You might also like
- WHO Ladder 20anosdepois PDFDocument4 pagesWHO Ladder 20anosdepois PDFIahel ManonNo ratings yet
- Analgesic Ladder Therapeutic EducationDocument7 pagesAnalgesic Ladder Therapeutic Educationfaciola hepaticaNo ratings yet
- Who Analgesic LadderDocument55 pagesWho Analgesic LadderSyifa Nurul Asma'No ratings yet
- A New Concept For Pain ManagementDocument5 pagesA New Concept For Pain ManagementNeurologi FK UKINo ratings yet
- Opiod RotationDocument9 pagesOpiod RotationboboNo ratings yet
- Final Approved Guidelines For The Drug Treatment of Pain in Primary Care Version 50 1494493393Document15 pagesFinal Approved Guidelines For The Drug Treatment of Pain in Primary Care Version 50 1494493393zebun nahar BushraNo ratings yet
- Pain Thesis PDFDocument7 pagesPain Thesis PDFafcnzcrcf100% (2)
- Pharmacological Management of Cancer-Related Pain: Photo Courtesy of Lisa Scholder. Solid Stance. 16" × 24"Document14 pagesPharmacological Management of Cancer-Related Pain: Photo Courtesy of Lisa Scholder. Solid Stance. 16" × 24"I Made AryanaNo ratings yet
- WHO Analgesic Ladder: Aabha A. Anekar Marco CascellaDocument5 pagesWHO Analgesic Ladder: Aabha A. Anekar Marco CascellaKessi VikaneswariNo ratings yet
- Schuster 2018Document23 pagesSchuster 2018Poly ArenaNo ratings yet
- Use of Strong Opioids in Advanced Cancer Pain: A Randomized TrialDocument8 pagesUse of Strong Opioids in Advanced Cancer Pain: A Randomized TrialFran WermannNo ratings yet
- Nej MP 1512932Document3 pagesNej MP 1512932anggiNo ratings yet
- Pain ManagementDocument2 pagesPain Managementfaith2rescoberNo ratings yet
- Pharmacologic Management of Neuropathic Pain ENGverDocument138 pagesPharmacologic Management of Neuropathic Pain ENGvermagreaNo ratings yet
- WHO Analgesic Ladder - StatPearls - NCBI BookshelfDocument5 pagesWHO Analgesic Ladder - StatPearls - NCBI BookshelfmagreaNo ratings yet
- Managing PostoperativeDocument9 pagesManaging PostoperativeWardah Fauziah El SofwanNo ratings yet
- Low Back Pain and Radicular PainDocument9 pagesLow Back Pain and Radicular PainrikasariNo ratings yet
- Hipnosis Estudio Piloto Holanda 1988Document6 pagesHipnosis Estudio Piloto Holanda 1988Gracia DelgadoNo ratings yet
- Pain Community Centre - Who Analgesic Ladder - 2011-03-15Document3 pagesPain Community Centre - Who Analgesic Ladder - 2011-03-15Karina WibowoNo ratings yet
- Postoperative Pain Control: Veerabhadram Garimella, MD, MRCS Christina Cellini, MDDocument6 pagesPostoperative Pain Control: Veerabhadram Garimella, MD, MRCS Christina Cellini, MDBani ZakiyahNo ratings yet
- Dolor Abdominal 1Document12 pagesDolor Abdominal 1likata07No ratings yet
- Canjclin 44 5 263Document42 pagesCanjclin 44 5 263I Made AryanaNo ratings yet
- Literature Review On Postoperative Pain ManagementDocument6 pagesLiterature Review On Postoperative Pain Managementea4c954qNo ratings yet
- JPR 10 2479Document10 pagesJPR 10 2479vanyoktavianiNo ratings yet
- WHO Analgesic LadderDocument2 pagesWHO Analgesic LadderAndi PakdheeNo ratings yet
- Multimodal Analgesia A CL 2022Document14 pagesMultimodal Analgesia A CL 2022Alejandra SanchezNo ratings yet
- WHO Analgesic LadderDocument2 pagesWHO Analgesic LadderAndi PakdheeNo ratings yet
- Thesis On Postoperative Pain ManagementDocument5 pagesThesis On Postoperative Pain ManagementOrderCustomPapersDesMoines100% (2)
- Pain Management Research PaperDocument6 pagesPain Management Research Paperafnhbijlzdufjj100% (1)
- Thesis Pain ManagementDocument8 pagesThesis Pain ManagementHelpInWritingPaperCanada100% (2)
- Falch Et Al-2014-European Journal of PainDocument13 pagesFalch Et Al-2014-European Journal of PainNur AiidaNo ratings yet
- Mki 053Document4 pagesMki 053I Made AryanaNo ratings yet
