You might also like
- From Crisis to Catastrophe: Care, COVID, and Pathways to ChangeFrom EverandFrom Crisis to Catastrophe: Care, COVID, and Pathways to ChangeNo ratings yet
- (2022) Strategies That Promote Equity in COVID-19 Vaccine Uptake For Undocumented Immigrants - A ReviewDocument9 pages(2022) Strategies That Promote Equity in COVID-19 Vaccine Uptake For Undocumented Immigrants - A Reviewse parkNo ratings yet
- COVID 19, Misinformation and Disinformation: An Analysis of Nigerians' Perception of Social Media Health Awareness CampaignsDocument22 pagesCOVID 19, Misinformation and Disinformation: An Analysis of Nigerians' Perception of Social Media Health Awareness CampaignsPeter EgielewaNo ratings yet
- Negotiating Pharmaceutical Uncertainty: Women's Agency in a South African HIV Prevention TrialFrom EverandNegotiating Pharmaceutical Uncertainty: Women's Agency in a South African HIV Prevention TrialNo ratings yet
- The Impact of Misinformation and Educational Attainment in The Vaccine Hesitancy of The FilipinosDocument56 pagesThe Impact of Misinformation and Educational Attainment in The Vaccine Hesitancy of The FilipinosvenusmonteverosNo ratings yet
- UntitledDocument26 pagesUntitledBryen GarciaNo ratings yet
- Misinformation of COVID 19 Vaccines and Vaccine Hesitancy: Sun Kyong Lee, Juhyung Sun, Seulki Jang & Shane ConnellyDocument11 pagesMisinformation of COVID 19 Vaccines and Vaccine Hesitancy: Sun Kyong Lee, Juhyung Sun, Seulki Jang & Shane ConnellyCharm LopezNo ratings yet
- Factors Affecting Differences in Attitudes Towards Covid - 19 VaccinationDocument8 pagesFactors Affecting Differences in Attitudes Towards Covid - 19 Vaccinationbien groyonNo ratings yet
- Understanding Risk Communication For Prevention and Control of Vector-Borne Diseases: A Mixed-Method Study in Curac AoDocument22 pagesUnderstanding Risk Communication For Prevention and Control of Vector-Borne Diseases: A Mixed-Method Study in Curac AoAbel Abelito Jimenez Jimenez Jr.No ratings yet
- Misinformation, Believability, and Vaccine Acceptance Over 40 Countries Takeaways From The Initial Phase of The COVID-19 InfodemicDocument35 pagesMisinformation, Believability, and Vaccine Acceptance Over 40 Countries Takeaways From The Initial Phase of The COVID-19 InfodemicHosam GomaaNo ratings yet
- Association of Individual Health Literacy With Preventive Behaviours and Family Well-Being During COVID-19 Pandemic - Mediating Role of Family Information Sharing.Document10 pagesAssociation of Individual Health Literacy With Preventive Behaviours and Family Well-Being During COVID-19 Pandemic - Mediating Role of Family Information Sharing.MYNo ratings yet
- Literature Review On Hiv InfectionDocument7 pagesLiterature Review On Hiv Infectionafdtunqho100% (1)
- Research Paper About Aids in AfricaDocument13 pagesResearch Paper About Aids in Africafzg9e1r9100% (1)
- IJRPR15690Document6 pagesIJRPR15690WOYOPWA SHEMNo ratings yet
- Substance Use Disorders and Telehealth in The COVID-19 Pandemic Era: A New OutlookDocument10 pagesSubstance Use Disorders and Telehealth in The COVID-19 Pandemic Era: A New OutlookRo M OyarzúnNo ratings yet
- Utilizing Evidence-Based Decision Making in Responding Public Health EmergencyDocument18 pagesUtilizing Evidence-Based Decision Making in Responding Public Health EmergencyInternational Journal of Innovative Science and Research Technology100% (1)
- Chapter 1 PR1Document11 pagesChapter 1 PR1Nanami MumuzunoNo ratings yet
