You might also like
- 16 Amniotic Fluid EmbolismDocument46 pages16 Amniotic Fluid EmbolismAhmed TarigNo ratings yet
- Management of Amniotic Fluid Embolism (AFEDocument30 pagesManagement of Amniotic Fluid Embolism (AFEMostafa EissaNo ratings yet
- Amniotic Fluid EmbolismDocument30 pagesAmniotic Fluid Embolismjhon heriansyah0% (1)
- Pleura Effusion Bahan Kuliah PakarDocument27 pagesPleura Effusion Bahan Kuliah PakarRudy LusmiandaNo ratings yet
- Pleura Effusion Bahan Kuliah PakarDocument27 pagesPleura Effusion Bahan Kuliah PakarAfifah NaurahNo ratings yet
- Respiratory Distress SyndromeDocument41 pagesRespiratory Distress Syndromef.abrahamNo ratings yet
- PE Diagnosis & TreatmentDocument3 pagesPE Diagnosis & TreatmentHeidi M FischerNo ratings yet
- Plural Effusion Presentation Adult 2... New 3 ....Document36 pagesPlural Effusion Presentation Adult 2... New 3 ....Marwa NaimNo ratings yet
- Paediatric Chest RadiologyDocument120 pagesPaediatric Chest Radiologysunielgoel100% (6)
- Gerry B. Acosta, MD, FPPS, FPCC: Pediatric CardiologistDocument51 pagesGerry B. Acosta, MD, FPPS, FPCC: Pediatric CardiologistChristian Clyde N. ApigoNo ratings yet
- Hemoptysis: Bahman Saatian, M.DDocument57 pagesHemoptysis: Bahman Saatian, M.DRovanNo ratings yet
- Pleural EffusionDocument24 pagesPleural Effusionalyas alyasNo ratings yet
- Lung Cyst Case ReportDocument64 pagesLung Cyst Case ReportJavaid Khan100% (1)
- Respiratory Diseases GuideDocument58 pagesRespiratory Diseases GuideSarahNo ratings yet
- Dr. IkhsanDocument46 pagesDr. IkhsanandiendaNo ratings yet
- Pleural Effusion 31.10.14Document25 pagesPleural Effusion 31.10.14Dr. AHBAB HUSSAINNo ratings yet
- Neonatal AnaesthesiaDocument61 pagesNeonatal AnaesthesianeneknoraNo ratings yet
- Respiratory Distress SyndromeDocument30 pagesRespiratory Distress SyndromeDennis MiritiNo ratings yet
- Gerry B. Acosta, MD, FPPS, FPCC: Pediatric CardiologistDocument51 pagesGerry B. Acosta, MD, FPPS, FPCC: Pediatric CardiologistChristian Clyde N. ApigoNo ratings yet
- Amniotic Fluid EmbolismDocument26 pagesAmniotic Fluid EmbolismAnant PachisiaNo ratings yet
- Pulmonary EmbolismDocument96 pagesPulmonary Embolismsamice5100% (1)
- RESPIRATORY Distress New NewDocument20 pagesRESPIRATORY Distress New NewAdegboye Sherifdeen AdedejiNo ratings yet
- Approach To Bleeding Child: Moderator: Dr. Ayal (MD, Pediatrician) Presenters: Wubshet K. & Yihenew D. (C-I Students)Document92 pagesApproach To Bleeding Child: Moderator: Dr. Ayal (MD, Pediatrician) Presenters: Wubshet K. & Yihenew D. (C-I Students)woldemariamNo ratings yet
- Approach to Diagnosing and Treating Pleural DiseasesDocument153 pagesApproach to Diagnosing and Treating Pleural DiseasesShanza AmaanNo ratings yet
- PLEURAL EFFUSION CAUSES AND DIAGNOSISDocument52 pagesPLEURAL EFFUSION CAUSES AND DIAGNOSISvaishnaviNo ratings yet
- Persistent Pulmonary Hypertension of The NewbornDocument32 pagesPersistent Pulmonary Hypertension of The NewbornDrSk SamimNo ratings yet
- Rare Childbirth Emergency: Amniotic Fluid EmbolismDocument5 pagesRare Childbirth Emergency: Amniotic Fluid EmbolismPatel AmeeNo ratings yet
- Name: Abdirahman Sheikh Abdillahi Farah Faculty: Clinical Officers (CO8) Course: Pediatric Lecturer: DR Amin Assingment: Pleural EffusionDocument46 pagesName: Abdirahman Sheikh Abdillahi Farah Faculty: Clinical Officers (CO8) Course: Pediatric Lecturer: DR Amin Assingment: Pleural EffusionAbdirahman Abdillahi FarahNo ratings yet
- Infantile Respiratory Distress SyndromeDocument27 pagesInfantile Respiratory Distress SyndromeRoy D RogerNo ratings yet
