You might also like
- Management of Hemostasis and Coagulopathies for Surgical and Critically Ill Patients: An Evidence-Based ApproachFrom EverandManagement of Hemostasis and Coagulopathies for Surgical and Critically Ill Patients: An Evidence-Based ApproachRating: 5 out of 5 stars5/5 (1)
- Contrasting Time - and Rate-Based Approaches For The Assessment of Drug-Induced QT ChangesDocument10 pagesContrasting Time - and Rate-Based Approaches For The Assessment of Drug-Induced QT ChangesLuciana OliveiraNo ratings yet
- Renal Pharmacotherapy: Dosage Adjustment of Medications Eliminated by the KidneysFrom EverandRenal Pharmacotherapy: Dosage Adjustment of Medications Eliminated by the KidneysNo ratings yet
- Chronic Kidney Disease and Statin Therapy: To Treat or Not To Treat?Document3 pagesChronic Kidney Disease and Statin Therapy: To Treat or Not To Treat?adilNo ratings yet
- The Evolution of Radionanotargeting towards Clinical Precision Oncology: A Festschrift in Honor of Kalevi KairemoFrom EverandThe Evolution of Radionanotargeting towards Clinical Precision Oncology: A Festschrift in Honor of Kalevi KairemoNo ratings yet
- Pharmacotherapy - 2022 - Skersick - Evaluating The Evidence For Sacubitril Valsartan Across The Continuum of Heart FailureDocument12 pagesPharmacotherapy - 2022 - Skersick - Evaluating The Evidence For Sacubitril Valsartan Across The Continuum of Heart FailureJ MrNo ratings yet
- Personalised Human Albumin in Patients With Cirrhosis and Ascites: Design and Rationale For The ALB-TRIAL - A Randomised Clinical Biomarker Validation TrialDocument8 pagesPersonalised Human Albumin in Patients With Cirrhosis and Ascites: Design and Rationale For The ALB-TRIAL - A Randomised Clinical Biomarker Validation Trialstardust.m002No ratings yet
- AC After StrokeDocument6 pagesAC After StrokeDileepa chathurangaNo ratings yet
- Katayama Et Al 2016 Factors Predicting Successful Discontinuation of Continuous Renal Replacement TherapyDocument5 pagesKatayama Et Al 2016 Factors Predicting Successful Discontinuation of Continuous Renal Replacement Therapypj rakNo ratings yet
- 1 s2.0 S1071916423003068 MainDocument13 pages1 s2.0 S1071916423003068 Mainevelyn.minichNo ratings yet
- Kidney News Article p20 7Document2 pagesKidney News Article p20 7ilgarciaNo ratings yet
- Noacs: An Emerging Class of Oral Anticoagulants-A Review ArticleDocument7 pagesNoacs: An Emerging Class of Oral Anticoagulants-A Review ArticleYohanes SutejaNo ratings yet
- J Jacc 2022 08 737Document13 pagesJ Jacc 2022 08 737kevin ortegaNo ratings yet
- Perioperative Use Anticoagulant-2016Document12 pagesPerioperative Use Anticoagulant-2016catalinguraanNo ratings yet
- Direct Oral Anticoagulants in Treatment of Cerebral Venous Thrombosis: A Systematic Review ProtocolDocument4 pagesDirect Oral Anticoagulants in Treatment of Cerebral Venous Thrombosis: A Systematic Review Protocolrachman puteraNo ratings yet
- E050067 FullDocument5 pagesE050067 FullAya ZemaliNo ratings yet
- Initiation, Continuation, Switching, and Withdrawal of Heart Failure Medical Therapies During HospitalizationDocument11 pagesInitiation, Continuation, Switching, and Withdrawal of Heart Failure Medical Therapies During HospitalizationAshutosh SinghNo ratings yet
- S126 FullDocument12 pagesS126 FullIago CarvalhoNo ratings yet
- Clinical Outcomes Related To Background Diuretic Use and New Diuretic Initiation in Patients With HfrefDocument13 pagesClinical Outcomes Related To Background Diuretic Use and New Diuretic Initiation in Patients With HfrefImaNo ratings yet
