You might also like
- National Immunization ScheduleDocument4 pagesNational Immunization ScheduleKenneth Ralph UrbanNo ratings yet
- National Immunization ScheduleDocument3 pagesNational Immunization SchedulescribdscribdtestNo ratings yet
- National Immunisation ProgrammeDocument2 pagesNational Immunisation ProgrammeAnonymous whcvnPBeQNo ratings yet
- Current UIP (Universal Immunization Programme) Schedule in Our StateDocument35 pagesCurrent UIP (Universal Immunization Programme) Schedule in Our StateGopireddy Sivakarthik ReddyNo ratings yet
- Universal Immunization ProgrammeDocument3 pagesUniversal Immunization ProgrammeAmy Lalringhluani ChhakchhuakNo ratings yet
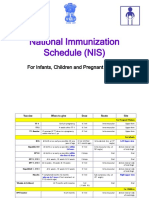
- National Immunization Schedule (NIS) For Infants, Children and Pregnant WomenDocument1 pageNational Immunization Schedule (NIS) For Infants, Children and Pregnant WomenShrinivas YuvanNo ratings yet
- National Immunization ScheduleDocument1 pageNational Immunization ScheduleSudheer100% (1)
- National - Immunization - Schedule PDFDocument3 pagesNational - Immunization - Schedule PDF80ALLA86iNo ratings yet
- Acute Respiratory InfectionDocument24 pagesAcute Respiratory Infectionsunma09082001No ratings yet
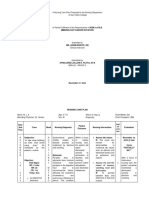
- Community Health Nursing: San Pedro College 12 C. Guzman Street, Davao City Toraja, Martina EDocument6 pagesCommunity Health Nursing: San Pedro College 12 C. Guzman Street, Davao City Toraja, Martina ECharlie AbagonNo ratings yet
- Handout - ADocument13 pagesHandout - AMadhu UpadhyayNo ratings yet
- National Immunization Schedule (NIS) : For Infants, Children and Pregnant WomenDocument13 pagesNational Immunization Schedule (NIS) : For Infants, Children and Pregnant WomenPrabir Kumar Chatterjee100% (1)
- Immunization-WPS OfficeDocument3 pagesImmunization-WPS OfficeFranc'isco ChidiebereNo ratings yet
- Immunization ComparisonDocument1 pageImmunization ComparisonNeil Dominic FernandesNo ratings yet
- Initial Patient Assessment in OpdDocument4 pagesInitial Patient Assessment in OpdLokender Goyal100% (1)
- Immunization ScheduleDocument18 pagesImmunization Scheduledr parveen bathlaNo ratings yet
- 2 ImmunizationsDocument2 pages2 ImmunizationsPHOEBE ANN ROCHENo ratings yet
- National Immunisation ScheduleDocument33 pagesNational Immunisation ScheduleVignesh ArumugamNo ratings yet
- Expanded Program On ImmunizationDocument9 pagesExpanded Program On ImmunizationJesena Salve100% (1)
- National Immunization Schedule & Faqs: DR Amita Raoot DFWDocument58 pagesNational Immunization Schedule & Faqs: DR Amita Raoot DFWamitaNo ratings yet
- ImmunizationDocument16 pagesImmunizationShikha Singh VermaNo ratings yet
- Immunization Clinic Report PDFDocument9 pagesImmunization Clinic Report PDFprabha krishnanNo ratings yet
- Enteric FeverDocument30 pagesEnteric FeverShivam MalikNo ratings yet
- IMUNISASI2Document29 pagesIMUNISASI2RatnaSuryatiNo ratings yet
- VACCINESDocument1 pageVACCINESNensu-chanNo ratings yet
- PEDIA Immunizations 2018Document4 pagesPEDIA Immunizations 2018Mary Christine IlangaNo ratings yet
- Routine ImmunizationDocument50 pagesRoutine ImmunizationA KokNo ratings yet
- IMMUNIZATION SCHEDULE NewDocument1 pageIMMUNIZATION SCHEDULE NewVaishali SinghNo ratings yet
- ImmunizationDocument1 pageImmunizationMicah Lou CalambaNo ratings yet
- Immunisation - NHMDocument2 pagesImmunisation - NHMindraseenayya chilakalaNo ratings yet
- Summarize Notes On ImciDocument6 pagesSummarize Notes On ImciI'm Just A BurgerNo ratings yet
