You might also like
- MedicineDocument206 pagesMedicinenandaram2191No ratings yet
- Cardio-Vascular ExaminationDocument43 pagesCardio-Vascular ExaminationDimas FrasesaNo ratings yet
- CardioDocument8 pagesCardioThomas KearneyNo ratings yet
- Approach To Diagnosis of Congenital Heart DiseasesDocument85 pagesApproach To Diagnosis of Congenital Heart DiseasesNirav CHOVATIYANo ratings yet
- Ventricel Septal DefectDocument38 pagesVentricel Septal DefectzaipullahNo ratings yet
- Ventricular Septal Defect: Present by Nur Kurnia Putri Halim Supervisor Dr. Akhtar Fajar M, SPJP, FihaDocument31 pagesVentricular Septal Defect: Present by Nur Kurnia Putri Halim Supervisor Dr. Akhtar Fajar M, SPJP, FihaChintya Fidelia MontangNo ratings yet
- Physiology Cardiodynamics and Shock: Bill Cayley MD Mdiv University of WisconsinDocument34 pagesPhysiology Cardiodynamics and Shock: Bill Cayley MD Mdiv University of WisconsinIamTineshNo ratings yet
- Vitals: Department of Paediatrics Nepalese Army Institute of Health SciencesDocument20 pagesVitals: Department of Paediatrics Nepalese Army Institute of Health SciencesDrakensberg EspaNo ratings yet
- Approach To Patients With Possible Cardiovascular Disease and Physical Examination of The Cardiovascular SystemDocument79 pagesApproach To Patients With Possible Cardiovascular Disease and Physical Examination of The Cardiovascular SystemLajel S. LachicaNo ratings yet
- New HematologyOncology FAE2016Document108 pagesNew HematologyOncology FAE2016omarNo ratings yet
- Sinus Rhythm and Sinus and Atrial DysrhythmiasDocument41 pagesSinus Rhythm and Sinus and Atrial Dysrhythmiasclaudia brongNo ratings yet
- Cardio PEDocument41 pagesCardio PENinna Isabel VictorioNo ratings yet
- Primary Care Arrhythmia FinalDocument36 pagesPrimary Care Arrhythmia FinalIsmai Eko SaputraNo ratings yet
- A1 CardioDocument98 pagesA1 CardioTikboy TaliliNo ratings yet
- EmergencyDocument47 pagesEmergencymedstudy123No ratings yet
- CVS ExaminationDocument85 pagesCVS ExaminationPrasenjit DasNo ratings yet
- CVS Examination-1Document84 pagesCVS Examination-1Prasenjit DasNo ratings yet
- Hypertension: Fadillah MaricarDocument30 pagesHypertension: Fadillah MaricarLucky CloverNo ratings yet
- Pericardial Diseases - Raghad DghaishDocument32 pagesPericardial Diseases - Raghad Dghaish180045No ratings yet
- PULSEDocument84 pagesPULSEVivek JaganathanNo ratings yet
- Congenital Heart Disease UHNDocument46 pagesCongenital Heart Disease UHNFaisalNo ratings yet
- Arterial PulseDocument37 pagesArterial PulseAdwaitha KrNo ratings yet
- Congestive Heart Failure (CHF) NYHA III E.C Coronary Artery Disease (OMI Anteroseptal)Document35 pagesCongestive Heart Failure (CHF) NYHA III E.C Coronary Artery Disease (OMI Anteroseptal)GP HMHNo ratings yet
- Approach To ECG PresentationDocument13 pagesApproach To ECG Presentationfck4wtgpckNo ratings yet
- Mitral RegurgitationDocument43 pagesMitral Regurgitationraissasafitry100% (1)
- Pericardial DiseaseDocument70 pagesPericardial DiseaseCindyNo ratings yet
- Valvular Heart DiseaseDocument55 pagesValvular Heart Diseaseapi-19916399No ratings yet
- Pediatric Cardiovascular Physical ExaminationDocument28 pagesPediatric Cardiovascular Physical ExaminationChakkrawan PhetfuangfaNo ratings yet
- Cardiac ArrythmiasDocument63 pagesCardiac ArrythmiasSankara SubramanianNo ratings yet
- Basic Arrythmia AnalysisDocument60 pagesBasic Arrythmia AnalysisZakky KurniawanNo ratings yet
