You might also like
- Advanced Biosensors for Virus Detection: Smart Diagnostics to Combat SARS-CoV-2From EverandAdvanced Biosensors for Virus Detection: Smart Diagnostics to Combat SARS-CoV-2Raju KhanNo ratings yet
- RTPCRBulk05-23-2021 2021-05-23 - 08-16Document28 pagesRTPCRBulk05-23-2021 2021-05-23 - 08-16Sumit PatelNo ratings yet
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Shashi KumarNo ratings yet
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)பைசல் ஹNo ratings yet
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Kaushik GoswamiNo ratings yet
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Soumya SwainNo ratings yet
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Harsh TyagiNo ratings yet
- Covid Positive Test ReportDocument2 pagesCovid Positive Test ReportShubharthak SangharshaNo ratings yet
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)manoj s.vNo ratings yet
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)von demNo ratings yet
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Sanjay Kumar GuptaNo ratings yet
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Rajat ChuttaniNo ratings yet
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)rakeshNo ratings yet
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)subhasis mahapatraNo ratings yet
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)ram lalNo ratings yet
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)mohan kumarNo ratings yet
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Vivek CGNo ratings yet
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)hajiabdurrahman1986No ratings yet
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Rajesh kumar rout boxing channelNo ratings yet
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Maltesh BannihalliNo ratings yet
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Shivam kumarNo ratings yet
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)vignesh seenirajNo ratings yet
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)ShiljithNo ratings yet
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)google payNo ratings yet
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Recruitment Cell Aiims BilaspurNo ratings yet
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Nishant KaushalNo ratings yet
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)18Y117 - MUKESHKUMAR M KNo ratings yet
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : Nic - (Https://Covid19Cc - Nic.In) Page 1/26 24-05-2021 14:37:11Document26 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : Nic - (Https://Covid19Cc - Nic.In) Page 1/26 24-05-2021 14:37:11Sumit PatelNo ratings yet
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)CROWNTECH SURFACENo ratings yet
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Ravi Kumar GangwarNo ratings yet
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Pramod shuklaNo ratings yet
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)fasf asfgrgNo ratings yet
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Hindi HD MoviesNo ratings yet
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Umesh MishraNo ratings yet
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Phono CompNo ratings yet
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : Nic - (Https://Covid19Cc - Nic.In) Page 1/18 27-04-2021 13:49:04Document18 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : Nic - (Https://Covid19Cc - Nic.In) Page 1/18 27-04-2021 13:49:04Sumit PatelNo ratings yet
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Mohammed Ismail VaseemNo ratings yet
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)nitish mahatoNo ratings yet
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Vaibhav KumarNo ratings yet