- Opioids in The Management of Persistent Non-Cancer PainDocument3 pagesOpioids in The Management of Persistent Non-Cancer Painafernandezd28No ratings yet
- JPR 14 1733Document12 pagesJPR 14 1733StivoNo ratings yet
- MDZ e DispnéiaDocument10 pagesMDZ e DispnéiaThaísa NogueiraNo ratings yet
- 2021 Article 1579Document45 pages2021 Article 1579Maria DanilaNo ratings yet
- Step LaddrDocument12 pagesStep LaddrSetyo RahmanNo ratings yet
- Research Paper Pain ManagementDocument6 pagesResearch Paper Pain Managementafnhdmovmtoddw100% (1)
- New Opioids: Ournal of Linical NcologyDocument6 pagesNew Opioids: Ournal of Linical Ncologyjuan tNo ratings yet
- The Argument For Enhanced Use of Complementary and Alternative Therapies in Chronic Pain ManagementDocument4 pagesThe Argument For Enhanced Use of Complementary and Alternative Therapies in Chronic Pain ManagementquadrospauloNo ratings yet
- Pain Management - A Decade's Perspective of A New SubspecialtyDocument8 pagesPain Management - A Decade's Perspective of A New SubspecialtyDavid PrivatNo ratings yet
- Lehmann 2005Document18 pagesLehmann 2005asdasdasdNo ratings yet
- P Acutepainmgmt PDFDocument3 pagesP Acutepainmgmt PDFEnrita DianNo ratings yet
- 3. Bài Báo Tiếng Anh Khác Tên Tác GiảDocument5 pages3. Bài Báo Tiếng Anh Khác Tên Tác GiảnamanesthesiaNo ratings yet
- Fpain 02 721357Document15 pagesFpain 02 721357goliath.chad2000No ratings yet
- Acute Pain Management in Patients With Opioid ToleranceDocument6 pagesAcute Pain Management in Patients With Opioid ToleranceHendrikus Surya Adhi PutraNo ratings yet
- Xxi BGCDocument116 pagesXxi BGCzicoparadigmaNo ratings yet
- Pain Management & Medicine: An Innovative Product For Pain Management: Proof From Clinical TrialDocument5 pagesPain Management & Medicine: An Innovative Product For Pain Management: Proof From Clinical TrialIkhdin SaadhiNo ratings yet
- The World Health Organization Three-Step Analgesic Ladder PDFDocument2 pagesThe World Health Organization Three-Step Analgesic Ladder PDFNanang HardiansyahNo ratings yet
- Efficacy Tolerability and Safety of Nonph Therapies For Chronic Pain CAMDocument15 pagesEfficacy Tolerability and Safety of Nonph Therapies For Chronic Pain CAMMiguel TrillosNo ratings yet
- Treatment of Neuropathic Pain An Overview of RecentDocument11 pagesTreatment of Neuropathic Pain An Overview of RecentIvette Silva FigueroaNo ratings yet
- Management of PainDocument6 pagesManagement of PainSinging MedicNo ratings yet
- Non-Pharmacological Methods and Post-Operative Pain Relief: An Observational StudyDocument7 pagesNon-Pharmacological Methods and Post-Operative Pain Relief: An Observational StudyAsti DwiningsihNo ratings yet
- Research Paper On Pain ManagementDocument6 pagesResearch Paper On Pain Managementc9sj0n70100% (1)
- Patients' Perception of Acute and Chronic Pain and Their Satisfaction With Care at The General Hospital DoualaDocument8 pagesPatients' Perception of Acute and Chronic Pain and Their Satisfaction With Care at The General Hospital DoualaEditor IJTSRDNo ratings yet
- Estudio 1.1 Patient-Perceived Benefit During One Year of Treatment With DoloteffinsDocument6 pagesEstudio 1.1 Patient-Perceived Benefit During One Year of Treatment With DoloteffinsLa Farmacia HomeopáticaNo ratings yet
- AnalgesicsDocument23 pagesAnalgesicsMuhammad SdiqNo ratings yet
- 2reconsidering Opioid Therapy Mar 2013Document6 pages2reconsidering Opioid Therapy Mar 2013Anonymous 4txA8N8etNo ratings yet
- The Routes of Administration For Acute Postoperative Pain MedicationDocument17 pagesThe Routes of Administration For Acute Postoperative Pain Medicationronald97hgNo ratings yet
- Handbook of Methadone Prescribing and Buprenorphine TherapyFrom EverandHandbook of Methadone Prescribing and Buprenorphine TherapyNo ratings yet
