You might also like
- Marsden Victor Emile - The Protocols of ZionDocument156 pagesMarsden Victor Emile - The Protocols of ZionPeter100% (4)
- SOAP Note Cheat Sheet - Complete H&PDocument2 pagesSOAP Note Cheat Sheet - Complete H&PAdeline N. Omene95% (19)
- AWR160 WMD AnswersDocument32 pagesAWR160 WMD Answersthatguy8950% (4)
- 1957 - Wasson - Life Magazine - Secret of Divine Mushrooms (Web) PDFDocument31 pages1957 - Wasson - Life Magazine - Secret of Divine Mushrooms (Web) PDFSam Ruger100% (1)
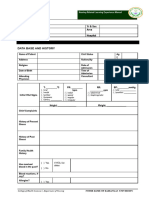
- Obstetric FormDocument4 pagesObstetric FormKhylamarie VillalunaNo ratings yet
- Pre-Employment Medical FormDocument2 pagesPre-Employment Medical FormSourin NandiNo ratings yet
- Pediatric Assessment 1 12 PDFDocument11 pagesPediatric Assessment 1 12 PDFJackieNate Ortiz100% (1)
- Case Study IcuDocument31 pagesCase Study Icujanna mae patriarcaNo ratings yet
- Postnatal Assessment Tool M.SC NSGDocument12 pagesPostnatal Assessment Tool M.SC NSGM. jehovah Nissie YeshalomeNo ratings yet
- Pediatrics Wards History Taking TemplateDocument2 pagesPediatrics Wards History Taking TemplateBobet Reña80% (5)
- Pediatric History OutlineDocument12 pagesPediatric History OutlineDawn MarcoNo ratings yet
- LAW 3100 - Persons & Family Relations - JD 33. G.R. No. 221029 - Republic vs. Manalo - Case Digest 8Document5 pagesLAW 3100 - Persons & Family Relations - JD 33. G.R. No. 221029 - Republic vs. Manalo - Case Digest 8John Kenneth ContrerasNo ratings yet
- Aisc Quality ManualDocument404 pagesAisc Quality Manualvo thi kim xuyenNo ratings yet
- History Taking FormDocument14 pagesHistory Taking FormFebbie ArcalesNo ratings yet
- Labor Case Digest CompilationDocument119 pagesLabor Case Digest CompilationErvin CavalidaNo ratings yet
- Quantity SurveyingDocument9 pagesQuantity Surveyingshijinrajagopal100% (4)
- IMNPD AssignmentDocument49 pagesIMNPD AssignmentSreePrakash100% (3)
- CMA DataDocument36 pagesCMA DataPramod GuptaNo ratings yet
- Factors Affecting Property Value PDFDocument2 pagesFactors Affecting Property Value PDFJennifer100% (1)
- I. Preoperative Assessment 1. Physical: Philippine Heart Center Perioperative Nursing RecordDocument2 pagesI. Preoperative Assessment 1. Physical: Philippine Heart Center Perioperative Nursing RecordERWINNo ratings yet
- Pediatric Initial Patient HistoryDocument11 pagesPediatric Initial Patient HistoryLinh TrịnhNo ratings yet
- Biofuel Production From Citrus Wastes IranDocument13 pagesBiofuel Production From Citrus Wastes IranRoberto Moreno MuñozNo ratings yet
- Kevin The Dino: Free Crochet PatternDocument3 pagesKevin The Dino: Free Crochet PatternMarina Assa100% (4)
- Family Healthcare Program FORMDocument12 pagesFamily Healthcare Program FORMRaquel ReyesNo ratings yet
- San Beda College of Medicine Batch 2017 Neuro-Pedia ChecklistDocument9 pagesSan Beda College of Medicine Batch 2017 Neuro-Pedia ChecklistAngelaTrinidadNo ratings yet
- Newborn Screening Continuity Clinic Initial Consult Form Ncr/MimaropaDocument3 pagesNewborn Screening Continuity Clinic Initial Consult Form Ncr/Mimaropajacqueline licupNo ratings yet
- Pediatric History Taking Chart PDFDocument2 pagesPediatric History Taking Chart PDFHerlene Lyneth ZalamedaNo ratings yet
- Health Examination RecordDocument4 pagesHealth Examination Recordmary joy dela cruzNo ratings yet
- Paediatrics History + Examination Format-2Document4 pagesPaediatrics History + Examination Format-2Salim KhaleelNo ratings yet
- Family Health Assessment Form: University of San Jose-Recoletos School of Allied Medical Sciences NursingDocument4 pagesFamily Health Assessment Form: University of San Jose-Recoletos School of Allied Medical Sciences NursingIvan A. EleginoNo ratings yet