- General Information:: Sta. Ana Hospital Department of Rehabilitation Medicine Physical Therapy SectionDocument13 pagesGeneral Information:: Sta. Ana Hospital Department of Rehabilitation Medicine Physical Therapy SectionOlenFuerteNo ratings yet
- Lesson8 Pediatric Health HistoryDocument9 pagesLesson8 Pediatric Health HistoryDennis Nabor Muñoz, RN,RM100% (1)
- Disorder S Tested For NewbornDocument8 pagesDisorder S Tested For NewbornKirsten KateNo ratings yet
- 3 Care PlanDocument25 pages3 Care PlanKhushbu KatariaNo ratings yet
- 12 - Bakuna Atbp.Document4 pages12 - Bakuna Atbp.gilbert agudoNo ratings yet
- Paediatrics - Arjuna 1.0 NEW 2Document9 pagesPaediatrics - Arjuna 1.0 NEW 2Ajay singhNo ratings yet
- Expanded Program of ImmunizationDocument20 pagesExpanded Program of ImmunizationgwynNo ratings yet
- EPI Schedule Malawi COM 2017Document2 pagesEPI Schedule Malawi COM 2017INNOCENT KHULIWANo ratings yet
- Routine Immunization National Immunization ScheduleDocument1 pageRoutine Immunization National Immunization ScheduleAshish GaurNo ratings yet
- Precept1 - Pulmo BlockDocument15 pagesPrecept1 - Pulmo BlockMary Christine IlangaNo ratings yet
- Expanded Immunization Program EpiDocument22 pagesExpanded Immunization Program EpiGirome BairaNo ratings yet
- Pulmonary EdemaDocument23 pagesPulmonary EdemaELISION OFFICIALNo ratings yet
- NP1 BulletsDocument17 pagesNP1 BulletsJea VesagasNo ratings yet
- NP1 BulletsDocument17 pagesNP1 BulletsJea VesagasNo ratings yet
- National Immunization Schedule: One Dose at 14 Weeks, Along With OPV3. Injectable Dose GivenDocument1 pageNational Immunization Schedule: One Dose at 14 Weeks, Along With OPV3. Injectable Dose GivenSandip PatilNo ratings yet
- Prescribing in ChildrenDocument4 pagesPrescribing in ChildrenArkopal GuptaNo ratings yet
- Each Province Immune ScheduleDocument2 pagesEach Province Immune ScheduleScribdNo ratings yet
- Vaccines of The National Immunization Program of TDocument7 pagesVaccines of The National Immunization Program of T1BSN04 DE GUZMAN, LEMARRY JOYCE V.No ratings yet
- CHN ReviewerDocument30 pagesCHN ReviewerKristian Del FierroNo ratings yet
- Essential Intrapartum Newborn CareDocument31 pagesEssential Intrapartum Newborn CareJohn Christopher LucesNo ratings yet
- Cnd. Epi Field Visit Report, April 2023. Sayah UpdatedDocument13 pagesCnd. Epi Field Visit Report, April 2023. Sayah UpdatedJel JohnNo ratings yet
- Week 8 NIPDocument25 pagesWeek 8 NIPBritney TamuraNo ratings yet
- Case 2Document19 pagesCase 2Aliyi MuktarNo ratings yet
- India EPI Factsheet 2023Document6 pagesIndia EPI Factsheet 2023Chetan SharmaNo ratings yet
- Pertinent Positive Pertinent Negative Weight Loss (41 KG To 37 KG in 1-2 Months) Productive Cough Double Vision Lymph Node Swelling Fatigue Bruising Syncope Body Tremors DyspneaDocument8 pagesPertinent Positive Pertinent Negative Weight Loss (41 KG To 37 KG in 1-2 Months) Productive Cough Double Vision Lymph Node Swelling Fatigue Bruising Syncope Body Tremors DyspneaMary Christine IlangaNo ratings yet
- F Pineda JhaymeeDocument29 pagesF Pineda JhaymeeJhaymee PinedaNo ratings yet
- TubercolosisDocument31 pagesTubercolosisibrahimNo ratings yet
- The Wonder of Probiotics: A 30-Day Plan to Boost Energy, Enhance Weight Loss, Heal GI Problems, Prevent Disease, and Slow AgingFrom EverandThe Wonder of Probiotics: A 30-Day Plan to Boost Energy, Enhance Weight Loss, Heal GI Problems, Prevent Disease, and Slow AgingNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 5: GastrointestinalFrom EverandComplementary and Alternative Medical Lab Testing Part 5: GastrointestinalNo ratings yet