- Lived Experiences of Individuals With Sexually Transmitted Infections (STIs) : An Input To Infectious Disease Awareness and PreventionDocument12 pagesLived Experiences of Individuals With Sexually Transmitted Infections (STIs) : An Input To Infectious Disease Awareness and PreventionPsychology and Education: A Multidisciplinary JournalNo ratings yet
- The COVID-19 Response: The Vital Role of the Public Health ProfessionalFrom EverandThe COVID-19 Response: The Vital Role of the Public Health ProfessionalNo ratings yet
- 11th R.LDocument24 pages11th R.LWilliam Tac anNo ratings yet
- Coronavirus Disease 2019: Covid-19 Pandemic, States of Confusion and Disorderliness of the Public Health Policy-making ProcessFrom EverandCoronavirus Disease 2019: Covid-19 Pandemic, States of Confusion and Disorderliness of the Public Health Policy-making ProcessNo ratings yet
- Anti-Vaccine Behavior of Serbian AdultsDocument8 pagesAnti-Vaccine Behavior of Serbian AdultsSITI SARAH AHMAD JAMILNo ratings yet
- Influencing Factors of Understanding COVID-19 Risks and Coping Behaviors Among The Elderly PopulationDocument16 pagesInfluencing Factors of Understanding COVID-19 Risks and Coping Behaviors Among The Elderly PopulationMäê MedrosoNo ratings yet
- Vaccine Hesitancy in China: A Qualitative Study of Stakeholders' PerspectivesDocument15 pagesVaccine Hesitancy in China: A Qualitative Study of Stakeholders' PerspectivesEliNo ratings yet
- Review of Related LiteratureDocument16 pagesReview of Related LiteratureHavier EsparagueraNo ratings yet
- Knowledge Attitude and Risk Perception of COVID 19 in Rural Ghana A ViewpointDocument6 pagesKnowledge Attitude and Risk Perception of COVID 19 in Rural Ghana A ViewpointAthenaeum Scientific PublishersNo ratings yet
- Literature Review On Hiv Aids in KenyaDocument8 pagesLiterature Review On Hiv Aids in Kenyapabup1hebyl2100% (1)
- 5365 Project FinalDocument13 pages5365 Project FinalDIVYA RANI KOLLINo ratings yet
- Theoretical FrameworkDocument2 pagesTheoretical FrameworkljgerzonNo ratings yet
- C E G H T: T ' N B T T N !: Losing The Ducational Ap On Uman Rafficking Here S O Etter IME HAN OWDocument16 pagesC E G H T: T ' N B T T N !: Losing The Ducational Ap On Uman Rafficking Here S O Etter IME HAN OWapi-572425899No ratings yet
- Resea CR H Report ProposalDocument5 pagesResea CR H Report ProposalLigsay, Dianne Rose N.No ratings yet
- Cidrap Covid19 Viewpoint Part4Document12 pagesCidrap Covid19 Viewpoint Part4ljing4No ratings yet
- Banana Pseudostem Fiber Its Feasibility As A Raw Material For Paper Bag Production (1) (Autosaved)Document14 pagesBanana Pseudostem Fiber Its Feasibility As A Raw Material For Paper Bag Production (1) (Autosaved)Rubilee GanoyNo ratings yet
- The Impact of Fake News On Social Media and Its Influence On Health During The COVID-19 Pandemic A Systematic ReviewDocument11 pagesThe Impact of Fake News On Social Media and Its Influence On Health During The COVID-19 Pandemic A Systematic ReviewZach Daniel Dela CruzNo ratings yet
- The Effects of Social Media Use On Preventive Behaviors During Infectious Disease Outbreaks The Mediating Role of Self Relevant Emotions and PublicDocument11 pagesThe Effects of Social Media Use On Preventive Behaviors During Infectious Disease Outbreaks The Mediating Role of Self Relevant Emotions and PublicHooman BNo ratings yet
- Mheidly-Fares2020 Article LeveragingMediaAndHealthCommunDocument11 pagesMheidly-Fares2020 Article LeveragingMediaAndHealthCommunDorina TicuNo ratings yet
