You might also like
- Psychotherapy DAP NoteDocument2 pagesPsychotherapy DAP NoteMistor Williams100% (1)
- Water Cures - F. Batmanghelidj, M.DDocument22 pagesWater Cures - F. Batmanghelidj, M.DEric Callahan100% (1)
- Intestinal ObstructionDocument59 pagesIntestinal ObstructionGeorge GuruNo ratings yet
- History and Physical Exam For COPDDocument2 pagesHistory and Physical Exam For COPDKarenJulioNo ratings yet
- Scoliosis PDFDocument19 pagesScoliosis PDFdallas100% (1)
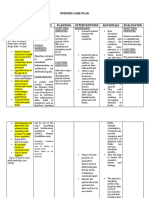
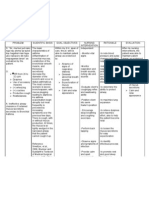
- Nursing Care Plan Diarrhea Assessment Diagnosis Planning Interventions Rationale EvaluationDocument8 pagesNursing Care Plan Diarrhea Assessment Diagnosis Planning Interventions Rationale EvaluationKrahNo ratings yet
- Laser Therapy ProtocolsDocument89 pagesLaser Therapy ProtocolsSYED ALI HUSSAINNo ratings yet
- SERETIDEDocument3 pagesSERETIDETempoNo ratings yet
- CyanosisDocument11 pagesCyanosissr_sushil100% (1)
- Pone 0267186Document18 pagesPone 0267186Kimberly Claire ParageleNo ratings yet
- 1 s2.0 S1201971219304229 MainDocument10 pages1 s2.0 S1201971219304229 MainAlleidya SalsabiillaNo ratings yet
- Journal Feng LiaoDocument19 pagesJournal Feng LiaoDewi KUNo ratings yet
- Asymptomatic and Human To Human Transmission of SARS COV 2Document3 pagesAsymptomatic and Human To Human Transmission of SARS COV 2belinda thaniaNo ratings yet
- Kegawatdaruratan Emergency DBD AnakDocument2 pagesKegawatdaruratan Emergency DBD AnakTheresia ChesarNo ratings yet
- Risk Predictors of Progression To Severe Disease of DengueDocument13 pagesRisk Predictors of Progression To Severe Disease of DengueTaufiqurrokhman RofiiNo ratings yet
- Toxoplasma Gondii Infection in Immunocompromised PatientsDocument12 pagesToxoplasma Gondii Infection in Immunocompromised PatientsHarvey alvin HartonoNo ratings yet
- Prevalence of Dengue Among Clinically SuDocument5 pagesPrevalence of Dengue Among Clinically SuIshreet ChaddaNo ratings yet
- A Two-Year Review On Epidemiology and Clinical Characteristics of Dengue Deaths in Malaysia, 2013-2014Document16 pagesA Two-Year Review On Epidemiology and Clinical Characteristics of Dengue Deaths in Malaysia, 2013-2014ibnu malikNo ratings yet
- PIIS1473309920302875Document9 pagesPIIS1473309920302875perozcyrusNo ratings yet
- Journal Pone 0190637Document15 pagesJournal Pone 0190637cooky maknaeNo ratings yet
- Pone 0217474Document12 pagesPone 0217474Breixo HarguindeyNo ratings yet
- HHS Public Access: The Global Distribution and Burden of DengueDocument13 pagesHHS Public Access: The Global Distribution and Burden of Denguelukman fatkhulNo ratings yet
- Fcimb 11 694093Document12 pagesFcimb 11 694093Marketable StudioNo ratings yet
- Review of Literature On Dengue Fever in IndiaDocument9 pagesReview of Literature On Dengue Fever in Indial1wot1j1fon3100% (1)
- Another Dengue Fever Outbreak in Eastern Ethiopia-An Emerging Public Health ThreatDocument16 pagesAnother Dengue Fever Outbreak in Eastern Ethiopia-An Emerging Public Health ThreatNigatu AdmasuNo ratings yet
- Etiologic and Epidemiologic Analysis of Hand FootDocument9 pagesEtiologic and Epidemiologic Analysis of Hand FootAisah AisahNo ratings yet