- LENS Skin Disorders 2324Document49 pagesLENS Skin Disorders 2324Zyrille Moira MaddumaNo ratings yet
- Sugar Free Shopping ListDocument4 pagesSugar Free Shopping Listhsquiers100% (3)
- NFPA Review of The Incident by Ken MastrulloDocument3 pagesNFPA Review of The Incident by Ken MastrullotatacpsNo ratings yet
- 中考英语100篇满分作文精讲(附万能写作句子)Document109 pages中考英语100篇满分作文精讲(附万能写作句子)qrh1950623825No ratings yet
- New Text DocumentDocument2 pagesNew Text DocumenteqweNo ratings yet
- Flux Cored Arc Welding NC IIDocument73 pagesFlux Cored Arc Welding NC IIAJ AcuñaNo ratings yet
- Research Proposal-1Document28 pagesResearch Proposal-1sowsthikaNo ratings yet
- AiepiDocument12 pagesAiepiRenzo Iván Marín DávalosNo ratings yet
- Feline Injection-Site Sarcoma - Todays Veterinary PracticeDocument12 pagesFeline Injection-Site Sarcoma - Todays Veterinary PracticeBla bla BlaNo ratings yet
- Plasma Metanephrine Test: Patient Information FactsheetDocument2 pagesPlasma Metanephrine Test: Patient Information FactsheetDamigart PremiumNo ratings yet
- Local Anaesthetics Mcqs From LouisDocument6 pagesLocal Anaesthetics Mcqs From LouisAmreen Khan100% (1)
- Basics of Therapeutic DietsDocument12 pagesBasics of Therapeutic DietstiruchanurNo ratings yet
- AIA IHS Clinics With TCM - Generic (120613)Document43 pagesAIA IHS Clinics With TCM - Generic (120613)junkaiiiNo ratings yet
- Microbial Limits Tests: The Difference Between "Absence of Objectionable Microorganisms" and "Absence of Specified Microorganisms"Document7 pagesMicrobial Limits Tests: The Difference Between "Absence of Objectionable Microorganisms" and "Absence of Specified Microorganisms"Jai MurugeshNo ratings yet
- Vi. Nursing Care PlanDocument11 pagesVi. Nursing Care PlanSamantha BolanteNo ratings yet
- What Concentration Is The Best To Kill GermsDocument3 pagesWhat Concentration Is The Best To Kill GermsAncaja, Jameir 1CNo ratings yet
- Drug Dispensing Practices at Pharmacies in Bengaluru: A Cross Sectional StudyDocument5 pagesDrug Dispensing Practices at Pharmacies in Bengaluru: A Cross Sectional StudySoumya RatnalaNo ratings yet
- Konsolidasi WelmiDocument72 pagesKonsolidasi WelmiWelmi Sulfatri IshakNo ratings yet
- Therapeutic PhlebotomyDocument2 pagesTherapeutic PhlebotomyAimee Howle BuchananNo ratings yet
- Surat Permintaan Obat Dinkes BaruDocument21 pagesSurat Permintaan Obat Dinkes BaruHafizh JhunkoNo ratings yet
- Good Practice Review - 8 - Revised2 PDFDocument323 pagesGood Practice Review - 8 - Revised2 PDFsteppevosNo ratings yet
- Cannabis-Infused Food and Canadian Consumers' Willingness To Consider "Recreational" Cannabis As A Food IngredientDocument7 pagesCannabis-Infused Food and Canadian Consumers' Willingness To Consider "Recreational" Cannabis As A Food IngredientCTV CalgaryNo ratings yet
- Gases Toxicos Irritantes PDFDocument6 pagesGases Toxicos Irritantes PDFLUIS ANDRES JUAREZ CALLENo ratings yet
- Catheter WiresDocument56 pagesCatheter WiresSaud ShirwanNo ratings yet
- Allan ALH105 Week 3Document5 pagesAllan ALH105 Week 3alvin mwizNo ratings yet
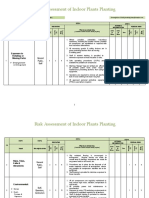
- Risk Assessment of Indoor Plants PlantingDocument5 pagesRisk Assessment of Indoor Plants Plantingطارق رضوانNo ratings yet
- Sensory Design of Easy-To-Chew Food For Elderly: - Ingredients and Manufacturing Conditions With Focus On Meat and CarrotDocument23 pagesSensory Design of Easy-To-Chew Food For Elderly: - Ingredients and Manufacturing Conditions With Focus On Meat and CarrotCaguioa Mark Anthony G.No ratings yet
- Hyoscine ButylbromideDocument2 pagesHyoscine ButylbromideKenneth ColeNo ratings yet
- Jonsen 4 Box MethodDocument5 pagesJonsen 4 Box MethodsawsanNo ratings yet