You might also like
- Patient Care Technician Textbook PDF ISBN 978-1495107993Document24 pagesPatient Care Technician Textbook PDF ISBN 978-1495107993McGill0% (8)
- ATI OB Study GuideDocument26 pagesATI OB Study GuideThelma Jerome100% (1)
- RH and Abo IncompatibilityDocument10 pagesRH and Abo IncompatibilityamitNo ratings yet
- DARSHANA Score Card PDFDocument2 pagesDARSHANA Score Card PDFHk Lifestyle100% (1)
- 30.99.00.8517-1 Rev. 0 (1) Criticality Rating SpecsDocument40 pages30.99.00.8517-1 Rev. 0 (1) Criticality Rating Specsvishnuvarthan50% (2)
- G JaundiceDocument40 pagesG JaundiceRedina Tuya RamirezNo ratings yet
- HEMATOLOGIC ONCOLOGIC IMMUNOLOGIC DISORDERS - BoardsDocument10 pagesHEMATOLOGIC ONCOLOGIC IMMUNOLOGIC DISORDERS - BoardsSoojung NamNo ratings yet
- Integrated MNH Card (Must Use) - 2022 85428 PDFDocument4 pagesIntegrated MNH Card (Must Use) - 2022 85428 PDFMichael MohammedNo ratings yet
- OB Careplan JaundiceDocument6 pagesOB Careplan JaundiceRenee' MayoNo ratings yet
- Hemolytic Disease of The New Born (HDN)Document24 pagesHemolytic Disease of The New Born (HDN)Miftah YasinNo ratings yet
- UK Biologics Checklist May 2014Document2 pagesUK Biologics Checklist May 2014Dr Sneha's Skin and Allergy Clinic IndiaNo ratings yet
- Neonatal Jaundice: Carolyn Joy Mendoza-Capisnon Geraldine Marie SalvoDocument46 pagesNeonatal Jaundice: Carolyn Joy Mendoza-Capisnon Geraldine Marie SalvoCarolyn CapisnonNo ratings yet
- Hemolytic Disease of The Fetus /newbornDocument46 pagesHemolytic Disease of The Fetus /newbornK.M.S. ChathunikaNo ratings yet
- Haemolytic Disease of The Newborn: Dr. Suhair Abbas Ahmed Dept of HaematologyDocument46 pagesHaemolytic Disease of The Newborn: Dr. Suhair Abbas Ahmed Dept of HaematologyChokJunHoongNo ratings yet
- Screening Tests For Anc MotherDocument20 pagesScreening Tests For Anc MotherDhrumini PatelNo ratings yet
- Transfusion ScienceDocument1 pageTransfusion ScienceMaahin IbrahimNo ratings yet
- 1.a Diagnostic Test in High Risk Pregnancy LecDocument12 pages1.a Diagnostic Test in High Risk Pregnancy LecFarmisa MannanNo ratings yet
- Presentation ABO & RH IncompactDocument33 pagesPresentation ABO & RH IncompactPinanong PimsuwanNo ratings yet
- Hayats ResponsesDocument18 pagesHayats Responsesyacineone01No ratings yet
- Hemolytic DiseaseDocument22 pagesHemolytic DiseaseDavid Young0% (1)
- Pedia: Hepatic Dysfunction: Fcnlxa - St. Luke's College of NursingDocument3 pagesPedia: Hepatic Dysfunction: Fcnlxa - St. Luke's College of NursingLAXA FRANCINENo ratings yet
- O&G History TakingDocument5 pagesO&G History TakingAishwarya SivakumarNo ratings yet
- Rhisoimmunization2 191008035506Document50 pagesRhisoimmunization2 191008035506vijetha gmcNo ratings yet
- RH Incompatibility Information - Mount Sinai - New YorkDocument3 pagesRH Incompatibility Information - Mount Sinai - New YorkLnkNo ratings yet
- Anti GDocument4 pagesAnti GDR.RAJESWARI SUBRAMANIYANNo ratings yet
- Neonatal JaundiveDocument15 pagesNeonatal JaundiveCarolyn CapisnonNo ratings yet
- RH Incompatibility: DR - Minal M. Patil Dr. Jyotsna P. PatilDocument27 pagesRH Incompatibility: DR - Minal M. Patil Dr. Jyotsna P. Patilchitushri100% (1)
- RH Incompatibility: Manuel V. Gallego Foundation Colleges Inc. Cabanatuan CityDocument4 pagesRH Incompatibility: Manuel V. Gallego Foundation Colleges Inc. Cabanatuan CityAnthea ValinoNo ratings yet
- Hemolytic Disease of NewbornDocument41 pagesHemolytic Disease of NewbornRaja100% (3)
- Antenatal Case - Jonathan Matthews - November 2013Document25 pagesAntenatal Case - Jonathan Matthews - November 2013Anusree AnusreervNo ratings yet
- Association of ABO and RH Incompatibility With NeonatalDocument8 pagesAssociation of ABO and RH Incompatibility With NeonatalMer RodriguezNo ratings yet