- 2.physical E, HISTORY NCPDocument13 pages2.physical E, HISTORY NCPمريم حجيNo ratings yet
- Assessment Guide ToddlerDocument2 pagesAssessment Guide ToddlerOla Anna GamutinNo ratings yet
- Prenatal Check Up InterviewDocument7 pagesPrenatal Check Up InterviewSHIELOU LOMODNo ratings yet
- Medical-History-Form 1Document2 pagesMedical-History-Form 1api-743136931No ratings yet
- Ah TemplateDocument4 pagesAh TemplateellalasadaNo ratings yet
- Migrant Health FormDocument5 pagesMigrant Health FormImelda Junaedi100% (3)
- Pedia Case ProtocolDocument5 pagesPedia Case ProtocolAllene PaderangaNo ratings yet
- Postpartum AssessmentDocument5 pagesPostpartum AssessmentJor BangsNo ratings yet
- Neuropreceptorial ChecklistDocument33 pagesNeuropreceptorial ChecklistAlloiBialba0% (1)
- Prenatal PHN BagDocument4 pagesPrenatal PHN BagStuart BlackNo ratings yet
- 1 Patient Health History and Health Assessment FormatDocument8 pages1 Patient Health History and Health Assessment FormatKn VelasquezNo ratings yet
- 1 Patient Health History and Health Assessment FormatDocument9 pages1 Patient Health History and Health Assessment Formatgwendee ealdamaNo ratings yet
- Case Study Questionnaire For Malnourished ChildrenDocument5 pagesCase Study Questionnaire For Malnourished ChildrenSta Cruz BacnotanNo ratings yet
- 1 Patient Health History and Health Assessment Format 1Document9 pages1 Patient Health History and Health Assessment Format 1Airaa ShaneNo ratings yet
- Ateneo Higher Education Health Services Office Ateneo de Naga University Ateneo Avenue, Bagumbayan Sur, Naga CityDocument2 pagesAteneo Higher Education Health Services Office Ateneo de Naga University Ateneo Avenue, Bagumbayan Sur, Naga CityKatherine VerceluzNo ratings yet
- Central Mindanao University College of Nursing Preschool Assessment FormDocument6 pagesCentral Mindanao University College of Nursing Preschool Assessment FormKyleRepolidon MoralesNo ratings yet
- OB Patho Assessment Tool EditedDocument6 pagesOB Patho Assessment Tool EditedDarren RobertoNo ratings yet
- Record of Newborn CareDocument1 pageRecord of Newborn CareMarie Antionette MondragonNo ratings yet
- Annex A1: Print Legibly. Mark Appropriate Boxes C With " "Document21 pagesAnnex A1: Print Legibly. Mark Appropriate Boxes C With " "allen zacariasNo ratings yet
- PEDO Forms To PrintDocument4 pagesPEDO Forms To PrintMONIQUE QUIMZONNo ratings yet
- Lasustech Medical FormDocument2 pagesLasustech Medical FormAl MubarakNo ratings yet
- Student Health Record Form - FrontDocument1 pageStudent Health Record Form - FrontESPOS JEMS MYKELNo ratings yet
- Pediatric History TemplateDocument6 pagesPediatric History TemplateseroshNo ratings yet
- Blank Neurodevelopmental Intake FormDocument2 pagesBlank Neurodevelopmental Intake FormjhecyNo ratings yet
- HA 1st Lecture Health HistoryDocument7 pagesHA 1st Lecture Health HistoryChilled Moo MooNo ratings yet
- Saint Louis University School of Medicine Department of Medicine General Data: Past Medical HistoryDocument3 pagesSaint Louis University School of Medicine Department of Medicine General Data: Past Medical HistoryMarieCrisNo ratings yet
- New P.E FormDocument5 pagesNew P.E FormSt. John ClinicNo ratings yet
- NSD FORMAT EndorsementDocument5 pagesNSD FORMAT EndorsementMarco Bryan G. DueroNo ratings yet
- NSD FormatDocument4 pagesNSD FormatAla'a Emerald AguamNo ratings yet
- Pediatric Intake Form SampleDocument10 pagesPediatric Intake Form SampleТравма ЮніверсумNo ratings yet
- Labor Room: Name - Age - Case No.Document15 pagesLabor Room: Name - Age - Case No.deamhi nursing serviceNo ratings yet
- Student Health Record PDFDocument2 pagesStudent Health Record PDFailen joy villoNo ratings yet
