation: risk factors
with carbonated beverage or antacid 2006;61: 921-923. of development and predictive criteria
in the stomach. Anesth Analg 148. Brantigan CO, Grow JB: for reintubation. Crit Care Med
1991;73:333. Cricothyroidotomy: Elective use in 1998;26:1049-1053.
135. Falk JL, Rackow EC, Weil MH: End-tidal respiratory problems requiring 164. Kapadia FN, Bajan KB, Singh S, et al:
carbon dioxide concentration during tracheostomy. Thorac Cardiovasc Surg Changing patterns of airway accidents
cardiopulmonary resuscitation. N Engl 2006;71:72-81. in intubated ICU patients. Intensive
J Med 1988;318:607. 149. Wright MJ, Greenberg DE, Hunt JP, Care Med 2001;27:296-300.
136. Moe KS, Stoeckli SJ, Schmid S, et al: et al: Surgical cricothyroidotomy in 165. Seay SJ, Gay SL, Strauss M:
Percutaneous tracheostomy: A trauma patients. South Med J Tracheostomy emergencies. Am J Nurs
comprehensive evaluation. Ann Otol 2003;96:465-467. 2002;102:59, 61-63.
Rhinol Laryngol 1999;108:384-391. 150. DeLaurier GA, Hawkins ML, Treat RC, 166. Trottier SJ, Ritter S, Lakshmanan R,
137. Powell DM, Price PD, Forrest LA: et al: Acute airway management. Role et al: Percutaneous tracheostomy tube
Review of percutaneous tracheostomy. of cricothyroidotomy. Am Surg 1990; obstruction: Warning. Chest
Laryngoscope 1998;108:170-177. 56:12-15. 2002;122:1377-1381.
37
Ch002-A04841.indd 37 9/13/2007 9:56:07 AM
You might also like
- Airway ManagementDocument8 pagesAirway ManagementMichael Sedano100% (1)
- Psychological Perspective PDFDocument7 pagesPsychological Perspective PDFRonin FernandezNo ratings yet
- Repair Station Class RatingDocument17 pagesRepair Station Class RatingLucaNo ratings yet
- Pygmalion AnalysisDocument28 pagesPygmalion AnalysisHafsa Usmani82% (11)
- Chapter 15 Respiratory SystemDocument3 pagesChapter 15 Respiratory SystemRayumaaa100% (1)
- 2 - Respiratory SystemDocument9 pages2 - Respiratory SystemHannah Grace CorveraNo ratings yet
- The Psychology of Thinking About The FutureDocument570 pagesThe Psychology of Thinking About The FutureMarina Petrovic100% (2)
- External Respiration: Angiotensin-Converting EnzymeDocument4 pagesExternal Respiration: Angiotensin-Converting EnzymeEllä PabustanNo ratings yet
- JPT MagazineDocument148 pagesJPT MagazineAsahel NuñezNo ratings yet
- Anatomy and Physiology of Respiratory SystemDocument21 pagesAnatomy and Physiology of Respiratory Systemsameeha semiNo ratings yet
- Kina Bank Personal Account Opening FormDocument7 pagesKina Bank Personal Account Opening FormJohn Yala100% (4)
- ANAPHY Respiratory SystemDocument30 pagesANAPHY Respiratory SystemAshley Franceska CansanayNo ratings yet
- 2 - Respiratory SystemDocument9 pages2 - Respiratory SystemHannah Grace CorveraNo ratings yet
- The New Lawsuit Ecosystem: Trends, Targets and PlayersDocument164 pagesThe New Lawsuit Ecosystem: Trends, Targets and PlayersU.S. Chamber of Commerce50% (2)
- Script For ASNHS Intrams 2014Document2 pagesScript For ASNHS Intrams 2014Charlad Cha Bangtan Potter100% (5)
- O CO O CO O CO: Chapter 15: Respiratory SystemDocument3 pagesO CO O CO O CO: Chapter 15: Respiratory SystemPrecious Faith RodriguezNo ratings yet
- Teachers Resource CDROM Rooftops 2 PDFDocument6 pagesTeachers Resource CDROM Rooftops 2 PDFViejoSuárezInes100% (2)
- Excerpt - Come Away My Beloved. - .And Rest by Frances J. RobertsDocument21 pagesExcerpt - Come Away My Beloved. - .And Rest by Frances J. RobertsBarbour Books100% (4)
- UNIT 1 (MS 1) Care of Clients With Problems in OxygenationDocument10 pagesUNIT 1 (MS 1) Care of Clients With Problems in OxygenationElle MirandaNo ratings yet
- Rehabilitation After Total LaryngectomyDocument7 pagesRehabilitation After Total LaryngectomyAnois Llivar100% (1)
