You might also like
- Mandibular Posterior Anatomic Limit For MolarDocument8 pagesMandibular Posterior Anatomic Limit For MolarRommy MelgarejoNo ratings yet
- Online Only Abstracts - YmodDocument5 pagesOnline Only Abstracts - YmodDr.Prakher SainiNo ratings yet
- Computed Tomography-Guided Bone Block Harvesting From The Mandibular RamusDocument6 pagesComputed Tomography-Guided Bone Block Harvesting From The Mandibular Ramusfer francoNo ratings yet
- Stability of Transverse Expansion in The Mandibular ArchDocument6 pagesStability of Transverse Expansion in The Mandibular ArchManena RivoltaNo ratings yet
- Evaluation of Marginal Alveolar Bone in The Anterior Mandible With Pretreatment and Posttreatment Computed Tomography in Nonextraction PatientsDocument10 pagesEvaluation of Marginal Alveolar Bone in The Anterior Mandible With Pretreatment and Posttreatment Computed Tomography in Nonextraction PatientsSoe San KyawNo ratings yet
- Retrospective Study of Maxillary Sinus Dimensions and Pneumatization in Adult Patients With An Anterior Open BiteDocument6 pagesRetrospective Study of Maxillary Sinus Dimensions and Pneumatization in Adult Patients With An Anterior Open BiteAntonio Pizarroso GonzaloNo ratings yet
- Quantitative Evaluation of Cortical BoneDocument6 pagesQuantitative Evaluation of Cortical Bonehector rinconNo ratings yet
- Evaluation of Mandibular First Molars' Axial Inclination and Alveolar Morphology in Different Facial Patterns: A CBCT StudyDocument10 pagesEvaluation of Mandibular First Molars' Axial Inclination and Alveolar Morphology in Different Facial Patterns: A CBCT StudyPututu PatataNo ratings yet
- Broadie 2Document12 pagesBroadie 2Stefana NanuNo ratings yet
- Dentofacial Changes From Fan-Type Rapid Maxillary Expansion Vs Traditional Rapid Maxillary Expansion in Early Mixed Dentition A Prospective Clinical TrialDocument9 pagesDentofacial Changes From Fan-Type Rapid Maxillary Expansion Vs Traditional Rapid Maxillary Expansion in Early Mixed Dentition A Prospective Clinical TrialMirza GlusacNo ratings yet
- Cantarella2018 DisyunciónDocument9 pagesCantarella2018 DisyunciónFernando Ruiz BorsiniNo ratings yet
- Embrasure and Central PappilaDocument5 pagesEmbrasure and Central PappilaDr. DeeptiNo ratings yet
- DiPietro 1976 Significance of FMA To ProsDocument12 pagesDiPietro 1976 Significance of FMA To ProsomidNo ratings yet
- Three-Dimensional Evaluation of Dentofacial Transverse Widths in Adults With Different Sagittal Facial Patterns PDFDocument10 pagesThree-Dimensional Evaluation of Dentofacial Transverse Widths in Adults With Different Sagittal Facial Patterns PDFSoe San KyawNo ratings yet
- Craniofacial Morphology in Women With Class I Occlusion and Severe Maxillary Anterior CrowdingDocument10 pagesCraniofacial Morphology in Women With Class I Occlusion and Severe Maxillary Anterior CrowdingMonojit DuttaNo ratings yet
- Class III Malocclusion and Bilateral Cross-Bite in An Adult Patient Treated With Miniscrew-Assisted Rapid Palatal Expander and AlignersDocument16 pagesClass III Malocclusion and Bilateral Cross-Bite in An Adult Patient Treated With Miniscrew-Assisted Rapid Palatal Expander and AlignersMirza GlusacNo ratings yet
