You might also like
- Policy and Procedures For Hiring, PromotionsDocument2 pagesPolicy and Procedures For Hiring, PromotionsRazel Ann ElagioNo ratings yet
- 1103-1104 RepairDocument120 pages1103-1104 RepairCristobal Sanchez91% (23)
- Pathophysiology of Cardiogenic Pulmonary EdemaDocument8 pagesPathophysiology of Cardiogenic Pulmonary EdemaLili Fiorela CRNo ratings yet
- Sample Project ReportDocument24 pagesSample Project ReportPariniti Gupta100% (1)
- Boq Floor Tiling WorksDocument1 pageBoq Floor Tiling WorksISAAC KIPSEREM0% (2)
- (Nikolaj Wolfson, Alexander Lerner, Leonid Roshal (B-Ok - CC)Document589 pages(Nikolaj Wolfson, Alexander Lerner, Leonid Roshal (B-Ok - CC)Andi sutandi100% (1)
- Overview of Hypertension in Acute and Chronic Kidney Disease - UpToDateDocument8 pagesOverview of Hypertension in Acute and Chronic Kidney Disease - UpToDateNiñoTanNo ratings yet
- Hypertension in Dialysis PatientsDocument16 pagesHypertension in Dialysis PatientsLiliana WoodNo ratings yet
- Malignant Hypertension: Hypertensive EmergenciesDocument7 pagesMalignant Hypertension: Hypertensive EmergenciesAbdul QuyyumNo ratings yet
- Treatment of Acute Decompensated Heart Failure - Components of TherapyDocument22 pagesTreatment of Acute Decompensated Heart Failure - Components of TherapyYahaira Borquez RiosNo ratings yet
- Insufic Cardiaca 1Document13 pagesInsufic Cardiaca 1Ronaldo DuarteNo ratings yet
- Cardiorenal SyndromeDocument18 pagesCardiorenal SyndromefelipetheNo ratings yet
- Clinical Manifestations and Diagnosis of Advanced Heart Failure - UpToDateDocument17 pagesClinical Manifestations and Diagnosis of Advanced Heart Failure - UpToDatearturitouNo ratings yet
- HypertensionDocument14 pagesHypertensionDavid HosamNo ratings yet
- Falla Cardiaca ReviewDocument9 pagesFalla Cardiaca ReviewYasmin CarhuamacaNo ratings yet
- A Patient With Uncontrolled Hypertension: Case DiscussionDocument2 pagesA Patient With Uncontrolled Hypertension: Case DiscussionkeboooooNo ratings yet
- Causes: Hypertension, Also Referred To As High Blood Pressure, HTN or HPN, Is A Medical Condition inDocument8 pagesCauses: Hypertension, Also Referred To As High Blood Pressure, HTN or HPN, Is A Medical Condition inChristine Karen BelgaNo ratings yet
- Cardiorenal Syndrome: Definition, Prevalence, Diagnosis, and Pa Tho PhysiologyDocument10 pagesCardiorenal Syndrome: Definition, Prevalence, Diagnosis, and Pa Tho PhysiologySimone AquinoNo ratings yet
- Interactions of The Heart and The LiverDocument11 pagesInteractions of The Heart and The LiverRahmatika LestariNo ratings yet
- Need To Know: Isolated Systolic Hypertension: AnemiaDocument8 pagesNeed To Know: Isolated Systolic Hypertension: Anemiaemlyn_lanonNo ratings yet
- Cardiorenal Syndrome: Definition, Prevalence, Diagnosis, and PathophysiologyDocument14 pagesCardiorenal Syndrome: Definition, Prevalence, Diagnosis, and PathophysiologyOlga BabiiNo ratings yet
- Clinical Manifestations and Diagnosis of Advanced Heart FailureDocument11 pagesClinical Manifestations and Diagnosis of Advanced Heart FailureJorge Silva MineiroNo ratings yet
- Abhay KumarDocument3 pagesAbhay KumarDr. Jatin GargNo ratings yet
- NIH Public Access: Author ManuscriptDocument24 pagesNIH Public Access: Author ManuscriptMusyawarah MelalaNo ratings yet
- Cardiovascular Effects of HypertensionDocument12 pagesCardiovascular Effects of HypertensionEdwin F. Freecss WoworNo ratings yet
- Perioperative ManagmentDocument9 pagesPerioperative ManagmentPrabhat KcNo ratings yet
- Stenoza AorticaDocument31 pagesStenoza Aorticamicaella07No ratings yet
- Predictors of Survival in Heart Failure With Reduced Ejection Fraction - UpToDateDocument48 pagesPredictors of Survival in Heart Failure With Reduced Ejection Fraction - UpToDatesamNo ratings yet