- Accelerated and Personalized Therapy For Heart Failure With Reduced Ejection FractionDocument15 pagesAccelerated and Personalized Therapy For Heart Failure With Reduced Ejection FractiondrguillermomoNo ratings yet
- NOCS European GuidelinesDocument27 pagesNOCS European Guidelinesdragon66No ratings yet
- J Jcin 2023 01 366Document15 pagesJ Jcin 2023 01 366Kardiologi ManadoNo ratings yet
- 1 s2.0 S0104001421001378 MainDocument14 pages1 s2.0 S0104001421001378 MainSantanico De CVT deozaNo ratings yet
- Peripocedural Anticoagulation LPDocument11 pagesPeripocedural Anticoagulation LPlauraalvisNo ratings yet
- A Meta-Analysis of Andexanet Alfa and ProthrombinDocument14 pagesA Meta-Analysis of Andexanet Alfa and ProthrombinLuan FerreiraNo ratings yet
- Bivalirudin Anticoagulant1Document6 pagesBivalirudin Anticoagulant1walid hassanNo ratings yet
- European J of Heart Fail - 2021 - Greene - Another Reason To Embrace Quadruple Medical Therapy For Heart FailureDocument4 pagesEuropean J of Heart Fail - 2021 - Greene - Another Reason To Embrace Quadruple Medical Therapy For Heart FailureSrinivas PingaliNo ratings yet
- When To Discontinue Renal Replacement TherapyDocument7 pagesWhen To Discontinue Renal Replacement Therapyvali.levo7No ratings yet
- Doacs in Patients With Mitral Stenosis and Atrial FibrillationDocument3 pagesDoacs in Patients With Mitral Stenosis and Atrial FibrillationNasriNo ratings yet
- Practneurol 2017 001820.fullDocument11 pagesPractneurol 2017 001820.fullIniya RajendranNo ratings yet
- Captura de Pantalla 2022-08-15 A La(s) 17.37.40 PDFDocument11 pagesCaptura de Pantalla 2022-08-15 A La(s) 17.37.40 PDFMatias PadillaNo ratings yet
- Impact of Optimal Medical Therapy On 10-Year Mortality After Coronary RevascularizationDocument12 pagesImpact of Optimal Medical Therapy On 10-Year Mortality After Coronary RevascularizationsarahNo ratings yet
- CVS Toxicity Anticancer Systematic ReviewDocument15 pagesCVS Toxicity Anticancer Systematic ReviewprasanbhandariNo ratings yet
- DAPTDocument12 pagesDAPTPedro JalladNo ratings yet
- RRT in Icu1 Spain PDFDocument13 pagesRRT in Icu1 Spain PDFrajkumarss87No ratings yet
- European J of Heart Fail - 2018 - Mullens - Rationale and Design of The ADVOR Acetazolamide in Decompensated Heart FailureDocument10 pagesEuropean J of Heart Fail - 2018 - Mullens - Rationale and Design of The ADVOR Acetazolamide in Decompensated Heart FailureAnnisa Tria FadillaNo ratings yet
- Artikel 1, A Comparative Post Hoc Analysis of Finerenone and Spironolactone in Resistant Hypertension in Moderate-To-Advanced Chronic Kidney DiseaseDocument10 pagesArtikel 1, A Comparative Post Hoc Analysis of Finerenone and Spironolactone in Resistant Hypertension in Moderate-To-Advanced Chronic Kidney DiseaseDandung RuskarNo ratings yet
- Insuficiencia Cardiaca HidratactionDocument5 pagesInsuficiencia Cardiaca Hidratactiongustavo reyesNo ratings yet
- Continuous Versus Intermittent Administration of Furosemide in AcuteDocument9 pagesContinuous Versus Intermittent Administration of Furosemide in AcuteDenisseRangelNo ratings yet
- Ejhf.927 CRT in PracticeDocument4 pagesEjhf.927 CRT in PracticeCorina DiaconescuNo ratings yet
- Pancreatic SurgeryDocument5 pagesPancreatic SurgeryFlaviu Ionuț FaurNo ratings yet
- Nef DiscRAADocument11 pagesNef DiscRAAGabriela PachecoNo ratings yet
- QT SyndromeDocument7 pagesQT SyndromeRikhardo RkNo ratings yet
- Fabes Et Al 2023 Goal Directed Haemodynamic Therapy Improves Patient Outcomes in Kidney TransplantationDocument6 pagesFabes Et Al 2023 Goal Directed Haemodynamic Therapy Improves Patient Outcomes in Kidney TransplantationJossy MarinesNo ratings yet