- Recall Questions-February 14, 2018 Wyne Brent M. Corpuz, RMTDocument4 pagesRecall Questions-February 14, 2018 Wyne Brent M. Corpuz, RMTRafael CayananNo ratings yet
- Neonatal Jaundice Disease Infographics by SlidesgoDocument42 pagesNeonatal Jaundice Disease Infographics by Slidesgoshahedshaderma15No ratings yet
- New Intern Guide Quick NotesDocument8 pagesNew Intern Guide Quick NotesTrisNo ratings yet
- University of Perpetual Help System - Isabela Campus Minante Uno, Cauayan City, IsabelaDocument12 pagesUniversity of Perpetual Help System - Isabela Campus Minante Uno, Cauayan City, Isabelaliam0831No ratings yet
- Hemolytic Disease of Newborn Class NotesDocument37 pagesHemolytic Disease of Newborn Class NotesElvisNo ratings yet
- Preterm LabourDocument3 pagesPreterm Labourcgao30No ratings yet
- Approach To Red Blood Cell Testing During PregnancyDocument14 pagesApproach To Red Blood Cell Testing During PregnancyPaulinaNo ratings yet
- Psychological Task of Pregnancy Danger Signs of Pregnancy: 4. Past Medical HistoryDocument6 pagesPsychological Task of Pregnancy Danger Signs of Pregnancy: 4. Past Medical HistoryKimberly Sharah Mae Fortuno100% (1)
- Management of Neonatal SepsisDocument30 pagesManagement of Neonatal SepsisRam krishnaNo ratings yet
- Approach To Neonatal JaundiceDocument73 pagesApproach To Neonatal JaundiceG Venkatesh50% (2)
- NCM 219 Review Part 1 and 2Document62 pagesNCM 219 Review Part 1 and 2jocieangelmendoza01No ratings yet
- Interpretation of THE Complete Blood Count: Paula KjöllerströmDocument32 pagesInterpretation of THE Complete Blood Count: Paula KjöllerströmAs Minhas OrigensNo ratings yet
- Management of Neonatal Sepsis: Niki Kosmetatos, MD Anthony Piazza, MD J. Devn Cornish, MDDocument30 pagesManagement of Neonatal Sepsis: Niki Kosmetatos, MD Anthony Piazza, MD J. Devn Cornish, MDiniidzniNo ratings yet
- Pediatric Transfusion-Risks and Guidelines - Cairo 9-01Document47 pagesPediatric Transfusion-Risks and Guidelines - Cairo 9-01Prateek GuptaNo ratings yet
- Brent Hospital and Colleges IncorporatedDocument2 pagesBrent Hospital and Colleges IncorporatedArnold Cavalida BucoyNo ratings yet
- Inkompatibilitas DarahDocument3 pagesInkompatibilitas DarahIntan PermataNo ratings yet
- Review For Pediajc OsoeDocument9 pagesReview For Pediajc OsoeAlloy Trixia BaguioNo ratings yet
- PBL 7Document8 pagesPBL 7Natosha MendozaNo ratings yet
- Hemolytic Disease of The NewbornDocument43 pagesHemolytic Disease of The Newbornalibayaty1No ratings yet
- Illustrator File Edit Select Effect View Window HelpDocument12 pagesIllustrator File Edit Select Effect View Window HelpHaizel BieberNo ratings yet
- 6TH - Rh-Sensi.-Pih-Eclampsia-HydramniousDocument32 pages6TH - Rh-Sensi.-Pih-Eclampsia-HydramnioussrslytrdNo ratings yet
- RH Incompatibility New For MDDocument65 pagesRH Incompatibility New For MDMd AtifNo ratings yet
- Algorithm 5: Coelomic Distention Coelomic DistentionDocument1 pageAlgorithm 5: Coelomic Distention Coelomic DistentionAli BakNo ratings yet
- Pediatrics - Neonatal Jaundice PDFDocument2 pagesPediatrics - Neonatal Jaundice PDFJasmine KangNo ratings yet
- Phototherapy 2Document8 pagesPhototherapy 2Dyah Putri PermatasariNo ratings yet
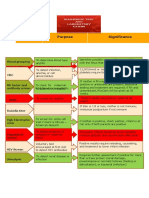
- Test Purpose Significance: HGB and HCT CBC Blood GroupingDocument1 pageTest Purpose Significance: HGB and HCT CBC Blood GroupingMarwina DorieNo ratings yet
- Gestation Purpose of VisitDocument1 pageGestation Purpose of Visitabu ubaidah100% (1)
- Blood Grouping in Pregnancy, Guidelines and Foetal GenotypingDocument37 pagesBlood Grouping in Pregnancy, Guidelines and Foetal GenotypingaliNo ratings yet
- Chapter 7 GUIDE To CSIDocument28 pagesChapter 7 GUIDE To CSIJade RomongNo ratings yet