- Therapeutic Options For The Management of The Cardiorenal SyndromeDocument11 pagesTherapeutic Options For The Management of The Cardiorenal SyndromeAntoine SchallerNo ratings yet
- Hepatorenal Syndrome - UpToDateDocument26 pagesHepatorenal Syndrome - UpToDateAssault AmphibiansNo ratings yet
- Manejo de La Insufiencia Cardica HtaDocument10 pagesManejo de La Insufiencia Cardica HtaNeiny FonsecaNo ratings yet
- Hypertension UrgencyDocument17 pagesHypertension UrgencyLeoNo ratings yet
- Cardiorenal Syndrome Definition, Prevalence, Diagnosis, and PathophysiologyDocument17 pagesCardiorenal Syndrome Definition, Prevalence, Diagnosis, and PathophysiologyRafael Vieira lealNo ratings yet
- Clinical Manifestations and Diagnosis of Edema in AdultsDocument7 pagesClinical Manifestations and Diagnosis of Edema in AdultsOscar Castro CuaquiraNo ratings yet
- Hypertension: Hypertension Is One of The Most Common Worldwide Diseases Afflicting Humans. BecauseDocument8 pagesHypertension: Hypertension Is One of The Most Common Worldwide Diseases Afflicting Humans. BecauseKramojNo ratings yet
- Jurnal Anes 1Document7 pagesJurnal Anes 1Chanvira Aria CandrayanaNo ratings yet
- Medical Management in Patients With Renovascular Hypertension 2013Document8 pagesMedical Management in Patients With Renovascular Hypertension 2013hmqNo ratings yet
- Clinical Manifestations and Evaluation of The Patient With Suspected Heart Failure PDFDocument23 pagesClinical Manifestations and Evaluation of The Patient With Suspected Heart Failure PDFcristianamihailaNo ratings yet
- Koniari 2011Document11 pagesKoniari 2011rosyidmawardi7No ratings yet
- Hypertension Management 2009Document6 pagesHypertension Management 2009Samnai RifaiNo ratings yet
- La VidaDocument16 pagesLa Vidajulio alonsoNo ratings yet
- Uncontrolled Blood PressureDocument6 pagesUncontrolled Blood PressureFika SilviaNo ratings yet
- Hypertension: Signs and SymptomsDocument7 pagesHypertension: Signs and SymptomsAdinia NugrahiniNo ratings yet
- Valsartan in The Treatment of Hypertension: OriginalDocument4 pagesValsartan in The Treatment of Hypertension: Originaldini hanifaNo ratings yet
- Pi Is 1499267113000373 ObatDocument3 pagesPi Is 1499267113000373 Obatscd_chesa_189432221No ratings yet
- Hepatorenal Syndrome - Introduction and DiagnosisDocument38 pagesHepatorenal Syndrome - Introduction and DiagnosisbornflaxNo ratings yet
- Acute Liver Failure in Adults - Management and Prognosis - UpToDateDocument36 pagesAcute Liver Failure in Adults - Management and Prognosis - UpToDateandus007No ratings yet
- HypertensionDocument8 pagesHypertensionsalahoveNo ratings yet
- ADHF Up To DateDocument25 pagesADHF Up To DateAndreas Agung KurniawanNo ratings yet
- Jcom Feb10 HypertensionDocument9 pagesJcom Feb10 HypertensionrchristevenNo ratings yet
- Ischemic Hepatitis, Hepatic Infarction, and Ischemic Cholangiopathy - UpToDateDocument9 pagesIschemic Hepatitis, Hepatic Infarction, and Ischemic Cholangiopathy - UpToDateAmirhossein MemariNo ratings yet
- HDA UPTODATE Approach To Acute Upper Gastrointestinal Bleeding in AdultsDocument12 pagesHDA UPTODATE Approach To Acute Upper Gastrointestinal Bleeding in AdultsLeoberto Batista Pereira SobrinhoNo ratings yet
- RENAL UNIT ReadingsDocument4 pagesRENAL UNIT Readingsrichelle cortesNo ratings yet
- تقرير ضغط الدمDocument10 pagesتقرير ضغط الدمlyh355754No ratings yet
- Overview of Hypertension in AdultsDocument27 pagesOverview of Hypertension in AdultsMedByteNo ratings yet
- Previous Sectionnext SectionDocument19 pagesPrevious Sectionnext Sectionbaiq_permataNo ratings yet
- Peer Review Process: Authors: Section Editors: Deputy EditorDocument32 pagesPeer Review Process: Authors: Section Editors: Deputy EditorCarolina CardozoNo ratings yet
- Gi BleedingDocument22 pagesGi BleedingAndreea GociuNo ratings yet
- Hepatorenal Syndrome - UpToDateDocument38 pagesHepatorenal Syndrome - UpToDateSantiago IllarramendiNo ratings yet