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : Nic - (Https://Covid19Cc - Nic.In) Page 1/24 28-04-2021 12:16:31Document24 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : Nic - (Https://Covid19Cc - Nic.In) Page 1/24 28-04-2021 12:16:31Sumit PatelNo ratings yet
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Váìßhäv UmarvaishyaNo ratings yet
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Amit GargNo ratings yet
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)VignesNo ratings yet
- Tahir Test 22.04.2021Document2 pagesTahir Test 22.04.2021bucolicNo ratings yet
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)arpanNo ratings yet
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)gjvNo ratings yet
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)nithya nithyaNo ratings yet
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Atul mishraNo ratings yet
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Chintu JashwanthNo ratings yet
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Jaspal Singh RanaNo ratings yet
- Document From LalitDocument2 pagesDocument From LalitLalit MohantaNo ratings yet
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)K P Singh Shakya-MuniNo ratings yet
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : Nic - (Https://Covid19Cc - Nic.In) Page 1/24 22-05-2021 11:43:47Document24 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : Nic - (Https://Covid19Cc - Nic.In) Page 1/24 22-05-2021 11:43:47Sumit PatelNo ratings yet
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Prem BhondeNo ratings yet
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)MEIVELJ 19EE025No ratings yet
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Tanya SirohiNo ratings yet
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)shailesh mahtoNo ratings yet
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Rakshith H P GadedhNo ratings yet
- Nanochromatography and Nanocapillary Electrophoresis: Pharmaceutical and Environmental AnalysesFrom EverandNanochromatography and Nanocapillary Electrophoresis: Pharmaceutical and Environmental AnalysesNo ratings yet
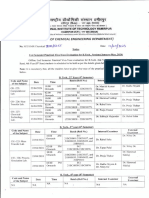
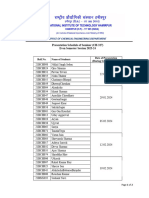
- End Sem Practical May2024Document2 pagesEnd Sem Practical May2024Akhil KumarNo ratings yet
- Prsentation Schedule (CH-327)Document2 pagesPrsentation Schedule (CH-327)Akhil KumarNo ratings yet
- B. Tech. Seminar Report: Recycling of PlasticsDocument31 pagesB. Tech. Seminar Report: Recycling of PlasticsAkhil KumarNo ratings yet
- LLM For QnA ProposalDocument12 pagesLLM For QnA ProposalAkhil KumarNo ratings yet
- Application ProformaDocument2 pagesApplication ProformaAkhil KumarNo ratings yet
- B. Tech. Seminar Report: Recycling of PlasticsDocument31 pagesB. Tech. Seminar Report: Recycling of PlasticsAkhil KumarNo ratings yet
- Introduction To Plastic RecyclingDocument10 pagesIntroduction To Plastic RecyclingAkhil KumarNo ratings yet
- Introduction To Plastic RecyclingDocument10 pagesIntroduction To Plastic RecyclingAkhil KumarNo ratings yet
- MT 2Document18 pagesMT 2Akhil KumarNo ratings yet
- Plastic Waste: It'S Use in Construction of Roads: Kurmadasu Chandramouli, Allipilli Satyaveni, Mallampalli - Ch. G.SubashDocument6 pagesPlastic Waste: It'S Use in Construction of Roads: Kurmadasu Chandramouli, Allipilli Satyaveni, Mallampalli - Ch. G.SubashMAHESH A VNo ratings yet
- StackDocument48 pagesStackAkhil KumarNo ratings yet
- AkhilDocument2 pagesAkhilAkhil KumarNo ratings yet
- MT 2Document18 pagesMT 2Akhil KumarNo ratings yet
- Non-Ideal Flow: Residence Time DistributionDocument71 pagesNon-Ideal Flow: Residence Time DistributionAkhil KumarNo ratings yet
- Time Table End SemDocument2 pagesTime Table End SemAkhil KumarNo ratings yet
- BONAFIDE SCHAnnexure-IDocument1 pageBONAFIDE SCHAnnexure-IRafiq MirNo ratings yet
- PDC Es5Document18 pagesPDC Es5Akhil KumarNo ratings yet
- Assignment - Q1.Document14 pagesAssignment - Q1.Akhil KumarNo ratings yet
