You might also like
- Diagnosis and Management of EctopicDocument11 pagesDiagnosis and Management of EctopicBaiq DysaNo ratings yet
- Scar PregnancyDocument11 pagesScar Pregnancyasshagab04No ratings yet
- Spontaneous Preterm Birth Prevention in Multiple PregnancyDocument7 pagesSpontaneous Preterm Birth Prevention in Multiple PregnancyElias Melo JrNo ratings yet
- Acog Practice Bulletin Summary: Multifetal Gestations: Twin, Triplet, and Higher-Order Multifetal PregnanciesDocument4 pagesAcog Practice Bulletin Summary: Multifetal Gestations: Twin, Triplet, and Higher-Order Multifetal PregnanciesMariana Hernandez100% (2)
- Practice Bulletin Summary: Multifetal Gestations: Twin, Triplet, and Higher-Order Multifetal PregnanciesDocument3 pagesPractice Bulletin Summary: Multifetal Gestations: Twin, Triplet, and Higher-Order Multifetal PregnancieselmerNo ratings yet
- Management of Monochorionic Twin Pregnancy: Green-Top Guideline No. 51Document13 pagesManagement of Monochorionic Twin Pregnancy: Green-Top Guideline No. 51indra_strongNo ratings yet
- TOG Advanced Abdominal Pregnancy 2022Document10 pagesTOG Advanced Abdominal Pregnancy 2022MarNo ratings yet
- Thesis On Ectopic Pregnancy in IndiaDocument7 pagesThesis On Ectopic Pregnancy in Indiaynwtcpwff100% (2)
- RCOG Guidelines - Gestational Trophoblastic DiseaseDocument12 pagesRCOG Guidelines - Gestational Trophoblastic Diseasemob3100% (1)
- The Role of Ultrasound in ObstetricsDocument9 pagesThe Role of Ultrasound in ObstetricsHanun FaizaNo ratings yet
- Good Clinical Practice Advice: Management of Twin PregnancyDocument8 pagesGood Clinical Practice Advice: Management of Twin PregnancyHambrian WijayaNo ratings yet
- Tog 12753Document7 pagesTog 12753Saeed HasanNo ratings yet
- Obgyn Ob PRPM Pt1 13Document6 pagesObgyn Ob PRPM Pt1 13SalmonteNo ratings yet
- Multiple Pregnancy GuidelineDocument12 pagesMultiple Pregnancy GuidelineAlia BangeshNo ratings yet
- Complications in Pregnancies After in Vitro Fertilization and Embryo TransferDocument4 pagesComplications in Pregnancies After in Vitro Fertilization and Embryo TransferBilal SalaamNo ratings yet
- Optimum Timing For Planned Delivery of Uncomplicated Monochorionic and Dichorionic Twin PregnanciesDocument10 pagesOptimum Timing For Planned Delivery of Uncomplicated Monochorionic and Dichorionic Twin PregnanciesNuzma AnbiaNo ratings yet
- Santana 2019Document12 pagesSantana 2019gcereiraaNo ratings yet
- GTN 6Document13 pagesGTN 6giant nitaNo ratings yet
- The "Vanishing Twin" Syndrome - A Myth or Clinical Reality in The Obstetric Practice?Document3 pagesThe "Vanishing Twin" Syndrome - A Myth or Clinical Reality in The Obstetric Practice?ariniNo ratings yet
- Deense Studie PDFDocument12 pagesDeense Studie PDFBas HermansNo ratings yet
- OB - 02 - Outcomes of Multifetal ReductionDocument6 pagesOB - 02 - Outcomes of Multifetal Reductionram4a5No ratings yet
- Anestesia FetalDocument13 pagesAnestesia FetalPauPatiñoNo ratings yet
- Caesarean Birth and Risk of Subsequent Preterm Birth: A Retrospective Cohort StudyDocument9 pagesCaesarean Birth and Risk of Subsequent Preterm Birth: A Retrospective Cohort Studyluis albenis mendoza guerraNo ratings yet
- Wolters 2021Document9 pagesWolters 2021Triaprasetya HadiNo ratings yet
- Practice Bulletin No 144 Multifetal Gestations .40Document15 pagesPractice Bulletin No 144 Multifetal Gestations .40Jose Luis Morales Bautista100% (1)
- Temmerman2016 PDFDocument2 pagesTemmerman2016 PDFBea SphNo ratings yet
- Pi Is 0015028213007073Document7 pagesPi Is 0015028213007073Jhue hanNo ratings yet
- Management of Multiple Gestations: Mary E. D'Alton - Noelle BreslinDocument7 pagesManagement of Multiple Gestations: Mary E. D'Alton - Noelle BreslinAnonymous nhaFUpOLNo ratings yet
