You might also like
- Foot and Mouth DiseaseDocument5 pagesFoot and Mouth Diseaseelvhynd beiNo ratings yet
- Waste World PDFDocument290 pagesWaste World PDFCat of Many Faces67% (3)
- Reptilian and Amphibious Diseases Found in Captivity FinalDocument12 pagesReptilian and Amphibious Diseases Found in Captivity Finalapi-250146149No ratings yet
- Orange BookDocument43 pagesOrange BookbiosiriNo ratings yet
- NCD Proof PDFDocument2 pagesNCD Proof PDFAnonymous TDzUwCg67% (3)
- PERSONALITY DEVELOPMENT CHAPTER 1 MaemaeDocument11 pagesPERSONALITY DEVELOPMENT CHAPTER 1 MaemaeFreshDianne Mhilkie Silvosa100% (1)
- Aqa A2 Biology LDRDocument21 pagesAqa A2 Biology LDRjames100% (4)
- Flagellates (New Version) PDFDocument91 pagesFlagellates (New Version) PDFjan9paeiamsubNo ratings yet
- Bacillary Dysentery RirisDocument27 pagesBacillary Dysentery Ririslutfia papitaNo ratings yet
- Eddy Current Testing in NDTDocument43 pagesEddy Current Testing in NDTMeby Selvaraj RNo ratings yet
- Prof Retno - Opportunistic Infections in AIDS EditDocument56 pagesProf Retno - Opportunistic Infections in AIDS EditMichael TambunanNo ratings yet
- 24 Basic Tai Chi Chuan (Yang Style) : Relaxation and HarmonyDocument2 pages24 Basic Tai Chi Chuan (Yang Style) : Relaxation and HarmonyDharma LingamNo ratings yet
- Answer Key Grade Six: Weathering and Erosion: Multiple Choice: (4 Points Each)Document5 pagesAnswer Key Grade Six: Weathering and Erosion: Multiple Choice: (4 Points Each)emmanuel richardNo ratings yet
- Lumpy Skin Disease: A Field Manual for VeterinariansFrom EverandLumpy Skin Disease: A Field Manual for VeterinariansNo ratings yet
- Fiebre AmarillaDocument5 pagesFiebre AmarillaLaDeKoC YoutuberNo ratings yet
- Yersinia Pestis Infection WithDocument5 pagesYersinia Pestis Infection WithMustixaNo ratings yet
- Diagnostic of LeptospiraDocument6 pagesDiagnostic of LeptospiraCaba MagdalenaNo ratings yet
- Listeria Monocytogenes Infection WithDocument6 pagesListeria Monocytogenes Infection WithKNo ratings yet
- Bluetongue 2Document5 pagesBluetongue 2Nancy HernándezNo ratings yet
- Rest SlidesDocument44 pagesRest SlidesMohed LipanNo ratings yet
- L3 - Enterobactericiae SPPDocument23 pagesL3 - Enterobactericiae SPPbujalkanNo ratings yet
- Typhoid Fever,-WPS OfficeDocument5 pagesTyphoid Fever,-WPS OfficeElvisNo ratings yet
- Vibrio CholeraeDocument5 pagesVibrio CholeraebloodstoragecentersuryaNo ratings yet
- Campylobacter PDFDocument78 pagesCampylobacter PDFKhushi PatelNo ratings yet
- Lecture 6 - Viruses Causing GastroenteritisDocument22 pagesLecture 6 - Viruses Causing GastroenteritisJeanPaule JoumaaNo ratings yet
- 48 Foot and Mouth DiseaseDocument20 pages48 Foot and Mouth DiseaseUsman Haider BuzdarNo ratings yet
- Kuliah Cestode & Trematode (Hand-Out)Document13 pagesKuliah Cestode & Trematode (Hand-Out)made yogaNo ratings yet
- Sarcoptes Scabiei (Infection With)Document4 pagesSarcoptes Scabiei (Infection With)Dinna KarlinaNo ratings yet
- MicrobiologyDocument6 pagesMicrobiologyDerek AtienzaNo ratings yet
- Leptospirosis Case Study (Short)Document16 pagesLeptospirosis Case Study (Short)Liryc Ernest CuerboNo ratings yet
- Zoonosis Revised 2016Document48 pagesZoonosis Revised 2016Yan Sheng HoNo ratings yet