- 1.11 ANATOMY - The Nose and Paransal SinusesDocument4 pages1.11 ANATOMY - The Nose and Paransal SinusesPaolo NaguitNo ratings yet
- AVIAN Respiratory SystemDocument7 pagesAVIAN Respiratory Systemtaner_soysurenNo ratings yet
- Janice Chan, M.D.: AnesthesiologyDocument14 pagesJanice Chan, M.D.: AnesthesiologyAbegail IbañezNo ratings yet
- Ms Trans Anaphy RespiDocument6 pagesMs Trans Anaphy RespiZariah Dela CruzNo ratings yet
- Lec 1 Respiratory SystemDocument3 pagesLec 1 Respiratory SystemfaiNo ratings yet
- OXYGENATIONDocument10 pagesOXYGENATIONnicoleNo ratings yet
- Airway Anatomy &assessmentDocument44 pagesAirway Anatomy &assessmentAya AlefeshatNo ratings yet
- Airway Anatomy and AssessmentDocument69 pagesAirway Anatomy and AssessmentEvan Permana Putra100% (1)
- Rhinoscopyinthedog1 AnatomyandtechniquesDocument8 pagesRhinoscopyinthedog1 AnatomyandtechniquesZackiary YukiNo ratings yet
- Anatomy - Section 9Document9 pagesAnatomy - Section 9Rosinah M KekanaNo ratings yet
- Airway - Assessment - Predictors - of - Difficult - Airway HNDocument7 pagesAirway - Assessment - Predictors - of - Difficult - Airway HNfoolscribdNo ratings yet
- Airway Mngt. Module 1.Document11 pagesAirway Mngt. Module 1.marc gorospeNo ratings yet
- CHAP13Document8 pagesCHAP13Crystal ARIETANo ratings yet
- Anatomy of AirwayDocument50 pagesAnatomy of AirwayHari Om ChaurasiyaNo ratings yet
- Unit 1Document60 pagesUnit 1Vanshika GuptaNo ratings yet
- Mallampati Airway ClassificationDocument6 pagesMallampati Airway ClassificationAnthony Osemudiamen OseghaleNo ratings yet
- Internet Scientific PublicationsDocument12 pagesInternet Scientific PublicationsAnonymous h0DxuJTNo ratings yet
- Respiratory System TransesDocument5 pagesRespiratory System Transesadrielvamos28No ratings yet
- Piazza 2010Document11 pagesPiazza 2010Israel BlancoNo ratings yet
- Jurnal Anatomi IDocument20 pagesJurnal Anatomi IStanislaus Stanley SuhermanNo ratings yet
- 1st Lecture of Respiratory Histology by DR RoomiDocument24 pages1st Lecture of Respiratory Histology by DR RoomiMudassar Roomi100% (1)
- Respiratory Notes (Tortora)Document3 pagesRespiratory Notes (Tortora)Eli MinchaiNo ratings yet
- Nasal ConchaDocument6 pagesNasal ConchaJohann S M MendezNo ratings yet
- MS Trans 1 DraftDocument12 pagesMS Trans 1 DraftVallerie Nicole GasparNo ratings yet
- 04 Respiration 2022 - AnswersDocument10 pages04 Respiration 2022 - Answersria khanNo ratings yet
- Resource Guide: Principles of CapnographyDocument70 pagesResource Guide: Principles of CapnographyJohn Paul PunzalanNo ratings yet
- 5.1 Anatomy, Physiology and Immunology of The Pharynx and EsophagusDocument6 pages5.1 Anatomy, Physiology and Immunology of The Pharynx and EsophagusPietersNo ratings yet
- Respiratory Physiology Mosby Physiology Series 2Nd Edition Edition Michelle M Cloutier All ChapterDocument67 pagesRespiratory Physiology Mosby Physiology Series 2Nd Edition Edition Michelle M Cloutier All Chaptervincent.pathak166100% (11)
- Airway and Its Maintenance Hand Out2Document49 pagesAirway and Its Maintenance Hand Out2agatakassaNo ratings yet
- ANESTHESIOLOGY TRANS Airway Dr. Gutierrez PDFDocument15 pagesANESTHESIOLOGY TRANS Airway Dr. Gutierrez PDFMeahgan Renee FeudoNo ratings yet
- Anatomy and Physiology of PharynxDocument16 pagesAnatomy and Physiology of Pharynxaleeza nomanNo ratings yet
- Topic 11Document15 pagesTopic 11Lorraine RiegoNo ratings yet
- Anaphy RespiratoryDocument14 pagesAnaphy RespiratoryAngellene GraceNo ratings yet
- CHAPTER 22 The Respiratory SystemDocument11 pagesCHAPTER 22 The Respiratory System楊畯凱No ratings yet
- Ebook Respiratory Physiology Mosby Physiology Series PDF Full Chapter PDFDocument67 pagesEbook Respiratory Physiology Mosby Physiology Series PDF Full Chapter PDFkyle.heffner607100% (28)