- Aortic Regurgitation CaseDocument38 pagesAortic Regurgitation CaseIka MagfirahNo ratings yet
- 28,29 Management of Cardiac ArrhythmiasDocument41 pages28,29 Management of Cardiac ArrhythmiasSL Dr ChEMiSNo ratings yet
- Terapi Cairan PD Syok KardiogenikDocument27 pagesTerapi Cairan PD Syok KardiogenikSri AsmawatiNo ratings yet
- PULSE For Student.189736.1566462511.6189Document48 pagesPULSE For Student.189736.1566462511.6189Nuthahai SimangernNo ratings yet
- Pharmacology: Cardiovascular SystemDocument314 pagesPharmacology: Cardiovascular SystemSharifa DarayanNo ratings yet
- 41 Paediatric ArrhythmiasDocument4 pages41 Paediatric ArrhythmiasnasibdinNo ratings yet
- Robbi Zidnii Ilmaa, War Zuqnii Fahmaa, AamiinDocument109 pagesRobbi Zidnii Ilmaa, War Zuqnii Fahmaa, Aamiinfitrian amwaalunNo ratings yet
- 12 CS Supraventricular TachycardiaDocument64 pages12 CS Supraventricular TachycardiaFatima MaazNo ratings yet
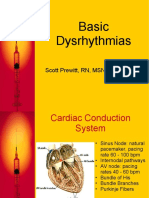
- Basic Dysrhythmias: Scott Prewitt, RN, MSN, APRN-BCDocument42 pagesBasic Dysrhythmias: Scott Prewitt, RN, MSN, APRN-BCtuffie85No ratings yet
- Chapter - 036 Arrhythmias ClassDocument129 pagesChapter - 036 Arrhythmias ClassWisdomIsMiseryNo ratings yet
- PCOL2Document21 pagesPCOL2CLARISSA GRACE GERALDINONo ratings yet
- Valvular UpdateDocument44 pagesValvular UpdateUlmi FadillahNo ratings yet
- Diagnosis Dan Tatalaksana Awal SVTDocument47 pagesDiagnosis Dan Tatalaksana Awal SVTZuly Vita AulyaNo ratings yet
- IC1 - Arrhythmia - 2012 EDITEDDocument42 pagesIC1 - Arrhythmia - 2012 EDITEDrazorazNo ratings yet
- Advanced Life SupportDocument65 pagesAdvanced Life SupportHandrian RahmanNo ratings yet
- Supraventricular Tachycardia NotesDocument59 pagesSupraventricular Tachycardia NotesShadi TabbarahNo ratings yet
- JVP Physical Exam PDFDocument2 pagesJVP Physical Exam PDFSuhana ShresthaNo ratings yet
- Eme CVDocument35 pagesEme CVJason LinNo ratings yet
- A Patient With PalpitationDocument43 pagesA Patient With PalpitationChris Jardine LiNo ratings yet
- KP 2.5.5.4 112027 - Shock FKGDocument39 pagesKP 2.5.5.4 112027 - Shock FKGnurul ramadhiniNo ratings yet
- How To Approach Dyspnea in ED - Pramono SigitDocument29 pagesHow To Approach Dyspnea in ED - Pramono SigitLeonita DwiNo ratings yet
- Dr. Niranjan Murthy HL Associate Professor Dept of Physiology SSMC, TumkurDocument53 pagesDr. Niranjan Murthy HL Associate Professor Dept of Physiology SSMC, TumkurnirilibNo ratings yet
- Cardiogenic Shock: BY Dr. M L Patel MD Associate Professor Deptt. of MedicineDocument19 pagesCardiogenic Shock: BY Dr. M L Patel MD Associate Professor Deptt. of MedicineDurgesh PushkarNo ratings yet
- Book Reading-Heart Disease Braunwald: Chapter 4 Physical Examination of The Heart and Circulation (I)Document29 pagesBook Reading-Heart Disease Braunwald: Chapter 4 Physical Examination of The Heart and Circulation (I)Jerrod WilsonNo ratings yet
- Approach To ACLS RhythmDocument150 pagesApproach To ACLS RhythmChristine Bernadette Rapal Bollong100% (2)
- Cyanotic Heart DiseaseDocument47 pagesCyanotic Heart Disease87-Saranya MNo ratings yet
- Arrhythmia 6 YrDocument72 pagesArrhythmia 6 YrPiyush MalikNo ratings yet
- Cardiovascular System ExaminationDocument67 pagesCardiovascular System ExaminationJaaydev100% (1)
- Valvular Heart Disease. KulDocument60 pagesValvular Heart Disease. KulIntan Kumalasari RambeNo ratings yet
- Immediate Life Support for healthcare Practitioners: A Step-By-Step GuideFrom EverandImmediate Life Support for healthcare Practitioners: A Step-By-Step GuideNo ratings yet