- The Barrow Ruptured Aneurysm Trial - 6-Year ResultsDocument9 pagesThe Barrow Ruptured Aneurysm Trial - 6-Year ResultsJulieta PereyraNo ratings yet
- 2.impact of A Pharmaceutical Care Service For Patients With Rheumatoid Arthritis Using A Customised Mobile Device (The PROUD Trial) Study Protocol For A Randomised Controlled TrialDocument8 pages2.impact of A Pharmaceutical Care Service For Patients With Rheumatoid Arthritis Using A Customised Mobile Device (The PROUD Trial) Study Protocol For A Randomised Controlled TrialGungunn bainiamNo ratings yet
- Nihms 1028632Document23 pagesNihms 1028632Halim MusahibNo ratings yet
- Medicine: Cardioprotective Effect of Histamine H2 Antagonists in Congestive Heart FailureDocument10 pagesMedicine: Cardioprotective Effect of Histamine H2 Antagonists in Congestive Heart Failureerni pabateNo ratings yet
- Jos 2015 01655Document14 pagesJos 2015 01655Arvin Anwar SamanteNo ratings yet
- Laboratory QADocument8 pagesLaboratory QAAnkush SinghalNo ratings yet
- Algoritmo Fallo Renal 2009Document10 pagesAlgoritmo Fallo Renal 2009JoseBustamanteRuizNo ratings yet
- Indikasi TrombektomiDocument6 pagesIndikasi TrombektomiNatasha BastiaanNo ratings yet
- Doacs AND LABORATORY1Document12 pagesDoacs AND LABORATORY1pasqualijNo ratings yet
- K Binders MADocument12 pagesK Binders MADouglas Mesadri GewehrNo ratings yet
- Auricchio & Cols. (1999)Document6 pagesAuricchio & Cols. (1999)Luba D'AndreaNo ratings yet
- Pioneering The In-Hospital Initiation of Sacubitril-ValsartanDocument2 pagesPioneering The In-Hospital Initiation of Sacubitril-ValsartanCarlos LlanosNo ratings yet
- Fluid Balance and Renal Replacement Therapy Initiation Strategy: A Secondary Analysis of The STARRT-AKI TrialDocument11 pagesFluid Balance and Renal Replacement Therapy Initiation Strategy: A Secondary Analysis of The STARRT-AKI Trialnina2911No ratings yet
- ESCAPE Study - JAMA 2005Document9 pagesESCAPE Study - JAMA 2005MICHAEL AMARILLO CORREANo ratings yet
- Fernandez-Fuertes J. 2022. Clinical Response OA Standardized Closed System Low Cost PRP ProductDocument11 pagesFernandez-Fuertes J. 2022. Clinical Response OA Standardized Closed System Low Cost PRP ProductJavier MartinNo ratings yet
- Impact of A Pharmaceutical Care Service For Patients With Rheumatoid Arthritis Using A Customised Mobile Device The PROUD Trial Study Protocol For A Randomised Controlled Trial - TEM HTMLDocument8 pagesImpact of A Pharmaceutical Care Service For Patients With Rheumatoid Arthritis Using A Customised Mobile Device The PROUD Trial Study Protocol For A Randomised Controlled Trial - TEM HTMLAline Leal CortesNo ratings yet
- Prospective Evaluation of Parent and Child Outcomes Following Admission To A Virtual' Early Parenting Residential ProgrammeDocument10 pagesProspective Evaluation of Parent and Child Outcomes Following Admission To A Virtual' Early Parenting Residential Programmestardust.m002No ratings yet
- Integrating Artificial Intelligence Into Lung Cancer Screening: A Randomised Controlled Trial ProtocolDocument6 pagesIntegrating Artificial Intelligence Into Lung Cancer Screening: A Randomised Controlled Trial Protocolstardust.m002No ratings yet
- Compliance of Adolescent Friendly Health Clinics With National and International Standards: Quantitative Findings From The I-Saathiya StudyDocument11 pagesCompliance of Adolescent Friendly Health Clinics With National and International Standards: Quantitative Findings From The I-Saathiya Studystardust.m002No ratings yet
- How Do Sepsis Survivors Experience Life After Sepsis? A Danish Qualitative Study Exploring Factors of ImportanceDocument7 pagesHow Do Sepsis Survivors Experience Life After Sepsis? A Danish Qualitative Study Exploring Factors of Importancestardust.m002No ratings yet