- Introduction To Bayesian TheoryDocument2 pagesIntroduction To Bayesian TheorySumanthNo ratings yet
- Educational Moments: What You Need To KnowDocument3 pagesEducational Moments: What You Need To KnowWagner de AvizNo ratings yet
- The Temporal Experience of Pleasure Scale (TEPS) : Exploration and Confirmation of Factor Structure in A Healthy Chinese SampleDocument7 pagesThe Temporal Experience of Pleasure Scale (TEPS) : Exploration and Confirmation of Factor Structure in A Healthy Chinese SampleShellyNo ratings yet
- 4 16Document42 pages4 16seddeik14 seddeikNo ratings yet
- NbdeDocument4 pagesNbdeNancy NaeimNo ratings yet
- Covid-19 Test Report SampleDocument1 pageCovid-19 Test Report SampleAhsanul HaqueNo ratings yet
- State Bank of India: Roll Numbers of Candidates Selected Provisionally From Waiting ListDocument1 pageState Bank of India: Roll Numbers of Candidates Selected Provisionally From Waiting Listseema malikNo ratings yet
- Session 0 - Cervical Cancer Screening and Treatment - Course Overview-REVIEWEDDocument16 pagesSession 0 - Cervical Cancer Screening and Treatment - Course Overview-REVIEWEDFaraaz SokwalaNo ratings yet
- 3ixso2idq334tonwmfhk0rrcDocument2 pages3ixso2idq334tonwmfhk0rrcrishikeshraj2021No ratings yet
- Camila E Mulero Morales - GRED 603 - d2 Test of Attention in Professional Counseling Presentation (Recording)Document19 pagesCamila E Mulero Morales - GRED 603 - d2 Test of Attention in Professional Counseling Presentation (Recording)Kae Mulero MoralesNo ratings yet
- Comparison of Quantitative and Qualilative Research MethodsDocument68 pagesComparison of Quantitative and Qualilative Research MethodsWellings ChizumilaNo ratings yet
- Fmea Quiz TrainingDocument4 pagesFmea Quiz Trainingrajesh sharmaNo ratings yet
- OPTHA 1.2 BASIC EYE EXAM - Dr. CheongDocument4 pagesOPTHA 1.2 BASIC EYE EXAM - Dr. CheongPatricia ManaliliNo ratings yet
- Process Safety Management, Q & ADocument84 pagesProcess Safety Management, Q & AAhmed HamadNo ratings yet
- The Odds Ratio: Statistics NotesDocument1 pageThe Odds Ratio: Statistics NotesMarceNo ratings yet
- IFIA Petroleum Inspector Certification ProgrammeDocument6 pagesIFIA Petroleum Inspector Certification Programmeابوالحروف العربي ابوالحروفNo ratings yet
- Survey To Assess The Attitude of Nursing Students Regarding Prevention of COVID 19 During COVID19 PandemicDocument3 pagesSurvey To Assess The Attitude of Nursing Students Regarding Prevention of COVID 19 During COVID19 PandemicEditor IJTSRDNo ratings yet
- SK SHARMA Hall Ticket IgnouDocument2 pagesSK SHARMA Hall Ticket IgnouSonu SharmaNo ratings yet
- Special, Emergency, Electronic Cross MatchingDocument4 pagesSpecial, Emergency, Electronic Cross MatchingAkash SarkarNo ratings yet
- Ergonomics & Safety CoursDocument2 pagesErgonomics & Safety CoursEstifanos FitsumNo ratings yet
- Effects of Occupational Health and Safety Culture On Employees' Performance at Agility International LTD., Semarang BranchDocument16 pagesEffects of Occupational Health and Safety Culture On Employees' Performance at Agility International LTD., Semarang BranchAndi Indah MagefirahNo ratings yet
- Berita Acara 14-07-2022Document12 pagesBerita Acara 14-07-2022tiaraardinataNo ratings yet
- Measures of IntelligenceDocument28 pagesMeasures of IntelligenceAudrey ConnerNo ratings yet
- FSMRDocument1 pageFSMRJulie50% (2)
- Adequacy of Fusion of Extruded Poly (Vinyl Chloride) (PVC) Pipe and Molded Fittings by Acetone ImmersionDocument3 pagesAdequacy of Fusion of Extruded Poly (Vinyl Chloride) (PVC) Pipe and Molded Fittings by Acetone ImmersionAndres Camilo BenitezNo ratings yet
- The Clinical LaboratoryDocument24 pagesThe Clinical LaboratoryRomar DurianNo ratings yet