You might also like
- Respiratory Distress Syndrome Hmd-Ttnb-Mas-Neonatal PneumoniaDocument65 pagesRespiratory Distress Syndrome Hmd-Ttnb-Mas-Neonatal PneumoniaBLOBLOBNo ratings yet
- RDS Ppts 2021Document37 pagesRDS Ppts 2021Mohammad NajjarNo ratings yet
- RESPIRATORY Distress New NewDocument20 pagesRESPIRATORY Distress New NewAdegboye Sherifdeen AdedejiNo ratings yet
- Paediatric Chest RadiologyDocument120 pagesPaediatric Chest Radiologysunielgoel100% (6)
- Illness in The NewbornDocument34 pagesIllness in The NewbornVivian Jean TapayaNo ratings yet
- Approach To Respiratory Distress in NewbornDocument79 pagesApproach To Respiratory Distress in NewbornNikhil100% (1)
- RESPIRATORY DIS-WPS OfficeDocument12 pagesRESPIRATORY DIS-WPS OfficeGiselle EstoquiaNo ratings yet
- Respiratory Distress SyndromDocument19 pagesRespiratory Distress Syndromapi-19916399100% (2)
- Respiratory Distress in Newborn: Presented By: Dr. Walaa MousaDocument74 pagesRespiratory Distress in Newborn: Presented By: Dr. Walaa MousasalamredNo ratings yet
- Respiratory Distress SyndromeeDocument42 pagesRespiratory Distress SyndromeeRoman MamunNo ratings yet
- MK BronchiolitisDocument6 pagesMK BronchiolitisMoses Jr Kazevu100% (1)
- Respiratory DiseasesDocument58 pagesRespiratory DiseasesSarahNo ratings yet
- Peritonitis Dan PermasalahannyaDocument52 pagesPeritonitis Dan PermasalahannyaNindyNo ratings yet
- Respiratory Distress SyndromeDocument41 pagesRespiratory Distress SyndromedicksonsamboNo ratings yet
- Illness in NewbornDocument2 pagesIllness in Newbornitsjamyca najorraNo ratings yet
- Case Report "Hidrocephalus With Broncopneumonia + TB"Document24 pagesCase Report "Hidrocephalus With Broncopneumonia + TB"Indah LindianaNo ratings yet
- Pedi 2Document25 pagesPedi 2Roba ANo ratings yet
- Respiratory Distress SyndromeDocument121 pagesRespiratory Distress Syndromeinno so qtNo ratings yet
- Respiratory Distress Syndrome (Iniego Carlo Jay)Document9 pagesRespiratory Distress Syndrome (Iniego Carlo Jay)Carlojay IniegoNo ratings yet
- Respiratory Distress in NewbornDocument52 pagesRespiratory Distress in NewbornNadia SalwaniNo ratings yet
- Respiratory Distress Syndrome: NewbornDocument17 pagesRespiratory Distress Syndrome: NewbornLoloNo ratings yet
- Diseases of The Newborn IDocument40 pagesDiseases of The Newborn InewazNo ratings yet
- Respiratory Distress Sydrome Year 5-2Document36 pagesRespiratory Distress Sydrome Year 5-2chebetnaomi945No ratings yet
- Modul Skills KKD4 Reproduksi 2018Document31 pagesModul Skills KKD4 Reproduksi 2018rizkiya novitaNo ratings yet
- Respiratory Distress in The Neonate and InfantDocument8 pagesRespiratory Distress in The Neonate and InfantMikey ZhitnitskyNo ratings yet
- Anak 1Document72 pagesAnak 1Nency PurmayaNo ratings yet
- Hypoplasia of The Lung: Helmilubis Ridwanm. Daulay Wismandalimunthe RinisavitridaulayDocument29 pagesHypoplasia of The Lung: Helmilubis Ridwanm. Daulay Wismandalimunthe RinisavitridaulayM Rizky Assilmy LubisNo ratings yet