- Universidad de Manila College of Nursing Community Health Survey ToolDocument9 pagesUniversidad de Manila College of Nursing Community Health Survey Toolaina_boydonNo ratings yet
- Viral Haemorrhagic Fever - Case Investigation Form: Date of Detection of The Case Case IDDocument3 pagesViral Haemorrhagic Fever - Case Investigation Form: Date of Detection of The Case Case IDSalihu MustaphaNo ratings yet
- Infant SeeDocument1 pageInfant Seeapi-13229096No ratings yet
- Pediatric AssessmentDocument6 pagesPediatric AssessmentChu BagunuNo ratings yet
- Rle Worksheet: Labor Room and Delivery RoomDocument15 pagesRle Worksheet: Labor Room and Delivery RoomLalisaM Activity100% (1)
- ANTENATAL Assessment FINALDocument12 pagesANTENATAL Assessment FINALM. jehovah Nissie YeshalomeNo ratings yet
- Assessment Tool of Mu SysDocument60 pagesAssessment Tool of Mu SysBeulah DasariNo ratings yet
- DR Langford1Document8 pagesDR Langford1Spencer JacksonNo ratings yet
- Essential Medical Disorders of the Stomach and Small Intestine: A Clinical CasebookFrom EverandEssential Medical Disorders of the Stomach and Small Intestine: A Clinical CasebookNo ratings yet
- Reproduction & Development: Essential Biology Self-Teaching GuideFrom EverandReproduction & Development: Essential Biology Self-Teaching GuideNo ratings yet
- Goso DpaDocument2 pagesGoso DpaBroward MadrioNo ratings yet
- PO BOX 177, SAFAT 13002, KUWAIT, C.R. 81300, Share Capital-17350000 17350000, 81300 . ., , 13002 177: . .Document1 pagePO BOX 177, SAFAT 13002, KUWAIT, C.R. 81300, Share Capital-17350000 17350000, 81300 . ., , 13002 177: . .Broward MadrioNo ratings yet
- DOH 13 Herbal MedicineDocument37 pagesDOH 13 Herbal MedicineBroward MadrioNo ratings yet
- Lec 1 Public Health Nursing OverviewDocument30 pagesLec 1 Public Health Nursing OverviewBroward MadrioNo ratings yet
- 9 Maternal Child Health ProgramsDocument57 pages9 Maternal Child Health ProgramsBroward MadrioNo ratings yet
- Louis BegleyDocument8 pagesLouis BegleyPatsy StoneNo ratings yet
- Mike Johnson The Rules of Engagement Life-Work Balance and Employee Commitment 2004Document225 pagesMike Johnson The Rules of Engagement Life-Work Balance and Employee Commitment 2004Perfect_Two100% (1)
- Tanesco OverviewDocument55 pagesTanesco Overviewhamdani ramadhaniNo ratings yet
- Pak Afghan Relations PDFDocument16 pagesPak Afghan Relations PDFMOHAMMAD KASHIFNo ratings yet
- TP 2Document3 pagesTP 2api-282173119No ratings yet
- Module 14 EquityDocument17 pagesModule 14 EquityZyril RamosNo ratings yet
- RBI Finance PDFDocument28 pagesRBI Finance PDFbiswashswayambhuNo ratings yet
- The Divine Bhrgu SamhitaDocument4 pagesThe Divine Bhrgu SamhitaJohn BregenzaNo ratings yet
- TN Booklet LandscapeDocument4 pagesTN Booklet LandscapeChrisss Z.No ratings yet
- Dissertation PrelimnariesreportDocument5 pagesDissertation PrelimnariesreportHarshita BhanawatNo ratings yet
- Canal Bank WalkDocument5 pagesCanal Bank Walkmajellamccoy37No ratings yet
- College Board BigFuture College Profile CDS Import 2022 2023Document154 pagesCollege Board BigFuture College Profile CDS Import 2022 2023Nguyen PhuongNo ratings yet
- TC - 96 (Respondent)Document31 pagesTC - 96 (Respondent)20225 SALONEE SHARMANo ratings yet
- Introduction To Internet of Things Assignment-Week 9Document6 pagesIntroduction To Internet of Things Assignment-Week 9Mr.M. ArivalaganNo ratings yet
- Azure Ea Us - Bif - Sow Template Fy15Document5 pagesAzure Ea Us - Bif - Sow Template Fy15SergeyNo ratings yet
- Pilar, BataanDocument2 pagesPilar, BataanSunStar Philippine NewsNo ratings yet
- Test For The Honors ClassDocument9 pagesTest For The Honors Classapi-592588138No ratings yet
- Book of Mormon: Scripture Stories Coloring BookDocument22 pagesBook of Mormon: Scripture Stories Coloring BookJEJESILZANo ratings yet