- Activty CHNDocument9 pagesActivty CHNGeneter EspirituNo ratings yet
- (Magness, Steve) Training NotesDocument28 pages(Magness, Steve) Training NotesDanCurtis100% (3)
- Diagnostic Procedures in Respiratory DiseaseDocument41 pagesDiagnostic Procedures in Respiratory DiseaseVio Mincu100% (1)
- Practical 20epidemiology 20 20for 20students 20and 20residentsDocument143 pagesPractical 20epidemiology 20 20for 20students 20and 20residentsIonutStanciuNo ratings yet
- Developing Management Skills: Managing Personal StressDocument33 pagesDeveloping Management Skills: Managing Personal StressThuyDuongNo ratings yet
- VitaminsDocument94 pagesVitaminsAnonymous iG0DCOfNo ratings yet
- Encefalitis LimbicaDocument11 pagesEncefalitis LimbicaRandy UlloaNo ratings yet
- Bezold AbscessDocument2 pagesBezold AbscessSamuel anNo ratings yet
- And Treatment Blepharokeratoconjunctivitis in Children: DiagnosisDocument5 pagesAnd Treatment Blepharokeratoconjunctivitis in Children: DiagnosislordaponkNo ratings yet
- CPH Chapter 1 2Document3 pagesCPH Chapter 1 2Mica CapistranoNo ratings yet
- Sports PhysiologyDocument3 pagesSports PhysiologyCLEMENTNo ratings yet
- 741 PUB Working Paper 35 PDFDocument34 pages741 PUB Working Paper 35 PDFBushra AsifNo ratings yet
- Alpha Shipping ManagementDocument2 pagesAlpha Shipping ManagementAlexylle Garsula de ConcepcionNo ratings yet
- AKP Jan. 2022Document30 pagesAKP Jan. 2022jcNo ratings yet
- Reduced Cortical Folding in PPPDDocument12 pagesReduced Cortical Folding in PPPDDanielNo ratings yet
- COMLEX Level 3 Time Grid and Self AssessmentDocument19 pagesCOMLEX Level 3 Time Grid and Self AssessmentR KidderNo ratings yet
- Cabaluna, Krizzia Franz L. BSN 1A: Biographical DataDocument7 pagesCabaluna, Krizzia Franz L. BSN 1A: Biographical DataNeølie Abello LatúrnasNo ratings yet
- Physiological Effects of Valsalva and IppvDocument27 pagesPhysiological Effects of Valsalva and IppvChaturika Bandara100% (1)
- Itch in Elderly People: A Cross-Sectional Study: Investigative ReportDocument9 pagesItch in Elderly People: A Cross-Sectional Study: Investigative ReportPatricia JesikaNo ratings yet
- Cerebral Palsy: by Ali Mohammad PhysiotherapistDocument16 pagesCerebral Palsy: by Ali Mohammad Physiotherapistwaris aliNo ratings yet
- Sept 17 Papers by DR - DR Raja WaseemDocument100 pagesSept 17 Papers by DR - DR Raja WaseemdrusmansaleemNo ratings yet
- FMGE December 4th 2020Document75 pagesFMGE December 4th 2020shimailNo ratings yet
- 04 - Typhoid FeverDocument35 pages04 - Typhoid Feversoheil100% (1)
- Occupational Health Surveillance by Fiona DavidsonDocument33 pagesOccupational Health Surveillance by Fiona DavidsonMuhammad Teguh DPNo ratings yet
- Emedicine Hypersemesis GravidarumDocument26 pagesEmedicine Hypersemesis GravidarumAnonymous 3OoumAUytNo ratings yet
- PADocument8 pagesPAtriziasisonNo ratings yet
- JIO Sailent FeaturesDocument3 pagesJIO Sailent FeaturesReeta DuttaNo ratings yet
- Jeopardy Digestive and Urinary SystemsDocument27 pagesJeopardy Digestive and Urinary Systemsapi-133770097No ratings yet
- CHN TransesDocument82 pagesCHN Transeskint manlangitNo ratings yet
- Endocrine System: Dr. Dedi Ardinata, M.Kes Physiology Department Medical School of University Sumatera UtaraDocument94 pagesEndocrine System: Dr. Dedi Ardinata, M.Kes Physiology Department Medical School of University Sumatera UtaraAdryansyah ChaniagoNo ratings yet