- Respiratory Distress SyndromeDocument30 pagesRespiratory Distress SyndromeDennis MiritiNo ratings yet
- Pedia Concepts 2:: From Respiratory Problems To HematologicDocument119 pagesPedia Concepts 2:: From Respiratory Problems To HematologicarudarbmeeNo ratings yet
- Goljan Respiratory NotesDocument21 pagesGoljan Respiratory Notesmedic2424100% (1)
- Neonatal PneumoniaDocument16 pagesNeonatal Pneumoniaelyuchan100% (1)
- 1) Respiratory Distress Syndrome (RDS) Hyaline Membrane Disease (HMD)Document9 pages1) Respiratory Distress Syndrome (RDS) Hyaline Membrane Disease (HMD)ُEssraa AdeelNo ratings yet
- Croup: Dr. Shveta Sethi Narula A.P. MicrobiologyDocument14 pagesCroup: Dr. Shveta Sethi Narula A.P. Microbiology12. Akshit AtwalNo ratings yet
- (Ped-W1) (Dr. Zuhair M. Al Musawi) Repiratory 2Document43 pages(Ped-W1) (Dr. Zuhair M. Al Musawi) Repiratory 2Haider Nadhem AL-rubaiNo ratings yet
- Kel Kongenital HMDDocument15 pagesKel Kongenital HMDSilvia RizkaNo ratings yet
- #10 - NCM109 (Pedia) - TransesDocument70 pages#10 - NCM109 (Pedia) - TransesJaimie BanaagNo ratings yet
- Paed Respiratory DistressDocument45 pagesPaed Respiratory Distressaboje ochekwuNo ratings yet
- Ass. of NewbornDocument54 pagesAss. of NewbornMahad Maxamed AxmedNo ratings yet
- Respiratory Distress SyndromeDocument41 pagesRespiratory Distress Syndromef.abrahamNo ratings yet
- Transient Tachypnea of The Newborn OutlineDocument7 pagesTransient Tachypnea of The Newborn OutlineMarceline GarciaNo ratings yet
- Respiratory Distress SyndromeDocument13 pagesRespiratory Distress SyndromeKenneth UbaldeNo ratings yet
- Pulmonary Hemorrhage: Dr. Habibur RahimDocument46 pagesPulmonary Hemorrhage: Dr. Habibur Rahimallaaobeid1987No ratings yet
- RD in Newborn by Yong Part 2Document37 pagesRD in Newborn by Yong Part 2semangat akreNo ratings yet
- Sistem Respirasi Sesak Napas: Problem Based LearningDocument61 pagesSistem Respirasi Sesak Napas: Problem Based LearningAkbar IskandarNo ratings yet
- Infant Respiratory Distress SyndromeDocument39 pagesInfant Respiratory Distress SyndromeIoana MuntianuNo ratings yet
- NEONATAL APNOEA SMNRDocument18 pagesNEONATAL APNOEA SMNRAswathy RC100% (1)
- Kelainan Kongenital 2010Document29 pagesKelainan Kongenital 2010Winson ChitraNo ratings yet
- Abnormality in NeonatesDocument30 pagesAbnormality in NeonatesEggyDsNo ratings yet
- Lower Respiratory Tract Diseases - KeyDocument45 pagesLower Respiratory Tract Diseases - KeyYugmaPandyaNo ratings yet
- Respiratory Distress Syndrome: Islamic University Nursing CollegeDocument21 pagesRespiratory Distress Syndrome: Islamic University Nursing Collegeyaumil agisnaNo ratings yet
- Congenital Cystic Adenomatoid Malformation (CCAM)Document7 pagesCongenital Cystic Adenomatoid Malformation (CCAM)sarguss14No ratings yet
- Eni Rahmawati, S.Kep., NS., M.KepDocument46 pagesEni Rahmawati, S.Kep., NS., M.KepLisa Qoriana RohmaniNo ratings yet
- Amniotic Fluid Disoder: Muhammad IzzatDocument26 pagesAmniotic Fluid Disoder: Muhammad IzzatcopperNo ratings yet