- Chief Complaint: Cough, Hemoptysis, Chest Pain: Kelly Kawaoka, M.D. Loma Linda University Medical CenterDocument18 pagesChief Complaint: Cough, Hemoptysis, Chest Pain: Kelly Kawaoka, M.D. Loma Linda University Medical CenterdradiagraNo ratings yet
- Chronic Lung Disease (Bronchopulmonary Dysplasia) : Intensive Care Nursery House Staff ManualDocument2 pagesChronic Lung Disease (Bronchopulmonary Dysplasia) : Intensive Care Nursery House Staff ManualPrincess AguirreNo ratings yet
- Respiratory Distress SyndromeDocument69 pagesRespiratory Distress SyndromeAbraham ChiuNo ratings yet
- Approach To A Neonate With CyanosisDocument56 pagesApproach To A Neonate With CyanosispaanarNo ratings yet
- Diseases of The Newborn IDocument40 pagesDiseases of The Newborn InewazNo ratings yet
- Pedi 2Document25 pagesPedi 2Roba ANo ratings yet
- Amniotic Fluid Embolism Clinical Presentation ReviewDocument29 pagesAmniotic Fluid Embolism Clinical Presentation ReviewArun Kumar Gupta100% (1)
- Acute CareDocument50 pagesAcute CareFrancr ToledanoNo ratings yet
- Gynae EmerganciesDocument39 pagesGynae EmerganciesgibreilNo ratings yet
- RdsDocument26 pagesRdsAsti FiandariNo ratings yet
- Pulmonary HemorrhageDocument6 pagesPulmonary HemorrhageSubas SharmaNo ratings yet
- Respiratory Distress SyndromeDocument121 pagesRespiratory Distress Syndromeinno so qtNo ratings yet
- Modul Skills KKD4 Reproduksi 2018Document31 pagesModul Skills KKD4 Reproduksi 2018rizkiya novitaNo ratings yet
- Persistent Pulmonary Hypertension of The NewbornDocument4 pagesPersistent Pulmonary Hypertension of The NewbornMarwa Adly100% (1)
- Amniotic Fluid EmbolismDocument30 pagesAmniotic Fluid EmbolismDonmer Ibañez Juan100% (1)
- Srishti Gupta - 304 - Day 15Document3 pagesSrishti Gupta - 304 - Day 15Srishti Gupta - 304No ratings yet
- Pediatric NursingDocument105 pagesPediatric NursingPaida P. Abdulmalik75% (4)
- 26. Thromboembolitic Diseases in PregnancyDocument31 pages26. Thromboembolitic Diseases in PregnancyMuwanga faizoNo ratings yet
- Pleural Effusion 23-24Document21 pagesPleural Effusion 23-24bazyan3aNo ratings yet
- PIHDocument30 pagesPIHPatcharavit PloynumponNo ratings yet
- Amniotic Fluid EmbolismDocument51 pagesAmniotic Fluid EmbolismDenyse Mayer Atutubo100% (2)
- ARDSDocument28 pagesARDSKAMLESH RATHODNo ratings yet
- Approach To Pediatric HemoptysisDocument5 pagesApproach To Pediatric HemoptysisAssma Haytham MuradNo ratings yet
- PdaDocument43 pagesPdaSandy ShahNo ratings yet
- Respiratory Distress SyndromeDocument54 pagesRespiratory Distress SyndromeKristine CaringalNo ratings yet
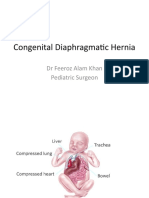
- Congenital Diaphragmatic Hernia: DR Feeroz Alam Khan Pediatric SurgeonDocument21 pagesCongenital Diaphragmatic Hernia: DR Feeroz Alam Khan Pediatric SurgeonPrabhat GuptaNo ratings yet
- Cyanotic Congenital Heart DiseaseDocument6 pagesCyanotic Congenital Heart DiseaseSimran JosanNo ratings yet
- Patent Ductus Arteriosus in Preterm Neonates: DR Deepti Damayanty Pradhan KIMS, BhubaneswarDocument58 pagesPatent Ductus Arteriosus in Preterm Neonates: DR Deepti Damayanty Pradhan KIMS, BhubaneswarDr.Sushree Smita BehuraNo ratings yet
- Rare and Interesting Cases in Pulmonary MedicineFrom EverandRare and Interesting Cases in Pulmonary MedicineRating: 4 out of 5 stars4/5 (1)
- Immediate Newborn CareDocument3 pagesImmediate Newborn CareKate Gabrielle Donal De GuzmanNo ratings yet
- LAS Q3-Health8-Week-6-8Document8 pagesLAS Q3-Health8-Week-6-8novem salonoyNo ratings yet