- Kjod 51 4 250Document10 pagesKjod 51 4 250utokaNo ratings yet
- Oral CencerDocument14 pagesOral CencerVilaseca224466No ratings yet
- 3 PBDocument8 pages3 PBfabian hernandez medinaNo ratings yet
- A R A A C L S B C I C B G: Lveolar Idge Ugmentation: Omparative Ongitudinal Tudy Etween Alvaria and Liac Rest ONE RaftsDocument7 pagesA R A A C L S B C I C B G: Lveolar Idge Ugmentation: Omparative Ongitudinal Tudy Etween Alvaria and Liac Rest ONE RaftsDr. Jalisson VicenteNo ratings yet
- Artigo Bad SplitDocument6 pagesArtigo Bad SplitCarolinaNo ratings yet
- Alveolar and Skeletal Dimensions AssociatedDocument10 pagesAlveolar and Skeletal Dimensions AssociatedSankhyaNo ratings yet
- Laterodesviacion PDFDocument6 pagesLaterodesviacion PDFSantos TicaNo ratings yet
- Rozzi 2018Document8 pagesRozzi 2018Soe San KyawNo ratings yet
- Tomographic Evaluation of Infrazygomatic Crest ForDocument7 pagesTomographic Evaluation of Infrazygomatic Crest ForVishal SharmaNo ratings yet
- Maxillary Buccal Cortical Plate InclinationDocument6 pagesMaxillary Buccal Cortical Plate InclinationDa Hae SungNo ratings yet
- Dr. Uzair Synopsis (Latest)Document14 pagesDr. Uzair Synopsis (Latest)Muhammad UzairNo ratings yet
- S0889540620306843 PDFDocument10 pagesS0889540620306843 PDFPepe RiveraNo ratings yet
- Fuhrmann 2002Document6 pagesFuhrmann 2002DentalErNo ratings yet
- Lai 2012Document10 pagesLai 2012ARMADNo ratings yet
- 10 1016@j Ajodo 2018 10 018Document10 pages10 1016@j Ajodo 2018 10 018Maria Alejandra ForeroNo ratings yet
- Maxillary Buccal Cortical Plate Inclination at Miniscrew Insertion SitesDocument6 pagesMaxillary Buccal Cortical Plate Inclination at Miniscrew Insertion SitesBraulio CaroNo ratings yet
- 1 s2.0 S0889540622006552 MainDocument13 pages1 s2.0 S0889540622006552 MainMarcos Gómez SosaNo ratings yet
- Anatomic Study of Pterygomaxillary Junctions in KoreansDocument8 pagesAnatomic Study of Pterygomaxillary Junctions in KoreansDONGXU LIUNo ratings yet
- 1. 1-s2.0-S0278239119305518-mainDocument15 pages1. 1-s2.0-S0278239119305518-mainALEJANDRA INÉS NIETO ARIASNo ratings yet
- Width of Buccal and Posterior CorridorsDocument7 pagesWidth of Buccal and Posterior CorridorspapasNo ratings yet
- Carlino 2019Document9 pagesCarlino 2019Isabella WilkeNo ratings yet
- A Cone-Beam Computed Tomographic Study of Alveolar Bone Morphology in Patients With Unilateral Cleft Lip and PalateDocument9 pagesA Cone-Beam Computed Tomographic Study of Alveolar Bone Morphology in Patients With Unilateral Cleft Lip and PalateDiego Andres Hincapie HerreraNo ratings yet
- Skeletally-Anchored Maxillary Expansion: Promising Effects and LimitationsDocument23 pagesSkeletally-Anchored Maxillary Expansion: Promising Effects and LimitationsAya ElsayedNo ratings yet
- Abordaje Cigomato TransmandibularDocument14 pagesAbordaje Cigomato TransmandibularRafael LópezNo ratings yet
- Herbst Vs SGTBDocument8 pagesHerbst Vs SGTBdessy SijabatNo ratings yet
- Garrett 2008Document11 pagesGarrett 2008Swadhinata HNo ratings yet
- ENG1 Effect of Different Clasps On Asymmetric Distal Extension Base Supporting Structures 1Document12 pagesENG1 Effect of Different Clasps On Asymmetric Distal Extension Base Supporting Structures 1Madalina BanarescuNo ratings yet