- 2 A Population Based Cohort Study On Chronic Comorbidity Risk Factors For Adverse Outcome in DengueDocument8 pages2 A Population Based Cohort Study On Chronic Comorbidity Risk Factors For Adverse Outcome in Denguerommelbasket08No ratings yet
- Antonio Jose GrandeDocument23 pagesAntonio Jose Grandeagung dwi darmawanNo ratings yet
- Dengue (Lancet)Document16 pagesDengue (Lancet)Roberth Mero100% (1)
- A Systematic Review and Meta-Analysis of Dengue Risk With Temperature ChangeDocument16 pagesA Systematic Review and Meta-Analysis of Dengue Risk With Temperature ChangedianNo ratings yet
- Diabetes With Hypertension As Risk Factors For Adult Dengue Hemorrhagic Fever in A Predominantly Dengue Serotype 2 Epidemic: A Case Control StudyDocument12 pagesDiabetes With Hypertension As Risk Factors For Adult Dengue Hemorrhagic Fever in A Predominantly Dengue Serotype 2 Epidemic: A Case Control StudyDwitari Novalia HaraziNo ratings yet
- Awareness of Dengue and Practice of Dengue Control Among1Document6 pagesAwareness of Dengue and Practice of Dengue Control Among1rjohn 7No ratings yet
- Paper FataldengueDocument19 pagesPaper FataldengueaidsariveraNo ratings yet
- Sars 2017Document10 pagesSars 2017LENA ELINNA OLIN BINTI AMBROSENo ratings yet
- PIIS1473309920302735Document7 pagesPIIS1473309920302735mostafa shahrabiNo ratings yet
- 21, Malaria Vs Dengue 2020Document4 pages21, Malaria Vs Dengue 2020Raquel FernandezNo ratings yet
- Pattern and Outcome of Dengue Fever in ADocument6 pagesPattern and Outcome of Dengue Fever in ABambang SudjatmikoNo ratings yet
- Risk Factors For Extrapulmonary Dissemination of Tuberculosis and Associated Mortality During Treatment For Extrapulmonary TuberculosisDocument15 pagesRisk Factors For Extrapulmonary Dissemination of Tuberculosis and Associated Mortality During Treatment For Extrapulmonary TuberculosisVincentius Michael WilliantoNo ratings yet
- New Insights of Emerging Sars-Cov-2: Epidemiology, Etiology, Clinical Features, Clinical Treatment, and PreventionDocument22 pagesNew Insights of Emerging Sars-Cov-2: Epidemiology, Etiology, Clinical Features, Clinical Treatment, and PreventionWendi IochNo ratings yet
- Animals Causing Infectious Disease - A Brief Review Vijayasankari A, Kalpana SDocument4 pagesAnimals Causing Infectious Disease - A Brief Review Vijayasankari A, Kalpana Snithish krishnaNo ratings yet
- Alyzah ArticleDocument9 pagesAlyzah ArticledanrevguevarraNo ratings yet
- Dengue LancetDocument16 pagesDengue LancetJorge Ricardo Uchuya GómezNo ratings yet
- Liu2020 Article ClinicalAndBiochemicalIndexesFDocument11 pagesLiu2020 Article ClinicalAndBiochemicalIndexesFGabriel Ibarra TrujilloNo ratings yet
- AsdsfDocument6 pagesAsdsfvirta andhikaNo ratings yet
- Epidemiological Risk Factors For Adult Dengue in Singapore: An 8-Year Nested Test Negative Case Control StudyDocument9 pagesEpidemiological Risk Factors For Adult Dengue in Singapore: An 8-Year Nested Test Negative Case Control StudydouwesdNo ratings yet