- S - "Sakit Ahong Tinahian" As Verbalized byDocument6 pagesS - "Sakit Ahong Tinahian" As Verbalized bylandilinoNo ratings yet
- BRY's Microbiology, 1st SemesterDocument95 pagesBRY's Microbiology, 1st SemesterSaima ZuberiNo ratings yet
- Aranas - Geriatric Assessment ToolDocument14 pagesAranas - Geriatric Assessment ToolNicko Pazon AranasNo ratings yet
- Adam Nursing 111 Evaluation ToolDocument6 pagesAdam Nursing 111 Evaluation Toolapi-281282134No ratings yet
- AngioedemaDocument15 pagesAngioedemaYuni IHNo ratings yet
- The Relevance of Attachment Theory For PDocument52 pagesThe Relevance of Attachment Theory For PVeera Balaji KumarNo ratings yet
- C. Pasternatsky Symptom IsDocument11 pagesC. Pasternatsky Symptom IsareenNo ratings yet
- In Favour of An Investigation of The Relationship Between Vitamin B12 Deficiency and HIV InfectionDocument3 pagesIn Favour of An Investigation of The Relationship Between Vitamin B12 Deficiency and HIV InfectionPJ 123No ratings yet
- NCP - IleusDocument7 pagesNCP - IleusJullian PloyaNo ratings yet
- Periodontitis: Foreign-Body ReactionsDocument25 pagesPeriodontitis: Foreign-Body ReactionsAisyah Arina NurhafizahNo ratings yet
- Journal Reading: Imaging of Intracranial HemorrhageDocument27 pagesJournal Reading: Imaging of Intracranial HemorrhagehasrilNo ratings yet
- Glaukoma - PPTX KoassDocument38 pagesGlaukoma - PPTX Koassdhita01No ratings yet
- Body Fluids and Circulation Class 11 Study Notes: BloodDocument7 pagesBody Fluids and Circulation Class 11 Study Notes: BloodTUSHAR DASHNo ratings yet
- APA Guidelines On The Prevention of Postoperative Vomiting in ChildrenDocument35 pagesAPA Guidelines On The Prevention of Postoperative Vomiting in ChildrenMaria Lucia RossiNo ratings yet
- Gonadal enDocument60 pagesGonadal enm7md TotiaNo ratings yet
- Management of Patients With Upper Respiratory Tract DisordersDocument93 pagesManagement of Patients With Upper Respiratory Tract DisordersErica Clerigo LandichoNo ratings yet
- Medicaid Family TherapyDocument685 pagesMedicaid Family TherapyfejjinsNo ratings yet
- Gauze-Based Negative Pressure Wound TherapyDocument20 pagesGauze-Based Negative Pressure Wound TherapyAbdilla RidhwanNo ratings yet
- Septic ShockDocument26 pagesSeptic ShockIma SoniaNo ratings yet
- Acupuntura - Puntos ImportantesDocument14 pagesAcupuntura - Puntos ImportantessanthigiNo ratings yet
- QRG Morpheus8 ROW February 2021docx (Appl)Document2 pagesQRG Morpheus8 ROW February 2021docx (Appl)JW100% (3)
- NCM 104 IG Lec - DOC CARLDocument23 pagesNCM 104 IG Lec - DOC CARLLanz LlnsNo ratings yet
- Gastro POMDocument63 pagesGastro POMLionell Castillo100% (1)
- Medical Terminology Chapter 3Document5 pagesMedical Terminology Chapter 3Gregg ProducerNo ratings yet
- Irna - Existing RS Type DDocument17 pagesIrna - Existing RS Type DUcrit TralalaNo ratings yet
- Core Knowledge OrthopaedicsDocument2 pagesCore Knowledge OrthopaedicsIamTineshNo ratings yet
- Zhang2020 Article EvaluationOfBepanGelHydrogelEfDocument14 pagesZhang2020 Article EvaluationOfBepanGelHydrogelEfİncelus ChinusNo ratings yet
- Foundations Adult Health Nursing 8th Cooper Test BankDocument15 pagesFoundations Adult Health Nursing 8th Cooper Test BankRaadqqqNo ratings yet
- Dexmedetomidine - Drug Information - UpToDateDocument21 pagesDexmedetomidine - Drug Information - UpToDateRicardo Ortiz NovilloNo ratings yet
- Insulin Pumps and Sensors Cox PDFDocument42 pagesInsulin Pumps and Sensors Cox PDFDevang SNo ratings yet