- Degree of Acceptance of Residents Barangay Bibincahan To Vaccination Program of The Philippine GovernmentDocument24 pagesDegree of Acceptance of Residents Barangay Bibincahan To Vaccination Program of The Philippine GovernmentRJ DealcaNo ratings yet
- 1 - Phenomenon of Depression and Anxiety Related To PrecautionsDocument5 pages1 - Phenomenon of Depression and Anxiety Related To PrecautionsHazhar BlbasNo ratings yet
- Simulacion de Fakes News en EpidemiasDocument10 pagesSimulacion de Fakes News en EpidemiasjavenacostaNo ratings yet
- Consideracion Bioeticas en La Investigacion Filogenetica Del VihDocument11 pagesConsideracion Bioeticas en La Investigacion Filogenetica Del VihJulio Cesar Nilo Polo SamillánNo ratings yet
- Summary of The Truth about COVID-19 by Joseph Mercola and Ronnie Cummins:Exposing the Great Reset, Lockdowns, Vaccine Passports, and the New Normal: A Comprehensive SummaryFrom EverandSummary of The Truth about COVID-19 by Joseph Mercola and Ronnie Cummins:Exposing the Great Reset, Lockdowns, Vaccine Passports, and the New Normal: A Comprehensive SummaryNo ratings yet
- Myths COVIDDocument19 pagesMyths COVIDPGNo ratings yet
- Hiv Virus Research PaperDocument4 pagesHiv Virus Research Papergmannevnd100% (1)
- Research Gap: Despite The Proliferation of False Information in Social Media Which May Have DirectDocument31 pagesResearch Gap: Despite The Proliferation of False Information in Social Media Which May Have DirectNUR-HATHI SANAANINo ratings yet
- Avoidance of InformationDocument14 pagesAvoidance of InformationHassan NadeemNo ratings yet
- CHAPTER 1-WPS OfficeDocument5 pagesCHAPTER 1-WPS OfficeAbdulrahman Abarani AdamNo ratings yet
- The Inequality of COVID-19: Immediate Health Communication, Governance and Response in Four Indigenous RegionsFrom EverandThe Inequality of COVID-19: Immediate Health Communication, Governance and Response in Four Indigenous RegionsNo ratings yet
- Leveraging Media Informatics For The Surveillance and Understanding of Disease OutbreaksDocument9 pagesLeveraging Media Informatics For The Surveillance and Understanding of Disease OutbreaksNerine Buter-BlaxellNo ratings yet
- RESEARCH 1 Fi 2Document20 pagesRESEARCH 1 Fi 2Alondra SagarioNo ratings yet
- Summary of Brian Tyson, George Fareed & Mathew Crawford's Overcoming the COVID DarknessFrom EverandSummary of Brian Tyson, George Fareed & Mathew Crawford's Overcoming the COVID DarknessNo ratings yet
- 1 s2.0 S2667321522000075 MainDocument6 pages1 s2.0 S2667321522000075 MainNeal TorwaneNo ratings yet
- Research Paper Outline On Hiv AidsDocument4 pagesResearch Paper Outline On Hiv Aidsc9rz4vrm100% (1)
- Defining Rights-Based Indicators For HIV Epidemic TransitionDocument7 pagesDefining Rights-Based Indicators For HIV Epidemic TransitionDanylo VianaNo ratings yet
- 13th R.LDocument9 pages13th R.LWilliam Tac anNo ratings yet
- Personality and Individual Differences: Heng LiDocument6 pagesPersonality and Individual Differences: Heng LiAndre SiahaanNo ratings yet
- Nimr Bibliography On Covid19Document92 pagesNimr Bibliography On Covid19sogetobi0No ratings yet
- Jurnal KesmasDocument6 pagesJurnal KesmasolaNo ratings yet
- What Promotes Cognitive Dissonance Among Anti-Vaccine Members in Indonesia?Document12 pagesWhat Promotes Cognitive Dissonance Among Anti-Vaccine Members in Indonesia?IJPHSNo ratings yet
- Disease, Death and Control: Missionary Medicine in Colonial ODISHA (1900-1940)Document12 pagesDisease, Death and Control: Missionary Medicine in Colonial ODISHA (1900-1940)TJPRC PublicationsNo ratings yet