- 2018 Monitoring and Detection of Leprosy Patients in Southest China A Retrospective Study 2010 - 2014Document8 pages2018 Monitoring and Detection of Leprosy Patients in Southest China A Retrospective Study 2010 - 2014Jorge RicardoNo ratings yet
- Dengue Hemorrhagic Fever and Shock Syndromes : Suchitra Ranjit, MBBS, MD Niranjan Kissoon, MBBS, FAAP, FCCM, FACPEDocument11 pagesDengue Hemorrhagic Fever and Shock Syndromes : Suchitra Ranjit, MBBS, MD Niranjan Kissoon, MBBS, FAAP, FCCM, FACPEvalenzuelacastilloNo ratings yet
- Seminar: Annelies Wilder-Smith, Eng-Eong Ooi, Olaf Horstick, Bridget WillsDocument14 pagesSeminar: Annelies Wilder-Smith, Eng-Eong Ooi, Olaf Horstick, Bridget WillsAlexander ArguelloNo ratings yet
- Liu Et Al-2021-Frontiers in Cellular and Infection MicrobiologyDocument11 pagesLiu Et Al-2021-Frontiers in Cellular and Infection MicrobiologyGTA5ON360No ratings yet
- Nguyen Minh Tuan 2013Document8 pagesNguyen Minh Tuan 2013libremdNo ratings yet
- Article+0201 129 136Document8 pagesArticle+0201 129 136Rizeillah QaanitahNo ratings yet
- Journal BinghuaDocument12 pagesJournal BinghuaDewi KUNo ratings yet
- H5N1Document7 pagesH5N1miqbal_100No ratings yet
- 2021 - Factors Affecting Outcome of Longer Regimen Multidrug-Resistant Tuberculosis Treatment in West Java Indonesia A Retrospective Cohort StudyDocument13 pages2021 - Factors Affecting Outcome of Longer Regimen Multidrug-Resistant Tuberculosis Treatment in West Java Indonesia A Retrospective Cohort StudyNurul RifqianiNo ratings yet
- 2Document9 pages2Dinda Dwi AgustinaNo ratings yet
- 838 3348 1 PBDocument7 pages838 3348 1 PBararapiaNo ratings yet
- Laboratory Diagnosis of Dengue Infection: Current Techniques and Future StrategiesDocument9 pagesLaboratory Diagnosis of Dengue Infection: Current Techniques and Future StrategiesAndri YansyahNo ratings yet
- K. Jagannath: Singh. Teacher Indus High School KurnoolDocument29 pagesK. Jagannath: Singh. Teacher Indus High School KurnoolJagannath SinghNo ratings yet
- WHO Dengue Bulletin Vol 24 Dec 2000Document3 pagesWHO Dengue Bulletin Vol 24 Dec 2000Tapojyoti DasNo ratings yet
- Dengvaxia VaccineDocument8 pagesDengvaxia VaccineBayek NgekekNo ratings yet
- Soil Transmitted Helminths Prevalence, Perception and Determinants Among Primary School Children in Rural Enugu State, NigeriaDocument12 pagesSoil Transmitted Helminths Prevalence, Perception and Determinants Among Primary School Children in Rural Enugu State, Nigeriaelias aniwadaNo ratings yet
- Ciaa242 2 PDFDocument8 pagesCiaa242 2 PDFHesbon MomanyiNo ratings yet
- Journal Pre-Proof: International Journal of Infectious DiseasesDocument14 pagesJournal Pre-Proof: International Journal of Infectious DiseasesKenya EspinozaNo ratings yet
- JurnalDocument18 pagesJurnalDefina RamandhaniNo ratings yet
- Epidemiology 2016Document65 pagesEpidemiology 2016musa onyango obuyaNo ratings yet
- Evolution of Drug-Resistant Acinetobacter Baumannii After DCD Renal TransplantationDocument9 pagesEvolution of Drug-Resistant Acinetobacter Baumannii After DCD Renal TransplantationsserggiosNo ratings yet
- Risk Factors For Herpes Zoster in Patients With Chronic Kidney Disease: A Case-Control StudyDocument7 pagesRisk Factors For Herpes Zoster in Patients With Chronic Kidney Disease: A Case-Control StudyPushpendra Singh ChouhanNo ratings yet