- English Handouts (Pormintilla)Document30 pagesEnglish Handouts (Pormintilla)Rommel BansaleNo ratings yet
- MONTHLY-JOURNAL - July 2020Document5 pagesMONTHLY-JOURNAL - July 2020Cristina MelloriaNo ratings yet
- The Effects of Emotional Intelligence in Employees PerformanceDocument16 pagesThe Effects of Emotional Intelligence in Employees PerformanceMohan SubramanianNo ratings yet
- Regional Family Planning Inventory FormsDocument2 pagesRegional Family Planning Inventory FormsRANDY BAOGBOGNo ratings yet
- Musclebear, J, R - Eat Clen Tren Hard - The Guide For Steroid Use in Powerlifting (2017)Document75 pagesMusclebear, J, R - Eat Clen Tren Hard - The Guide For Steroid Use in Powerlifting (2017)macajir6980% (2)
- Formfit: Digital Scale & Body AnalyzerDocument24 pagesFormfit: Digital Scale & Body Analyzerdon baileyNo ratings yet
- 986 Assessment of New Born NursingDocument91 pages986 Assessment of New Born NursingkrishnaNo ratings yet
- MDS Selection ListDocument5 pagesMDS Selection ListMangesh SandeNo ratings yet
- PB 7Document32 pagesPB 7Dracule MihawkNo ratings yet
- Pagadian Capitol College. Inc.: Technology and Livelihood Education 10 ExaminationDocument4 pagesPagadian Capitol College. Inc.: Technology and Livelihood Education 10 ExaminationJovelyn TakilidNo ratings yet
- Panel Outcome Letter Patient Eligible For CHC MGDocument2 pagesPanel Outcome Letter Patient Eligible For CHC MGDivine Mercy Apostolate UKNo ratings yet
- References Group Ni JanineDocument20 pagesReferences Group Ni JanineJunjun GwapoNo ratings yet
- Alert OrganismDocument40 pagesAlert OrganismSuhazeli Abdullah100% (3)
- MDC COVID-19 Mandatory Health Safety Protocols Upon Work Resumption - V5 20200513Document13 pagesMDC COVID-19 Mandatory Health Safety Protocols Upon Work Resumption - V5 20200513Clarabelle Mae Dela RosaNo ratings yet
- Pewarnaan Sederhana, KOH, LPCB Dan GramDocument51 pagesPewarnaan Sederhana, KOH, LPCB Dan GramYolandaMartaLenaNo ratings yet
- KistokelDocument4 pagesKistokelIntan PermataNo ratings yet
- TTP vs HUS: Distinguishing Features and TreatmentDocument21 pagesTTP vs HUS: Distinguishing Features and TreatmentHanif ullahNo ratings yet
- Teachers Perception of Factors Affecting School DropoutsDocument53 pagesTeachers Perception of Factors Affecting School DropoutsIchipi-ifukor Patrick Chukuyenum100% (1)
- Issue Brief NPNRSDocument1 pageIssue Brief NPNRSKristin Villaseñor-MercadoNo ratings yet
- Basic Family Relations Parental Bonding and DyadicDocument8 pagesBasic Family Relations Parental Bonding and Dyadicsanskriti gautamNo ratings yet
- Bonnie Patten Article - Self-RegulationDocument24 pagesBonnie Patten Article - Self-RegulationBill KeepNo ratings yet
- 54 GM LessonsDocument14 pages54 GM LessonsJosé VidalNo ratings yet
- Marginal Ridge Is Severely WeakenedDocument9 pagesMarginal Ridge Is Severely WeakenedChin GeslaniNo ratings yet
- Code of Ethics-American Counseling AssociationDocument51 pagesCode of Ethics-American Counseling AssociationJohn Carlo PerezNo ratings yet
- Childhood Sexual Abuse - An Umbrella ReviewDocument10 pagesChildhood Sexual Abuse - An Umbrella ReviewHarish KarthikeyanNo ratings yet
- Rapid-p0014-Oui-Apc-ltr-0230 Ouijv Rigging and Lifting Procedure RapidDocument153 pagesRapid-p0014-Oui-Apc-ltr-0230 Ouijv Rigging and Lifting Procedure RapidYo Wee LiamNo ratings yet
- Antimicrobial Stewardship Integration in EmrsDocument67 pagesAntimicrobial Stewardship Integration in Emrsapi-668616332No ratings yet
- Plan of ActivitiesDocument3 pagesPlan of ActivitiesLiiza G-GsprNo ratings yet