- Agar Gel Precipitation...Document47 pagesAgar Gel Precipitation...fedhawakNo ratings yet
- Pediatrics ArimgsasDocument403 pagesPediatrics ArimgsasGabriela ChristianNo ratings yet
- Klasifikasi Tscherne Open Soft-Tissue InjuryDocument2 pagesKlasifikasi Tscherne Open Soft-Tissue InjuryAnggita Efipania Silambi'No ratings yet
- Precipath CK-MB.04362349001.V6.en PDFDocument2 pagesPrecipath CK-MB.04362349001.V6.en PDFARIF AHAMMED PNo ratings yet
- Pdo Health Hazard Inventory 2015decemberDocument274 pagesPdo Health Hazard Inventory 2015decemberrwerwerwNo ratings yet
- Basic Concepts On Laboratory Biosafety and BiosecurityDocument3 pagesBasic Concepts On Laboratory Biosafety and BiosecurityGwynneth EuriccaNo ratings yet
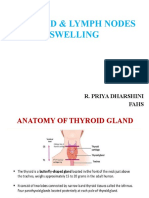
- Thyroid & Lymph NodesDocument44 pagesThyroid & Lymph NodesSarah CornerNo ratings yet
- Pneumonia, COPD, Tuberculosis - ReportDocument23 pagesPneumonia, COPD, Tuberculosis - ReportJoceelyyn EufemianoNo ratings yet
- Para 311 Lec Week 3Document81 pagesPara 311 Lec Week 3jeijai0827No ratings yet
- Lesson Plan: Achievement ObjectivesDocument4 pagesLesson Plan: Achievement ObjectivesAnonymous bStw5dNo ratings yet
- Tuberculosis: Dr.V. Gangadharan Professor & Hod Department of Respiratory Medicine Saveetha Medical College HospitalDocument58 pagesTuberculosis: Dr.V. Gangadharan Professor & Hod Department of Respiratory Medicine Saveetha Medical College HospitalJoanna RachelNo ratings yet
- Infectious Control Measures (Dental Clinic)Document7 pagesInfectious Control Measures (Dental Clinic)Susan JilhanoNo ratings yet
- U1 The Human Body 5Document12 pagesU1 The Human Body 5Francisco RosNo ratings yet
- Health Problems Vocabulary Matching Exercise ESL Worksheets For Kids and New Learners 2122Document2 pagesHealth Problems Vocabulary Matching Exercise ESL Worksheets For Kids and New Learners 2122Beatriz MoraisNo ratings yet
- Ficha Tecnica Dengue Duo SDDocument2 pagesFicha Tecnica Dengue Duo SDDanitxa Leyva100% (1)
- Exam Syllabus For DN Intake July 2018Document22 pagesExam Syllabus For DN Intake July 2018Igga Peter ayaNo ratings yet
- Bacteriology SummaryDocument38 pagesBacteriology SummaryMohsen HaleemNo ratings yet
- Ficus: Bacterial ProblemsDocument7 pagesFicus: Bacterial Problemsioanadelia1972No ratings yet
- Q1 M1 Gr.7Document39 pagesQ1 M1 Gr.7Rowena PaguiaNo ratings yet
- Drug Study - CefpodoximeDocument4 pagesDrug Study - CefpodoximeIzza DeloriaNo ratings yet
- Community-Acquired Pneumonia PathophysiologyDocument2 pagesCommunity-Acquired Pneumonia PathophysiologyFrancis Adrian83% (12)
- World Health Organization (WHO)Document23 pagesWorld Health Organization (WHO)Abhishek Verma100% (1)
- Transcript of The Videotelephony Medical Examination ReportDocument2 pagesTranscript of The Videotelephony Medical Examination ReportKamarapu Vamshee KrishnaNo ratings yet
- ACTIVITY NO - 2 - MycologyDocument17 pagesACTIVITY NO - 2 - MycologysofiaNo ratings yet
- 1.public Health Importance, Common RTI, STIDocument42 pages1.public Health Importance, Common RTI, STIJobin Thomas100% (1)
- Articulo de e Coli en InglesDocument3 pagesArticulo de e Coli en Inglesjuan gonzalezNo ratings yet
- Infection Control (Q & A)Document27 pagesInfection Control (Q & A)Dr. Bimal Hospital Private LimitedNo ratings yet
- Pulmonary TBDocument13 pagesPulmonary TBAmanda ScarletNo ratings yet
- Deacon Scott J. Conway Rhonda Rose Theresa LittleDocument2 pagesDeacon Scott J. Conway Rhonda Rose Theresa LittleActionNewsJaxNo ratings yet