- Best Practice & Research Clinical Obstetrics and GynaecologyDocument14 pagesBest Practice & Research Clinical Obstetrics and Gynaecologysarahreiza miNo ratings yet
- Optimizing The Definition of Intrauterine Growth Restriction: The Multicenter Prospective PORTO StudyDocument6 pagesOptimizing The Definition of Intrauterine Growth Restriction: The Multicenter Prospective PORTO StudyfujimeisterNo ratings yet
- Care in Pregnancies Subsequent To Stillbirthor Perinatal DeatDocument12 pagesCare in Pregnancies Subsequent To Stillbirthor Perinatal DeatgalalNo ratings yet
- Manejo Cancer in Pregnancy Fetal and Neonatal OutcomesDocument17 pagesManejo Cancer in Pregnancy Fetal and Neonatal OutcomesLaura LealNo ratings yet
- 11 Abnormal PlacentationDocument29 pages11 Abnormal PlacentationMaria Gabriela CristanchoNo ratings yet
- C-Obs 42 Management of Monochorionic Twins New Mar 11Document4 pagesC-Obs 42 Management of Monochorionic Twins New Mar 11indra_strongNo ratings yet
- Aggressive Intervention of Previable Preterm Premature Rupture of MembranesDocument8 pagesAggressive Intervention of Previable Preterm Premature Rupture of MembranesVanessa Riaño GodoyNo ratings yet
- Objectives:: CorrespondenceDocument5 pagesObjectives:: Correspondenceraudatul jannahNo ratings yet
- Potdar 2020Document8 pagesPotdar 2020Christian Leonardo Molina HinojosaNo ratings yet
- Seminars in Fetal & Neonatal Medicine: Ellen Knox, William MartinDocument5 pagesSeminars in Fetal & Neonatal Medicine: Ellen Knox, William MartinSean WintersNo ratings yet
- Consumption Coagulopathy Following Single Fetal Demise in Second Trimester Dcda Twin Pregnancy-A Rare Case ReportDocument3 pagesConsumption Coagulopathy Following Single Fetal Demise in Second Trimester Dcda Twin Pregnancy-A Rare Case ReportIJAR JOURNALNo ratings yet
- Acta Obstet Gynecol Scand - 2011 - STJERNHOLM - Changed Indications For Cesarean SectionsDocument5 pagesActa Obstet Gynecol Scand - 2011 - STJERNHOLM - Changed Indications For Cesarean SectionsAli QuwarahNo ratings yet
- Malignancies in Pregnancy Multiple 2016 Best Practice Research ClinicalDocument8 pagesMalignancies in Pregnancy Multiple 2016 Best Practice Research ClinicalorriNo ratings yet
- Trial of Labor at The Maternity Department of The Sourosanou University Hospital (Chuss) : Clinical Aspects, The Maternal and Perinatal PrognosticsDocument8 pagesTrial of Labor at The Maternity Department of The Sourosanou University Hospital (Chuss) : Clinical Aspects, The Maternal and Perinatal PrognosticsIJAR JOURNALNo ratings yet
- Pitfalls of Prenatal Diagnosis Associated With Mosaicism TOGDocument10 pagesPitfalls of Prenatal Diagnosis Associated With Mosaicism TOGMarNo ratings yet
- Acute Inversion of The Uterus PDFDocument6 pagesAcute Inversion of The Uterus PDFEvelyn TingNo ratings yet
- Prevention of Preterm LabDocument6 pagesPrevention of Preterm LabDanTe D' WinchesterNo ratings yet
- ACOG SMFM Joint Practice Bulletin Multiple Gestation 2004Document15 pagesACOG SMFM Joint Practice Bulletin Multiple Gestation 2004Reza ZulkarnainNo ratings yet
- Jsafog 13 137Document5 pagesJsafog 13 137Elizabeth Duprat GaxiolaNo ratings yet
- Current Trends in ObstetricsDocument6 pagesCurrent Trends in ObstetricsShyrra Edades Pinder100% (1)
- b2 10 1Document9 pagesb2 10 1Tio Ayahnya AtharNo ratings yet
- Acta Obstet Gynecol Scand 2023 Oct 27 Khalaf S ADocument10 pagesActa Obstet Gynecol Scand 2023 Oct 27 Khalaf S ABALTAZAR OTTONELLONo ratings yet
- 1 s2.0 S0020729209615502 Main PDFDocument1 page1 s2.0 S0020729209615502 Main PDFPaula UrsuNo ratings yet
- Recurrent Pregnancy LossDocument19 pagesRecurrent Pregnancy LossSean NamNo ratings yet