- Safe Zone AjoDocument7 pagesSafe Zone AjojoeNo ratings yet
- Transverse Maxillary Deficiency GuideDocument26 pagesTransverse Maxillary Deficiency GuideminalNo ratings yet
- Incisive Canal and Its Propinquity To Maxillary Central Incisors in Various Sagittal Growth Patterns: A CBCT StudyDocument11 pagesIncisive Canal and Its Propinquity To Maxillary Central Incisors in Various Sagittal Growth Patterns: A CBCT StudyIJAR JOURNALNo ratings yet
- Art - Ref 2020Document10 pagesArt - Ref 2020Flor GutiérrezNo ratings yet
- JCDP 19 515Document6 pagesJCDP 19 515jaslinshalinNo ratings yet
- The Roof of The Labyrinthine Facial Nerve Canal and The Geniculate Ganglion Fossa On High-Resolution Computed Tomography - Dehiscence Thickness and PneumatizationDocument11 pagesThe Roof of The Labyrinthine Facial Nerve Canal and The Geniculate Ganglion Fossa On High-Resolution Computed Tomography - Dehiscence Thickness and PneumatizationSa'Deu FondjoNo ratings yet
- UntitledDocument6 pagesUntitledsanaNo ratings yet
- International Journal of Surgery Case Reports: Kanistika Jha, Manoj AdhikariDocument4 pagesInternational Journal of Surgery Case Reports: Kanistika Jha, Manoj AdhikariYeraldin EspañaNo ratings yet
- 13 de Praeter J, Dermaut L, Martens G, Et Al - Long-Term Stability of The Leveling of The Curve of SpeeDocument7 pages13 de Praeter J, Dermaut L, Martens G, Et Al - Long-Term Stability of The Leveling of The Curve of SpeeabhishekiNo ratings yet
- 2020 Article 73180Document11 pages2020 Article 73180rachmadyNo ratings yet
- Abeleira 2014Document11 pagesAbeleira 2014Luly AnggrainiNo ratings yet
- Imaging in Oral Cancers: Ead and Eck YmposiumDocument14 pagesImaging in Oral Cancers: Ead and Eck YmposiumHayyu F RachmadhanNo ratings yet
- 2021 Does The Timing of 1-Stage Palatoplasty With Radical Muscle Dissection Effect Long-Term Midface Growth A Single-Center Retrospective AnalysisDocument7 pages2021 Does The Timing of 1-Stage Palatoplasty With Radical Muscle Dissection Effect Long-Term Midface Growth A Single-Center Retrospective AnalysisDimitris RodriguezNo ratings yet
- Timmerman Et Al-2006-Journal of Clinical PeriodontologyDocument6 pagesTimmerman Et Al-2006-Journal of Clinical PeriodontologydrjonduNo ratings yet
- Dental Arch Widths and Mandibular Base Width in Class III MalocclusionsDocument6 pagesDental Arch Widths and Mandibular Base Width in Class III MalocclusionsShiva PrasadNo ratings yet
- Posterior Crossbite With Mandibular Asymmetry Treated With Lingual Appliances, Maxillary Skeletal Expanders, and Alveolar Bone MiniscrewsDocument21 pagesPosterior Crossbite With Mandibular Asymmetry Treated With Lingual Appliances, Maxillary Skeletal Expanders, and Alveolar Bone MiniscrewsJuliana ÁlvarezNo ratings yet
- Industrial Coupling and HoseDocument57 pagesIndustrial Coupling and HoseCesar CoronelNo ratings yet
- Energy Security IndexDocument13 pagesEnergy Security IndexCarlos AlvarezNo ratings yet
- Brand Project-Swapnil WaichaleDocument31 pagesBrand Project-Swapnil WaichaleSwapnil WaichaleNo ratings yet