- Experiences With Neonatal Jaundice Management in Hospitals and The Community: Interviews With Australian Health ProfessionalsDocument9 pagesExperiences With Neonatal Jaundice Management in Hospitals and The Community: Interviews With Australian Health Professionalsstardust.m002No ratings yet
- Social Media and Postsecondary Student Adoption of Mental Health Labels: Protocol For A Scoping ReviewDocument5 pagesSocial Media and Postsecondary Student Adoption of Mental Health Labels: Protocol For A Scoping Reviewstardust.m002No ratings yet
- Teaching and Learning Techniques For The Online Environment. How To Maintain Students' Attention and Achieve Learning Outcomes in A Virtual Environment Using New TechnologyDocument13 pagesTeaching and Learning Techniques For The Online Environment. How To Maintain Students' Attention and Achieve Learning Outcomes in A Virtual Environment Using New Technologystardust.m002No ratings yet
- Investigating Experiences of People With Advanced Breast or Lung Cancer in Their Natural Context: Protocol For An Experience Sampling StudyDocument12 pagesInvestigating Experiences of People With Advanced Breast or Lung Cancer in Their Natural Context: Protocol For An Experience Sampling Studystardust.m002No ratings yet
- Women's Perceptions and Attitudes Towards The Use of AI in Mammography in Sweden: A Qualitative Interview StudyDocument10 pagesWomen's Perceptions and Attitudes Towards The Use of AI in Mammography in Sweden: A Qualitative Interview Studystardust.m002No ratings yet
- MifepristoneDocument1 pageMifepristonejennierubyjane kimNo ratings yet
- Kalbe Farma, TBK (Optima) UPDATE JULI 2023 - 1Document12 pagesKalbe Farma, TBK (Optima) UPDATE JULI 2023 - 1ekaputraantoNo ratings yet
- Comparison Between Efficacy of Melatonin and Diazepam For Prevention of Recurrent Simple Febrile Seizures A Randomized Clinical TrialDocument6 pagesComparison Between Efficacy of Melatonin and Diazepam For Prevention of Recurrent Simple Febrile Seizures A Randomized Clinical TrialalasNo ratings yet
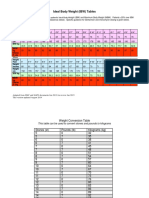
- IBW TableDocument2 pagesIBW TablegrafikeyesNo ratings yet
- Adrenergic Receptor ChartDocument1 pageAdrenergic Receptor ChartAnkit Mehta75% (4)
- Drugs Associated With Tinnitus 2013Document28 pagesDrugs Associated With Tinnitus 2013DownTheTheRabbitHole108No ratings yet
- Case Report Tinea Corporis - Salsabilla Sahara - 22004101052Document25 pagesCase Report Tinea Corporis - Salsabilla Sahara - 22004101052Salsabilla SaharaNo ratings yet
- Therapeutic Drug Monitoring: T H e R A P e U T I C T o X I CDocument22 pagesTherapeutic Drug Monitoring: T H e R A P e U T I C T o X I Ckavya nainitaNo ratings yet
- Pho Meds ListDocument1 pagePho Meds Listmister emdiNo ratings yet
- Foundations Ati QuizletDocument5 pagesFoundations Ati QuizletsaraNo ratings yet
- Anti-Viral Drugs1Document38 pagesAnti-Viral Drugs1Curex QANo ratings yet
- Aims Email Ids - DoctorsDocument10 pagesAims Email Ids - DoctorsKunwar SaigalNo ratings yet
- ATB and Combined PillDocument8 pagesATB and Combined PillDaniela SimõesNo ratings yet
- Tablet SIBDocument45 pagesTablet SIBMd Sayeed100% (1)
- 2019 PPhA NatCon Program Overview (05-Apr-2019)Document5 pages2019 PPhA NatCon Program Overview (05-Apr-2019)Tondo PharmNo ratings yet
- Categorize The Treatment Options For Patients With Existing Medical ConditionDocument3 pagesCategorize The Treatment Options For Patients With Existing Medical ConditionMicah LatosaNo ratings yet
- Pharmacology For Oral RecitDocument16 pagesPharmacology For Oral RecitAngel DiangNo ratings yet