- Control of Hypertension in The Critically Ill: A Pathophysiological ApproachDocument13 pagesControl of Hypertension in The Critically Ill: A Pathophysiological Approachjose torresNo ratings yet
- Acute Kidney Injury - Cardiorenal Syndromes (Acute Decompensated Heart Failure and Worsening Renal Function) - Renal and Urology NewsDocument25 pagesAcute Kidney Injury - Cardiorenal Syndromes (Acute Decompensated Heart Failure and Worsening Renal Function) - Renal and Urology Newsrr_eeyNo ratings yet
- Hypertensive CrisisDocument13 pagesHypertensive Crisis.Katherine CalderonNo ratings yet
- Evaluation and Treatment of Hypertensive Emergencies in Adults - UpToDateDocument13 pagesEvaluation and Treatment of Hypertensive Emergencies in Adults - UpToDaterolland_arrizaNo ratings yet
- Portal Hypertension, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandPortal Hypertension, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Comparative Study For Determination of Atracurium Besilate in Presence of Its Toxic Degradant (Laudanosine) by Reversed Phase HPLC and by TLC DensitometryDocument11 pagesComparative Study For Determination of Atracurium Besilate in Presence of Its Toxic Degradant (Laudanosine) by Reversed Phase HPLC and by TLC DensitometrySabrina JonesNo ratings yet
- Mini Dental ImplantsDocument11 pagesMini Dental ImplantsDario PuljićNo ratings yet
- PERDEV FIRST Periodical Test (2022)Document5 pagesPERDEV FIRST Periodical Test (2022)jeadryl LinatocNo ratings yet
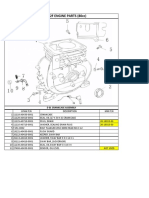
- Lifan 152F Engine Parts (80Cc) : E 01 Crankcase AssemblyDocument13 pagesLifan 152F Engine Parts (80Cc) : E 01 Crankcase AssemblySean MurrayNo ratings yet
- Sample CV Format (JIMS FORMAT)Document3 pagesSample CV Format (JIMS FORMAT)Elay PedrosoNo ratings yet
- 150.66-RP4 YcalDocument92 pages150.66-RP4 YcalJosé RamosNo ratings yet
- Grandma StoriesDocument38 pagesGrandma StoriesSita Rani Devi DasiNo ratings yet
- 6 Ijasrjun20196Document8 pages6 Ijasrjun20196TJPRC PublicationsNo ratings yet
- E 23 Fuel System Schaffer 4350ZDocument3 pagesE 23 Fuel System Schaffer 4350ZSergeyNo ratings yet
- Book Review - Black Skin, White MasksDocument9 pagesBook Review - Black Skin, White MasksKaren A. LloydNo ratings yet
- 10 Achievement ChartDocument3 pages10 Achievement ChartLyka ollerasNo ratings yet
- Dr. Ashraf Sayeed: Department of OphthalmologyDocument49 pagesDr. Ashraf Sayeed: Department of Ophthalmologysaiful haque100% (1)
- Shabeer Et Al-2018-Journal of PerinatologyDocument8 pagesShabeer Et Al-2018-Journal of PerinatologyrenataNo ratings yet
- IWGIA Book The Indigenous World 2021 ENGDocument824 pagesIWGIA Book The Indigenous World 2021 ENGREy FOxNo ratings yet
- My Project PresentationDocument12 pagesMy Project Presentationkarunasand15No ratings yet
- List of Grocery Importers in Austria Europe PDF FreeDocument11 pagesList of Grocery Importers in Austria Europe PDF FreeEmpy SumardiNo ratings yet
- JECFA Carrageenan MonographDocument5 pagesJECFA Carrageenan MonographSurya SaputraNo ratings yet
- 7-Day Indian Keto Diet Plan & Recipes For Weight LossDocument43 pages7-Day Indian Keto Diet Plan & Recipes For Weight LossachusanachuNo ratings yet
- Request For New Tax DeclarationDocument2 pagesRequest For New Tax DeclarationAsterio MagootNo ratings yet
- Goat Science and Production PDFDocument446 pagesGoat Science and Production PDFRiyaz Khan100% (1)
- Service ProgramDocument47 pagesService ProgramHuseyn aliyevNo ratings yet
- The European Board of Anaesthesiology.2Document4 pagesThe European Board of Anaesthesiology.2readririNo ratings yet
- E560 PSR00 DSDocument4 pagesE560 PSR00 DSSalvador FayssalNo ratings yet
- API 510 Study GuideDocument3 pagesAPI 510 Study GuidedanikakaNo ratings yet
- Aerobic ActivitiesExercises PDFDocument14 pagesAerobic ActivitiesExercises PDFPalma, Arrabela M.No ratings yet