- Guidelines For The Management of Postterm Pregnancy: Journal of Perinatal Medicine February 2010Document10 pagesGuidelines For The Management of Postterm Pregnancy: Journal of Perinatal Medicine February 2010Hafif Fitra Alief SultanaNo ratings yet
- A Study On Risk of Twin PregnancyDocument12 pagesA Study On Risk of Twin PregnancyINDHUMATHI R SUBBUNo ratings yet
- 6 - Preterm Pregnancy With Sacrococcygeal TeratomaDocument5 pages6 - Preterm Pregnancy With Sacrococcygeal TeratomarobertuserikkantonaNo ratings yet
- Twin PregnancyDocument20 pagesTwin PregnancyReynaldo Ali MarazaNo ratings yet
- Cystic Fibrosis and PregnancyDocument2 pagesCystic Fibrosis and Pregnancyscience world publishingNo ratings yet
- 2015 Sep Embarazo Múltiple - Vía Del Parto.Document13 pages2015 Sep Embarazo Múltiple - Vía Del Parto.Alexander Gonzalez BarturenNo ratings yet
- Brewer 2011Document17 pagesBrewer 2011Iman BousnaneNo ratings yet
- osteoprosisDocument48 pagesosteoprosissaeed hasan saeedNo ratings yet
- Tog 12685Document3 pagesTog 12685saeed hasan saeedNo ratings yet
- Potdar 2020Document8 pagesPotdar 2020Christian Leonardo Molina HinojosaNo ratings yet
- Tog 12665Document13 pagesTog 12665saeed hasan saeed100% (1)
- Tog 12709Document7 pagesTog 12709saeed hasan saeed100% (1)
- Tog 12703Document4 pagesTog 12703saeed hasan saeedNo ratings yet
- Tog 12620Document12 pagesTog 12620saeed hasan saeedNo ratings yet
- Tog 12625Document8 pagesTog 12625saeed hasan saeedNo ratings yet
- 2 - ANC After ART TOG 2020Document11 pages2 - ANC After ART TOG 2020Muhammad Javed GabaNo ratings yet
- TPP Tratamento 2021Document18 pagesTPP Tratamento 2021João Marcelo ColunaNo ratings yet
- Does Ovarian Cystectomy Pose A Risk To Ovarian Reserve and Fertility?Document10 pagesDoes Ovarian Cystectomy Pose A Risk To Ovarian Reserve and Fertility?Mohmd AboelkheirNo ratings yet
- Tog 12619Document6 pagesTog 12619saeed hasan saeedNo ratings yet
- Brier Ley 2020Document8 pagesBrier Ley 2020kemoNo ratings yet
- Tog 12643Document3 pagesTog 12643saeed hasan saeedNo ratings yet
- CPD 1, 2021Document5 pagesCPD 1, 2021saeed hasan saeedNo ratings yet
- 1471-0528 16283Document8 pages1471-0528 16283saeed hasan saeedNo ratings yet
- Care in Pregnancies Subsequent To Stillbirthor Perinatal DeatDocument12 pagesCare in Pregnancies Subsequent To Stillbirthor Perinatal DeatgalalNo ratings yet
- CLP Womens Health Preterm Clin Assess at Risk Hcs 183 01Document18 pagesCLP Womens Health Preterm Clin Assess at Risk Hcs 183 01saeed hasan saeedNo ratings yet
- Medical Spectrum Twente, Enschede, 2. Retired GynecologistDocument1 pageMedical Spectrum Twente, Enschede, 2. Retired Gynecologistsaeed hasan saeedNo ratings yet
- Understanding the Factors that Influence CA125 LevelsDocument7 pagesUnderstanding the Factors that Influence CA125 Levelsaish25No ratings yet
- Tog 12150Document10 pagesTog 12150saeed hasan saeedNo ratings yet
- Guideline 449 enDocument279 pagesGuideline 449 ensaeed hasan saeedNo ratings yet
- Cerclage DKDocument57 pagesCerclage DKsaeed hasan saeedNo ratings yet
- TOG 2007 915-20 Review Cardiac Disease in Pregnancy Part 1 CongenitalDocument6 pagesTOG 2007 915-20 Review Cardiac Disease in Pregnancy Part 1 Congenitalsaeed hasan saeedNo ratings yet
- Venous Thrombosis and Embolism Prevention and ManagementDocument39 pagesVenous Thrombosis and Embolism Prevention and Managementsaeed hasan saeedNo ratings yet
- LCE Handbook 2018-19Document50 pagesLCE Handbook 2018-19saeed hasan saeedNo ratings yet
- Vaccination in Pregnancy Review Provides OverviewDocument7 pagesVaccination in Pregnancy Review Provides OverviewNoraNo ratings yet
- Pco With Eshre GLDocument21 pagesPco With Eshre GLsaeed hasan saeedNo ratings yet
- 15 ADocument9 pages15 ABrunoNo ratings yet
- P2 NCP 1Document4 pagesP2 NCP 1Kyle Albert EstoestaNo ratings yet