- Diagnostic Imaging of Novel Coronavirus PneumoniaFrom EverandDiagnostic Imaging of Novel Coronavirus PneumoniaMinming ZhangNo ratings yet
- Infectious Diseases in Solid-Organ Transplant Recipients: A practical approachFrom EverandInfectious Diseases in Solid-Organ Transplant Recipients: A practical approachOriol ManuelNo ratings yet
- Ineffective Airway ClearanceDocument1 pageIneffective Airway ClearancejomerdalonaNo ratings yet
- What Are Bacteria - Streptococcus FaecalisDocument3 pagesWhat Are Bacteria - Streptococcus FaecalisAnkan PalNo ratings yet
- The Anaesthetic Crisis Manual Is An Excellent Companion The Anaesthetic Crisis Manual Has All Drug Doses ConvenientlyDocument1 pageThe Anaesthetic Crisis Manual Is An Excellent Companion The Anaesthetic Crisis Manual Has All Drug Doses Convenientlyali etikarNo ratings yet
- Ulkus VarricosumDocument26 pagesUlkus VarricosumNurul FadilahNo ratings yet
- Summary of Blood Donor Deferral Following Covid 19 Vaccine and CCP TransfusionDocument1 pageSummary of Blood Donor Deferral Following Covid 19 Vaccine and CCP Transfusionalimas darNo ratings yet
- PSA Great HoaxDocument24 pagesPSA Great HoaxjobishNo ratings yet
- Spinal Cord InjuryDocument52 pagesSpinal Cord Injurynur muizzah afifah hussinNo ratings yet
- نشرة المختبرDocument85 pagesنشرة المختبرAhmed GaberNo ratings yet
- COVID19 Aanpak Van HVAC SystemenDocument4 pagesCOVID19 Aanpak Van HVAC SystemenJan Willem van BorselenNo ratings yet
- Determination of DeathDocument8 pagesDetermination of DeathZam PamateNo ratings yet
- Vernal Keratoconjunctivitis (VKC)Document19 pagesVernal Keratoconjunctivitis (VKC)api-3742497No ratings yet
- NR 325 Diabetes Power-Student Copy1118Document39 pagesNR 325 Diabetes Power-Student Copy1118John MixerNo ratings yet
- Renal or Urinary Tract DisorderDocument6 pagesRenal or Urinary Tract DisorderMarcel Quario OrinaNo ratings yet
- Presentation 1Document18 pagesPresentation 1Talha Mughal Talha MughalNo ratings yet
- Glycogen Storage Disease, Type II (Pompe Disease) : BackgroundDocument7 pagesGlycogen Storage Disease, Type II (Pompe Disease) : Background201111000No ratings yet
- Tutor: Dr. Vera Dr. Haerani: Skenario Problems Learning Objectives Main Map ReferensiDocument36 pagesTutor: Dr. Vera Dr. Haerani: Skenario Problems Learning Objectives Main Map ReferensiAdeLia Nur FitrianaNo ratings yet
- Evaluation and Treatment of Hypertensive Emergencies in AdultsDocument13 pagesEvaluation and Treatment of Hypertensive Emergencies in Adultsjavier ariasNo ratings yet
- Nosocomial InfectionDocument57 pagesNosocomial InfectionFaith Ho100% (1)
- Soft Tissue Disorders and Fibromyalgia: Jaya Ravindran Consultant RheumatologistDocument54 pagesSoft Tissue Disorders and Fibromyalgia: Jaya Ravindran Consultant RheumatologistarunupadhayaNo ratings yet
- Common Brain MalformationsDocument10 pagesCommon Brain MalformationsradiologyNo ratings yet
- Syllabus Pharmaceuticals Related Neurotoxicity C16 Kumar April 22 Sat 2023 AANDocument59 pagesSyllabus Pharmaceuticals Related Neurotoxicity C16 Kumar April 22 Sat 2023 AANJere AyerbeNo ratings yet