- Croup (Laryngotracheobronchitis) : EtiologyDocument13 pagesCroup (Laryngotracheobronchitis) : EtiologyOmar mohamedNo ratings yet
- Hyaline Membrane Disease-1Document24 pagesHyaline Membrane Disease-1JOSLIN100% (1)
- SGADocument5 pagesSGAChary HorladorNo ratings yet
- Medical Mnemonic Sketches : Pulmonary DiseasesFrom EverandMedical Mnemonic Sketches : Pulmonary DiseasesNo ratings yet
- Rare and Interesting Cases in Pulmonary MedicineFrom EverandRare and Interesting Cases in Pulmonary MedicineRating: 4 out of 5 stars4/5 (1)
- Autoimmune Disease Clinical Research: ExpertsDocument2 pagesAutoimmune Disease Clinical Research: ExpertsRoy D RogerNo ratings yet
- The Influenza & Parainfluenza VirusesDocument35 pagesThe Influenza & Parainfluenza VirusesRoy D RogerNo ratings yet
- Methods and Technique of Endoscopic Research of ENT-organs. Clinical Anatomy and Physiology of Auditory AnalyzerDocument56 pagesMethods and Technique of Endoscopic Research of ENT-organs. Clinical Anatomy and Physiology of Auditory AnalyzerRoy D RogerNo ratings yet
- Agarwal2014 Article TreatmentAndPreventionOfRhIsoiDocument8 pagesAgarwal2014 Article TreatmentAndPreventionOfRhIsoiRoy D RogerNo ratings yet
- CH 24Document3 pagesCH 24Roy D RogerNo ratings yet
- Hypotonic Hypohydration .Metabolic Acidosis. Classification of Acute PoisoningDocument2 pagesHypotonic Hypohydration .Metabolic Acidosis. Classification of Acute PoisoningRoy D RogerNo ratings yet
- Reference ID: 3975973Document2 pagesReference ID: 3975973Aldrin LampareroNo ratings yet
- Endoscopic Diagnosis of Diseases of The Intestine.Document12 pagesEndoscopic Diagnosis of Diseases of The Intestine.Roy D RogerNo ratings yet
- Case Study - Multiple SclerosisDocument11 pagesCase Study - Multiple SclerosisMyrhaida BairullaNo ratings yet
- Concluding Lesson-1Document5 pagesConcluding Lesson-1Roy D RogerNo ratings yet
- Workbook 2016 StomDocument186 pagesWorkbook 2016 StomAysenNo ratings yet
- Laparoscopic Repair of Perforated Duodenal UlcerDocument3 pagesLaparoscopic Repair of Perforated Duodenal UlcerRoy D RogerNo ratings yet
- Advantages and Disadvantages of Ultra Sonic Skin Care DevicesDocument3 pagesAdvantages and Disadvantages of Ultra Sonic Skin Care DevicesMuqarrub Ali KhanNo ratings yet
- Case Study - Tennis Elbow: Suresh BandaruDocument9 pagesCase Study - Tennis Elbow: Suresh BandaruCarl MacCordNo ratings yet
- Duodenal GistDocument5 pagesDuodenal Gistmudasir61No ratings yet
- PolydactylyDocument16 pagesPolydactylyGupies100% (1)
- International Classification of Diseases: Presented By: DR Arijit Kundu Guided By: Prof. Sumitra PattanaikDocument56 pagesInternational Classification of Diseases: Presented By: DR Arijit Kundu Guided By: Prof. Sumitra PattanaikpriyagerardNo ratings yet
- Goljan Errata SheetDocument11 pagesGoljan Errata SheetVishala MishraNo ratings yet
- Determination of DeathDocument8 pagesDetermination of DeathZam PamateNo ratings yet
- Peripheral Nerve Field Stimulation For Sacroiliac Joint PainDocument4 pagesPeripheral Nerve Field Stimulation For Sacroiliac Joint PainAna Cristina MartinsNo ratings yet