- 17 FfsfafDocument78 pages17 FfsfafAndres Zambrano ArteagaNo ratings yet
- Hepatitis A VirusDocument4 pagesHepatitis A VirusEduardo Ramirez LasoNo ratings yet
- GiardiasisDocument16 pagesGiardiasismehrshad Farahpour Gp5No ratings yet
- Git T13 2024Document17 pagesGit T13 2024myarjddbzNo ratings yet
- The Reoviridae Family: by Luka, Mela IluDocument49 pagesThe Reoviridae Family: by Luka, Mela IluMela LukaNo ratings yet
- Swine Vesicular DiseaseDocument4 pagesSwine Vesicular DiseaseJohn Paul BlancaNo ratings yet
- Dipiro 8 ParasitDocument12 pagesDipiro 8 ParasitErik Firman RusdiantoNo ratings yet
- Feaco-Oral Infections 1Document32 pagesFeaco-Oral Infections 1Maria PavlovaNo ratings yet
- GIT InfectionDocument43 pagesGIT InfectionRaja RuzannaNo ratings yet
- Shigella: The Organism/ToxinDocument3 pagesShigella: The Organism/ToxinEduardo Ramirez LasoNo ratings yet
- Lumpy Skin Disease FinalDocument5 pagesLumpy Skin Disease FinalrohishaakNo ratings yet
- 9th Lec. Enterobacteriaceae Part 2 and Pseudo2023.Document30 pages9th Lec. Enterobacteriaceae Part 2 and Pseudo2023.Alex AlexNo ratings yet
- Shigella SPP, Vibrio SPPDocument6 pagesShigella SPP, Vibrio SPPtomal7811islamNo ratings yet
- Listeria HealthsafetyDocument3 pagesListeria HealthsafetyAzzedine BakaNo ratings yet
- Protozoal Gastrointestinal InfectionsDocument3 pagesProtozoal Gastrointestinal InfectionssivaNo ratings yet
- HGJK J LHB, JKDocument4 pagesHGJK J LHB, JKChandra Noor RachmanNo ratings yet
- Intestinal CestodaDocument62 pagesIntestinal CestodaadeshindyNo ratings yet
- Yersinia and Vibrio Associated DiseaseDocument19 pagesYersinia and Vibrio Associated DiseaseCurious PersonNo ratings yet
- Haccp Nacmcf 1997 HazardsDocument74 pagesHaccp Nacmcf 1997 HazardsAkramZakiNo ratings yet
- Foot and Mouth Disease: AetiologyDocument6 pagesFoot and Mouth Disease: Aetiology1938 MANOJ R BHARADWAJNo ratings yet
- Diarreia Do ViajanteDocument8 pagesDiarreia Do ViajanteAndreia RibeiroNo ratings yet
- Neisseria Gonorrhoeae, Sometimes Called The: I. DefinitionDocument16 pagesNeisseria Gonorrhoeae, Sometimes Called The: I. DefinitionBerle Joy VillanuevaNo ratings yet
- PARAGONIMIASISDocument21 pagesPARAGONIMIASISaNo ratings yet
- Diarrhea in Kittens and Young Cats - WSAVA2011 - VINDocument4 pagesDiarrhea in Kittens and Young Cats - WSAVA2011 - VINkukuhamru19No ratings yet
- Classification of RotavirusDocument74 pagesClassification of RotavirusAnupama S BNo ratings yet
- Informe HidatidosisDocument5 pagesInforme HidatidosisLeonardo Anthony Pérez SilvestreNo ratings yet
- Chapter 53 Intestinal CestodesDocument51 pagesChapter 53 Intestinal CestodesbartsnewNo ratings yet
- Balantidium Coli: Compiled by PB Wadigamangawa School of MLT, PeradeniyaDocument45 pagesBalantidium Coli: Compiled by PB Wadigamangawa School of MLT, Peradeniyawadige4668No ratings yet
- Intestinal Cestodes: DR Mohiedden M Abdul-FattahDocument27 pagesIntestinal Cestodes: DR Mohiedden M Abdul-FattahMicroscopeGeekNo ratings yet
- Diagnosis and Patophysiology OF Typhoid Fever: Nuzirwan Acang Faculty of Medicine Islamic University BandungDocument22 pagesDiagnosis and Patophysiology OF Typhoid Fever: Nuzirwan Acang Faculty of Medicine Islamic University BandungUci MarleyNo ratings yet