- Uncoordinated ContractionsDocument23 pagesUncoordinated ContractionsjoyceexallowNo ratings yet
- Lilac and Tan French Bulldog - Google SearchDocument1 pageLilac and Tan French Bulldog - Google SearchLyrics JuradoNo ratings yet
- Sexual Self JaylordDocument16 pagesSexual Self JaylordAko Si natoyNo ratings yet
- Importance of Sex EducationDocument6 pagesImportance of Sex EducationSristi ChNo ratings yet
- Pathophysiology of HysterectomyDocument5 pagesPathophysiology of HysterectomyJORINA PUMIHICNo ratings yet
- OvurelinDocument2 pagesOvurelinAndrew George GeorgeNo ratings yet
- E Learning NCM 107 NotesDocument47 pagesE Learning NCM 107 NotesSophia TomasNo ratings yet
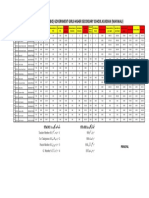
- Merit List Stis (Bio) Government Girls Higher Secondary School Kundian (Mianwali)Document1 pageMerit List Stis (Bio) Government Girls Higher Secondary School Kundian (Mianwali)Malik AsadNo ratings yet
- AHDP - Teenage Pregnancy NewDocument20 pagesAHDP - Teenage Pregnancy NewEdisa AsuncionNo ratings yet
- Cord Prolapse and Cord PresentationDocument21 pagesCord Prolapse and Cord PresentationKwizera virgileNo ratings yet
- GENSOC M2 Lesson 4Document7 pagesGENSOC M2 Lesson 4cassy margaNo ratings yet
- A Prelim CAMCARDocument18 pagesA Prelim CAMCARIvan VillapandoNo ratings yet
- Janimah DLLDocument3 pagesJanimah DLLعبد من عباد اللهNo ratings yet
- What Is The Process of Becoming A SurrogateDocument2 pagesWhat Is The Process of Becoming A SurrogateEva HospitalNo ratings yet
- Infertility Management in Women With PolycysticDocument7 pagesInfertility Management in Women With PolycysticCarolina SidabutarNo ratings yet
- Dissertation Questions On Teenage PregnancyDocument7 pagesDissertation Questions On Teenage PregnancyPayToDoMyPaperBatonRouge100% (1)
- Database of Questions For The Medical Final Examination (LEK) Obstetrics and GynecologyDocument87 pagesDatabase of Questions For The Medical Final Examination (LEK) Obstetrics and GynecologyAmalNo ratings yet
- Complications of Twin Pregnancy: by Harsh SharmaDocument19 pagesComplications of Twin Pregnancy: by Harsh SharmakushalNo ratings yet
- Lesson 11Document3 pagesLesson 11Jhoanna Rose AlingalanNo ratings yet
- Reproductive SystemDocument49 pagesReproductive SystemAyro Business CenterNo ratings yet
- 5 Reasons To Have Sex Even If You Don't Think You're in The MoodDocument11 pages5 Reasons To Have Sex Even If You Don't Think You're in The MoodBrian PierceNo ratings yet
- Ectopic PregnancyDocument10 pagesEctopic PregnancyRaquel MonsalveNo ratings yet
- Propose A Program in School or Community That Will Raise The Awareness of Students and Help Eliminate Sexually Transmitted Diseases Especially Among The YouthDocument2 pagesPropose A Program in School or Community That Will Raise The Awareness of Students and Help Eliminate Sexually Transmitted Diseases Especially Among The YouthDaziel ManaloNo ratings yet
- Shettles Method - WikipediaDocument3 pagesShettles Method - WikipediaYomiyu MNo ratings yet
- Biology Quarter 1 Unit 2 Day 7 Enrichment Escape Room PrintablesDocument4 pagesBiology Quarter 1 Unit 2 Day 7 Enrichment Escape Room PrintablesTeachTappyNo ratings yet
- Tugas KKPMT Pregnancy, Childbirth and The PuerperiumDocument3 pagesTugas KKPMT Pregnancy, Childbirth and The PuerperiumDyah CitraNo ratings yet
- Dogs BreedsDocument20 pagesDogs BreedsdonovanwickNo ratings yet
- Assess The Prevalence of Self Reported Vaginal Discharge, Perceived Causes and Associated Symptoms Among Reproductive Aged WomenDocument7 pagesAssess The Prevalence of Self Reported Vaginal Discharge, Perceived Causes and Associated Symptoms Among Reproductive Aged WomenEditor IJTSRDNo ratings yet
- Printed Pieces English Sba T DavyDocument7 pagesPrinted Pieces English Sba T DavyDAVYANAH WRIGHTNo ratings yet