- Ear, Nose and Throat EmergenciesDocument3 pagesEar, Nose and Throat Emergenciesfmta100% (1)
- Ass Triangle of Human EcologyDocument6 pagesAss Triangle of Human EcologyClarissa Marie Limmang100% (1)
- Super Final 220-Zoonotic Infectious Diseases Exam Questions 8 SOLVED by ANKIT AKELADocument37 pagesSuper Final 220-Zoonotic Infectious Diseases Exam Questions 8 SOLVED by ANKIT AKELAYara AlmouallemNo ratings yet
- Tomografía Computarizada para El Diagnóstico de La Apendicitis Aguda en Pacientes AdultosDocument199 pagesTomografía Computarizada para El Diagnóstico de La Apendicitis Aguda en Pacientes AdultosMarco Jimenez HerreraNo ratings yet
- Nurselabs PEDIA QuestionsDocument13 pagesNurselabs PEDIA QuestionsSteffi MurielNo ratings yet
- Hematologic System Practice QuestionsDocument3 pagesHematologic System Practice QuestionsJoslyn GrossNo ratings yet
- Proceedings of The 16th Italian Association of Equine Veterinarians CongressDocument4 pagesProceedings of The 16th Italian Association of Equine Veterinarians CongressCabinet VeterinarNo ratings yet
- What Are Bacteria - Streptococcus FaecalisDocument3 pagesWhat Are Bacteria - Streptococcus FaecalisAnkan PalNo ratings yet
- Nursing Care Plan Diarrhea Assessment Diagnosis Planning Interventions Rationale EvaluationDocument8 pagesNursing Care Plan Diarrhea Assessment Diagnosis Planning Interventions Rationale EvaluationKrahNo ratings yet
- PTS - Soal Bahasa Inggris Kelas IXDocument6 pagesPTS - Soal Bahasa Inggris Kelas IXRini YusmayantiNo ratings yet
- Food HygieneDocument31 pagesFood Hygienehemihema100% (1)
- Name of The Course:-M.Phil, Economics: Result of Delhi University Entrance Test (DUET) - 2018Document5 pagesName of The Course:-M.Phil, Economics: Result of Delhi University Entrance Test (DUET) - 2018Saiganesh RameshNo ratings yet
- Types of Diabetes MellitusDocument5 pagesTypes of Diabetes MellitusKlinik MaleoNo ratings yet
- HCIA Study Guide 2023Document22 pagesHCIA Study Guide 2023consultasluisfloresdrNo ratings yet
- 2803NRS Acute Nursing Practice Exam NotesDocument18 pages2803NRS Acute Nursing Practice Exam NotesGrace CallowNo ratings yet
- Document PDFDocument11 pagesDocument PDFYANDA PELIA ANo ratings yet
- NEJM Image Challenges Album Part 4 2014 PDFDocument56 pagesNEJM Image Challenges Album Part 4 2014 PDFAntoun Kamel100% (1)
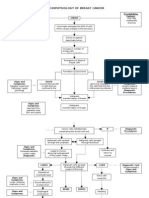
- Pathophysiology of Breast Cancer: Unkno Predisposing Factors: Precipitating FactorsDocument3 pagesPathophysiology of Breast Cancer: Unkno Predisposing Factors: Precipitating FactorsKevin Ercia100% (1)
- Thromboembolic Disease PDFDocument5 pagesThromboembolic Disease PDFBáĦẳá Y. Ẳl-mársǾúmiNo ratings yet
- Ismail's Undergraduate ThesisDocument82 pagesIsmail's Undergraduate ThesisAbiola IbrahimNo ratings yet
- Anthroposophical Approach To Cancer Rita Leroi MDDocument26 pagesAnthroposophical Approach To Cancer Rita Leroi MD144bob144No ratings yet
- 1 s2.0 S014067362300020X MainDocument14 pages1 s2.0 S014067362300020X MainGERIATRIA 72No ratings yet