- PDC Es3Document25 pagesPDC Es3Akhil KumarNo ratings yet
- PDC Es1Document25 pagesPDC Es1Akhil KumarNo ratings yet
- Press Release 13 June 2023Document16 pagesPress Release 13 June 2023Newsinc 24No ratings yet
- Assignment - Q1.Document7 pagesAssignment - Q1.Akhil KumarNo ratings yet
- Bi 2Document2 pagesBi 2Akhil KumarNo ratings yet
- RTD Studies in CSTRDocument6 pagesRTD Studies in CSTRsri pragnaNo ratings yet
- Chemical Process Calculations: D.C. SikdarDocument11 pagesChemical Process Calculations: D.C. SikdarSharanappa ANo ratings yet
- Che 416 L5Document21 pagesChe 416 L5palmer okiemuteNo ratings yet
- CT Mid TermDocument2 pagesCT Mid TermAkhil KumarNo ratings yet
- MalachiteDocument2 pagesMalachiteAkhil KumarNo ratings yet
- Assignment 1 PDFDocument1 pageAssignment 1 PDFAkhil KumarNo ratings yet
- Assignment 4Document1 pageAssignment 4Akhil KumarNo ratings yet
- ACCSA Module 1 - 8 Practice Dimensions & Skillsets of Addiction CounsellingDocument148 pagesACCSA Module 1 - 8 Practice Dimensions & Skillsets of Addiction Counsellingskye42817No ratings yet
- Social Change Theme in The Cherry Orchard - LitChartsDocument17 pagesSocial Change Theme in The Cherry Orchard - LitChartsShivashankar. DNo ratings yet
- Yogesh Kadam (ABC)Document5 pagesYogesh Kadam (ABC)vipin HNo ratings yet
- 430D Backhoe LoaderDocument8 pages430D Backhoe LoaderRaul GuaninNo ratings yet
- Kompilasi Soal Paket BDocument10 pagesKompilasi Soal Paket Babdul wahidNo ratings yet
- CHAPTER 5 Work MeasurementDocument24 pagesCHAPTER 5 Work MeasurementAiman SupniNo ratings yet
- PATMD-LW Series Trifold 20200212Document2 pagesPATMD-LW Series Trifold 20200212Taacsa MatrizNo ratings yet
- Ivin Resume Nov 2022Document1 pageIvin Resume Nov 2022Ivin KuriakoseNo ratings yet
- Sokkia MagnetDocument9 pagesSokkia Magnetbbutros_317684077No ratings yet
- 66 Essential Phrasal Verbs EnglishDocument6 pages66 Essential Phrasal Verbs EnglishNarcisVega100% (15)
- Halftrack Track Chains InstructionsDocument4 pagesHalftrack Track Chains Instructionsddlevy0% (1)
- Pantos 16: Panoramic X-Ray SystemDocument6 pagesPantos 16: Panoramic X-Ray SystemAlbaz BiomedNo ratings yet
- Voting BehaviorDocument23 pagesVoting BehaviorWela Paing FallitangNo ratings yet
- MAPEH (AutoRecovered)Document12 pagesMAPEH (AutoRecovered)Mark Jerome MontañoNo ratings yet
- Distress Manual PDFDocument51 pagesDistress Manual PDFEIRINI ZIGKIRIADOUNo ratings yet
- GSKDocument22 pagesGSKChaudhary Hassan ArainNo ratings yet
- MGT-01 (14.03.23) - QPDocument19 pagesMGT-01 (14.03.23) - QPSrinivas VakaNo ratings yet
- Model Teaching CompetenciesDocument12 pagesModel Teaching CompetenciesTeachers Without BordersNo ratings yet
- Date CalcDocument8 pagesDate CalcPaolaNo ratings yet
- Assignment CM Final PDFDocument9 pagesAssignment CM Final PDFRefisa JiruNo ratings yet
- Jeff Nippard's Workout Routine & Diet (2022) - Jacked GorillaDocument11 pagesJeff Nippard's Workout Routine & Diet (2022) - Jacked Gorillaticoninx100% (1)
- Building A HA SmartConnector Cluster-V2.0.6Document35 pagesBuilding A HA SmartConnector Cluster-V2.0.6Ranadeep BhattacahrayaNo ratings yet
- Jasa Marga TBK - Billingual - 31 - Des - 2018 - JSMR PDFDocument227 pagesJasa Marga TBK - Billingual - 31 - Des - 2018 - JSMR PDFSjamsulHarunNo ratings yet
- Cost ActivityDocument6 pagesCost ActivityDeepak PahujaNo ratings yet
- Filcro - LabrevDocument19 pagesFilcro - LabrevKim ArniñoNo ratings yet
- MQ SSL/TLS Channels Including V8 ChangesDocument23 pagesMQ SSL/TLS Channels Including V8 ChangesAnkit GuptaNo ratings yet
- KV Admission EnclosureDocument1 pageKV Admission EnclosureLaishram PilotNo ratings yet
- Seven Keys To Church GrowthDocument4 pagesSeven Keys To Church GrowthJob0% (1)
- Case Study 6Document6 pagesCase Study 6Shaikh BilalNo ratings yet
- 05 N141 31673Document21 pages05 N141 31673priya thakurNo ratings yet