- Airway Assessment Predictors of Difficult AirwayDocument7 pagesAirway Assessment Predictors of Difficult AirwayChakib AmariNo ratings yet
- Anatomyand Physiologyofthe Larynxand HypopharynxDocument13 pagesAnatomyand Physiologyofthe Larynxand HypopharynxAngela PetreskaNo ratings yet
- CH 23 Respiration F 2017 SRMDocument153 pagesCH 23 Respiration F 2017 SRMJuliaNo ratings yet
- Anaphy Chapter 23 Respiratory System Doran MLS 1 FDocument9 pagesAnaphy Chapter 23 Respiratory System Doran MLS 1 FayenaNo ratings yet
- We Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsDocument35 pagesWe Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsmeenakshiNo ratings yet
- Organs of The Respiratory SystemDocument8 pagesOrgans of The Respiratory SystemCrystal Kaye RecasaNo ratings yet
- Respiratory SystemDocument54 pagesRespiratory SystemDominique MohanNo ratings yet
- Tonsil Anatomy Review PDFDocument3 pagesTonsil Anatomy Review PDFElisabethLisyeKonnyNo ratings yet
- Respiratory SystemDocument8 pagesRespiratory SystemAlther LorenNo ratings yet
- Advancedtechniquesin Nonsurgicalrhinoplasty: Umang Mehta,, Zachary FridiriciDocument11 pagesAdvancedtechniquesin Nonsurgicalrhinoplasty: Umang Mehta,, Zachary FridiriciRaphaela TravassosNo ratings yet
- Hand Out 3 Respiratory System Overview PDFDocument12 pagesHand Out 3 Respiratory System Overview PDFGrape JuiceNo ratings yet
- Treatise on the Anatomy and Physiology of the Mucous Membranes: With Illustrative Pathological ObservationsFrom EverandTreatise on the Anatomy and Physiology of the Mucous Membranes: With Illustrative Pathological ObservationsNo ratings yet
- ACC101 Practice Problem - Complete Accounting CycleDocument2 pagesACC101 Practice Problem - Complete Accounting CycleJeluMVNo ratings yet
- Aic Management: Left View 01Document1 pageAic Management: Left View 01Hung NguyentheNo ratings yet
- Dixith Devops ResumeDocument4 pagesDixith Devops ResumeNaveenNo ratings yet
- Meritlistdi&cDocument362 pagesMeritlistdi&cOCILABS Origin & Cause InvestigationNo ratings yet
- 9.1 Guidelines Semester Test 1Document7 pages9.1 Guidelines Semester Test 1Gael SNo ratings yet
- Ceiling Design Sheet 1Document1 pageCeiling Design Sheet 1Alvin Jay CastilloNo ratings yet
- CDocument59 pagesCKishan PandaNo ratings yet
- Schedule BDocument1 pageSchedule BBrandySpiceNo ratings yet
- Structural Analysis Report OF Office Building IN Butwal, RupandehiDocument41 pagesStructural Analysis Report OF Office Building IN Butwal, RupandehiAsan GajurelNo ratings yet
- COLGATE Present Perfect Vs Simple PastDocument3 pagesCOLGATE Present Perfect Vs Simple PastCoco Del CastilloNo ratings yet
- Chapter 21Document12 pagesChapter 21Mark ArceoNo ratings yet
- Sainz (Web OK)Document60 pagesSainz (Web OK)sebascianNo ratings yet
- Raniri and The Wujudiyyah of 17th Century Acheh PDFDocument260 pagesRaniri and The Wujudiyyah of 17th Century Acheh PDFDedi Gunawan SaputraNo ratings yet
- Kolleru Report 9 Apri 11Document203 pagesKolleru Report 9 Apri 11MamtaNo ratings yet
- MINCO A3 Genset Controller User's ManualDocument9 pagesMINCO A3 Genset Controller User's ManualRODRIGO_RALONo ratings yet
- Soundplate™: Owner'S ManualDocument20 pagesSoundplate™: Owner'S ManualdanielNo ratings yet
- Examiner's Report: P7 Advanced Audit and Assurance December 2017Document4 pagesExaminer's Report: P7 Advanced Audit and Assurance December 2017Lukas CNo ratings yet
- ACC Mix Design of Different GradesDocument1 pageACC Mix Design of Different GradesVikram KOTHARINo ratings yet
- Readings in Philippine HistoryDocument9 pagesReadings in Philippine HistoryEddie Agbayani Jr.No ratings yet
- Unit 2 Economic ActivitiesDocument3 pagesUnit 2 Economic Activitiesnotkingit68No ratings yet