- The Wall Street Journal - 24-11-2021Document30 pagesThe Wall Street Journal - 24-11-2021Samuel GiovanelliNo ratings yet
- Pokemon Heart GoldDocument8 pagesPokemon Heart GoldPainToTheWorldNo ratings yet
- Biotech ProjectDocument14 pagesBiotech ProjectRahul V ChandramouliNo ratings yet
- Poem PDFDocument6 pagesPoem PDFTaylor JohnsNo ratings yet
- 6-1 Homework Team 7Document3 pages6-1 Homework Team 7Edgar ValenciaNo ratings yet
- Power Gating - Power Management Technique: VLSI Basics and Interview QuestionsDocument12 pagesPower Gating - Power Management Technique: VLSI Basics and Interview QuestionsRohith RajNo ratings yet
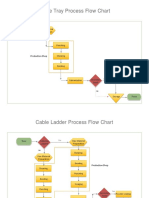
- Process Flow ChartDocument4 pagesProcess Flow Chartchacko chiramalNo ratings yet
- TextDocument17 pagesTextnaser zoabiNo ratings yet
- Swiss ReDocument9 pagesSwiss ReTuxedo1982No ratings yet
- HazCom QuizDocument8 pagesHazCom QuizMax McguireNo ratings yet
- 3d Printing Thesis StatementDocument5 pages3d Printing Thesis Statementoabfziiig100% (2)
- Mineral Resources: Earth ScienceDocument20 pagesMineral Resources: Earth ScienceRegina Mae Narciso NazarenoNo ratings yet
- A 3-Channel Monopulse Tracking Receiver System Using Commercial Off-The-Shelf EquipmentDocument9 pagesA 3-Channel Monopulse Tracking Receiver System Using Commercial Off-The-Shelf EquipmentJean-Hubert DelassaleNo ratings yet
- RTC Invoice 2965 Gj29es2223100505Document1 pageRTC Invoice 2965 Gj29es2223100505Alok PandeyNo ratings yet
- Bittersweet Tragedy - Melanie Martinez - LETRASDocument2 pagesBittersweet Tragedy - Melanie Martinez - LETRASFlávia FernandesNo ratings yet
- HTTP Sleekfreak Ath CX 81 3wdev CD3WD METALWRK GTZ075CE B65 7 HTMDocument14 pagesHTTP Sleekfreak Ath CX 81 3wdev CD3WD METALWRK GTZ075CE B65 7 HTMPavan SripadaNo ratings yet
- Sanitas-Health Coach Quick Start GuideDocument26 pagesSanitas-Health Coach Quick Start GuideGabriel MuresanuNo ratings yet
- Guitar SetupDocument1 pageGuitar SetupEduardo Maia CardosoNo ratings yet
- Lam Sendz MmsDocument8 pagesLam Sendz MmsVíc AltamarNo ratings yet
- Lesson 8 Homework Practice Volume and Surface Area of Composite Figures AnswersDocument8 pagesLesson 8 Homework Practice Volume and Surface Area of Composite Figures Answerscfg1ngzn100% (1)
- Capitulo 9 Incropera 4 EdDocument16 pagesCapitulo 9 Incropera 4 EdDaxon RodriguezNo ratings yet
- LP Series: Airless Paint SprayerDocument31 pagesLP Series: Airless Paint SprayerFrancisco Jose Domenech SalaNo ratings yet
- BD-90 75 Dekanter DE-EN 905-738-1 02-16Document4 pagesBD-90 75 Dekanter DE-EN 905-738-1 02-16RasoolKhadibiNo ratings yet
- SHS 2023 Thinking Skills Practice Test QuestionsDocument32 pagesSHS 2023 Thinking Skills Practice Test Questionsvenkatesh113No ratings yet
- Humidity Chamber Tek For Fruiting BRF Cakes - Mushroom Cultivation - Shroomery Message BoardDocument15 pagesHumidity Chamber Tek For Fruiting BRF Cakes - Mushroom Cultivation - Shroomery Message BoardABIYA UNIVERSENo ratings yet
- La Villa Fact Sheet 2021-2022-UpdatedDocument4 pagesLa Villa Fact Sheet 2021-2022-Updatedsweta suresh ganvirNo ratings yet
- Area and Circumference of CircleDocument17 pagesArea and Circumference of CircleJared VallesNo ratings yet