- Enterobius: Anti-Infective AgentsDocument11 pagesEnterobius: Anti-Infective AgentsIonela VișinescuNo ratings yet
- Giardiasis Dan LeismaniaDocument39 pagesGiardiasis Dan LeismaniaSurya PradnyaNo ratings yet
- Ebola VirusDocument19 pagesEbola Virusdelwin yuNo ratings yet
- Parasitology Lecture 2Document85 pagesParasitology Lecture 2Dr Sarah Bakhsh - Resident FCPS Community MedicineNo ratings yet
- Artículo 1 GiardiasisDocument11 pagesArtículo 1 GiardiasisJonathan Paul Ramirez RodríguezNo ratings yet
- Datasheet: Pathogenic Bacteria:: Staphylococcus AureusDocument2 pagesDatasheet: Pathogenic Bacteria:: Staphylococcus AureusDutch CharmingNo ratings yet
- IMV-QP-PVD-05 (Evaluation of Supplier) - Rev2Document5 pagesIMV-QP-PVD-05 (Evaluation of Supplier) - Rev2ori wahyuniNo ratings yet
- Surface Vehicle Standard: Rev. JAN95Document28 pagesSurface Vehicle Standard: Rev. JAN95john georgeNo ratings yet
- Juri MCQDocument6 pagesJuri MCQmukul sidhqueNo ratings yet
- Hiranandani Warehouse Building, Janapanchatram, Box-2, TamilnaduDocument6 pagesHiranandani Warehouse Building, Janapanchatram, Box-2, TamilnaduRashmi Ranjan RoutNo ratings yet
- Elementary Lesson 1Document4 pagesElementary Lesson 1Gabriela DenisNo ratings yet
- C V - RajiDocument2 pagesC V - RajiUpender VanamNo ratings yet
- PIS - J512 No Rinse SanitiserDocument2 pagesPIS - J512 No Rinse SanitiserMannuNo ratings yet
- Topic 3 Teacher - S Roles As A CounsellorDocument19 pagesTopic 3 Teacher - S Roles As A Counsellorlky411No ratings yet
- GEHC Brochure OEC Brivo Plus C Arm The Confident ChoiceDocument8 pagesGEHC Brochure OEC Brivo Plus C Arm The Confident ChoiceGANESHNo ratings yet
- Day 1 - Introduction To Mobile CommunicationDocument16 pagesDay 1 - Introduction To Mobile CommunicationMichelle NyamupanemundaNo ratings yet
- Thermo Scientific Forma High-Performance Laboratory Refrigerators and FreezersDocument22 pagesThermo Scientific Forma High-Performance Laboratory Refrigerators and FreezerswhoisvicksNo ratings yet
- AmbergrisDocument4 pagesAmbergriskaram deolNo ratings yet
- Prostitution Intervention ProjectDocument7 pagesProstitution Intervention Projectchrisr310No ratings yet
- Bid SheetDocument10 pagesBid SheetVi KraNo ratings yet
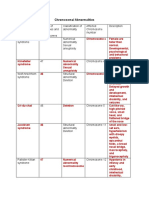
- Table On Chromosomal AbnormalitiesDocument3 pagesTable On Chromosomal AbnormalitiesJoanne Mary RomoNo ratings yet
- StreakingDocument2 pagesStreakingMar MacaranasNo ratings yet
- AIATSDocument74 pagesAIATSAtindra NathGanguly67% (6)
- Declaration: Document Updated 9 June 2011Document16 pagesDeclaration: Document Updated 9 June 2011Pippa McFallNo ratings yet
- 1 Land Rover Freelander MY2001 Parking Heater Install TD4Document4 pages1 Land Rover Freelander MY2001 Parking Heater Install TD4Florin ConstantinNo ratings yet
- CP Carina-Td-9036629-EnDocument40 pagesCP Carina-Td-9036629-EnDu Phạm QuangNo ratings yet
- Postpartum Clinical Prep SheetDocument3 pagesPostpartum Clinical Prep SheetKurata432No ratings yet
- Arya Petroleum International (API) Located in Harmriya Free Zone-UAEDocument2 pagesArya Petroleum International (API) Located in Harmriya Free Zone-UAEKaushal SutariaNo ratings yet