- Treatment ProtocolDocument3 pagesTreatment ProtocolFabio CoelhoNo ratings yet
- Lista de Precios CefarmaDocument54 pagesLista de Precios CefarmaAlicia OrtizNo ratings yet
- Chemistry in Everyday LifeDocument71 pagesChemistry in Everyday LifePratima SinghNo ratings yet
- Rajini Final Merged ThesisDocument89 pagesRajini Final Merged ThesispadminiNo ratings yet
- Bronchodilators and Other Respiratory AgentsDocument46 pagesBronchodilators and Other Respiratory AgentsElthon John BueNo ratings yet
- The Use of Burst Ketamin in Refracter Cancer PainDocument6 pagesThe Use of Burst Ketamin in Refracter Cancer PainInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Implementation of Pharmacogenomics Testing in Shoppers Drug Mart #976Document54 pagesImplementation of Pharmacogenomics Testing in Shoppers Drug Mart #976eishavjNo ratings yet
- Paracetamol Toxicity Inacat: Case ReportDocument3 pagesParacetamol Toxicity Inacat: Case ReportValen BarreroNo ratings yet
- Aspartame Studies Correlation Outcome Funding Sources PDFDocument18 pagesAspartame Studies Correlation Outcome Funding Sources PDFportosinNo ratings yet
- Arrhythmia 6 YrDocument72 pagesArrhythmia 6 YrPiyush MalikNo ratings yet
- Management of HypokalemiaDocument6 pagesManagement of HypokalemiaEsraa Abu elelaNo ratings yet
- Calculation of Oral and Parenteral DosesDocument10 pagesCalculation of Oral and Parenteral DosesHilary LaneNo ratings yet
- DopamineDocument9 pagesDopamineBaby Lyn Ann TanalgoNo ratings yet
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDFrom EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDRating: 5 out of 5 stars5/5 (5)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (404)
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)From EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Rating: 3 out of 5 stars3/5 (1)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 4.5 out of 5 stars4.5/5 (84)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- The Twentysomething Treatment: A Revolutionary Remedy for an Uncertain AgeFrom EverandThe Twentysomething Treatment: A Revolutionary Remedy for an Uncertain AgeRating: 5 out of 5 stars5/5 (4)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (40)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 4 out of 5 stars4/5 (6)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (267)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 4 out of 5 stars4/5 (5)
- I Shouldn't Feel This Way: Name What’s Hard, Tame Your Guilt, and Transform Self-Sabotage into Brave ActionFrom EverandI Shouldn't Feel This Way: Name What’s Hard, Tame Your Guilt, and Transform Self-Sabotage into Brave ActionNo ratings yet
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (44)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeRating: 2 out of 5 stars2/5 (1)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (170)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (46)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisFrom EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (4)
- To Explain the World: The Discovery of Modern ScienceFrom EverandTo Explain the World: The Discovery of Modern ScienceRating: 3.5 out of 5 stars3.5/5 (51)
- Manipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesFrom EverandManipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesRating: 4.5 out of 5 stars4.5/5 (1412)
- Self-Care for Autistic People: 100+ Ways to Recharge, De-Stress, and Unmask!From EverandSelf-Care for Autistic People: 100+ Ways to Recharge, De-Stress, and Unmask!Rating: 5 out of 5 stars5/5 (1)