You might also like
- Lymph Nodes Normal and MalignantDocument12 pagesLymph Nodes Normal and MalignantMagzNo ratings yet
- G. Di Monta2014Document6 pagesG. Di Monta2014Kelly Jasmin Meza CapchaNo ratings yet
- Connective Tissue Diseases: Focus On Microcirculatory Bed: O.I. Zarudna, I.K. Venher, A.V. DovbushDocument8 pagesConnective Tissue Diseases: Focus On Microcirculatory Bed: O.I. Zarudna, I.K. Venher, A.V. DovbushdjdNo ratings yet
- Pure Vulvar Langerhans Cell Histiocytosis A Case Report and Literature ReviewDocument8 pagesPure Vulvar Langerhans Cell Histiocytosis A Case Report and Literature ReviewqdvtairifNo ratings yet
- Intima-Media Thickness of The Common Femoral Artery As A Marker of Leg Ulceration in Sickle Cell Disease PatientsDocument6 pagesIntima-Media Thickness of The Common Femoral Artery As A Marker of Leg Ulceration in Sickle Cell Disease PatientsAnonymous 9QxPDpNo ratings yet
- 1 s2.0 S0268960X08000787 Main PDFDocument7 pages1 s2.0 S0268960X08000787 Main PDFmohamedhazemelfollNo ratings yet
- Histopathology - 2009 - Carlson - The Histological Assessment of Cutaneous VasculitisDocument21 pagesHistopathology - 2009 - Carlson - The Histological Assessment of Cutaneous VasculitisleartaNo ratings yet
- Sarcoidosis and Lymphoma Case Series and Literature ReviewDocument6 pagesSarcoidosis and Lymphoma Case Series and Literature Reviewea7sfn0fNo ratings yet
- Calciphylaxis, Another Facet of Mastitis: A Case ReportDocument5 pagesCalciphylaxis, Another Facet of Mastitis: A Case ReportIJAR JOURNALNo ratings yet
- Https:emedicine Medscape Com:article:1227025-PrintDocument18 pagesHttps:emedicine Medscape Com:article:1227025-PrintSalsa BillaNo ratings yet
- Multinucleate Cell Angiohistiocytoma - Confocal DescriptionDocument6 pagesMultinucleate Cell Angiohistiocytoma - Confocal DescriptionMihai LupuNo ratings yet
- RARE COMBINATIONDocument4 pagesRARE COMBINATIONYuniita VerayantiiNo ratings yet
- Ymj 60 174Document8 pagesYmj 60 174Jairo Lino BNo ratings yet
- 1543-2165-133.12.1943 Mass General AutopsiesDocument6 pages1543-2165-133.12.1943 Mass General AutopsiesgasfgdNo ratings yet
- Pediatric Non-Hodgkin Lymphoma Workup - Approach Considerations, Laboratory Studies, Imaging StudiesDocument5 pagesPediatric Non-Hodgkin Lymphoma Workup - Approach Considerations, Laboratory Studies, Imaging StudiestopNo ratings yet
- Jurnal Radiologi 1Document4 pagesJurnal Radiologi 1Adelya Dwi AsyifaNo ratings yet
- Laryngeal Precancer: A Review of The Literature, Commentary, and Comparison With Oral LeukoplakiaDocument10 pagesLaryngeal Precancer: A Review of The Literature, Commentary, and Comparison With Oral LeukoplakiabrboyNo ratings yet
- Systemic Disorders Associated With Peripheral Corneal UlcerationDocument4 pagesSystemic Disorders Associated With Peripheral Corneal UlcerationYoga KharismaNo ratings yet
- Lichen Hypertrophic Vs SCCDocument8 pagesLichen Hypertrophic Vs SCCHamza Abu HumaidNo ratings yet
- KalsifilaksisDocument28 pagesKalsifilaksisAnonymous rt6lXkLZNo ratings yet
- Molecular Diagnosis of Blood Disorder Disease: Trial On Gabonese Sickle Cell PatientsDocument6 pagesMolecular Diagnosis of Blood Disorder Disease: Trial On Gabonese Sickle Cell PatientsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Future Neurol. (2012) 7 (5), 595-612Document18 pagesFuture Neurol. (2012) 7 (5), 595-612Anonymous fg5XXFOSj4No ratings yet
- Urinary Sediment Microscopy in Acute Kidney Injury Associated With COVID-19Document11 pagesUrinary Sediment Microscopy in Acute Kidney Injury Associated With COVID-19Gabriel Felipe CGNo ratings yet
- Diagnosis of Blood and Bone Marrow DisordersFrom EverandDiagnosis of Blood and Bone Marrow DisordersSa A. WangNo ratings yet
- argani2000Document15 pagesargani2000karen.cobenaNo ratings yet
- Articulo 8Document8 pagesArticulo 8Yerly Ramirez MuñozNo ratings yet
- A 56 Year Old Woman With Multiple Pulmonary CystsDocument8 pagesA 56 Year Old Woman With Multiple Pulmonary CystsAchmad Dodi MeidiantoNo ratings yet
- Global Epidemiology of Vasculitis: Richard A. Watts, Jane C. Burns and Aladdin J. MohammadDocument13 pagesGlobal Epidemiology of Vasculitis: Richard A. Watts, Jane C. Burns and Aladdin J. MohammadPaola ZuluagaNo ratings yet
- EsplenomegaliaDocument24 pagesEsplenomegaliaJhonatan Efraín López CarbajalNo ratings yet
- Jurnal OM TransleteDocument7 pagesJurnal OM TransleterisjunNo ratings yet
- Informed Consent in Elective and Emergency LaparosDocument2 pagesInformed Consent in Elective and Emergency LaparosFadi NasrallahNo ratings yet
- Langer 2010Document10 pagesLanger 2010Nelson William UsnayoNo ratings yet
- Calciphylaxis Controversies in Pathogenesis, DiagDocument11 pagesCalciphylaxis Controversies in Pathogenesis, DiagJosh Jimenez RochaNo ratings yet
- Primer: Castleman DiseaseDocument18 pagesPrimer: Castleman DiseaseMarco Aurélio SartoriNo ratings yet
- Case ConDocument9 pagesCase ConDhine Dhine ArguellesNo ratings yet
- Clinical Risk Factors for Organ Involvement in Systemic SclerosisDocument11 pagesClinical Risk Factors for Organ Involvement in Systemic Sclerosisnermal93No ratings yet
- Synchronous Presence of Chronic Lymphocytic Leukaemia and Breast Cancer in Nigerian Adult Females Case SeriesDocument5 pagesSynchronous Presence of Chronic Lymphocytic Leukaemia and Breast Cancer in Nigerian Adult Females Case SeriesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Bone Marrow Evaluation of Patients Having Pancytopenia at Tertiary Care Center, M. Y. Hospital, Indore, India: One-Year StudyDocument4 pagesBone Marrow Evaluation of Patients Having Pancytopenia at Tertiary Care Center, M. Y. Hospital, Indore, India: One-Year StudyivanNo ratings yet
- Hepatic Nodules CEUSDocument8 pagesHepatic Nodules CEUScalustre2016No ratings yet
- Beku 2Document8 pagesBeku 2sri karuniaNo ratings yet
- PapillomaDocument4 pagesPapillomaNovhy GanggutNo ratings yet
- 1 s2.0 S003962571630090X MainDocument14 pages1 s2.0 S003962571630090X MainBenjamin NgNo ratings yet
- Fluid Complications: Malignant Pleural EffusionDocument11 pagesFluid Complications: Malignant Pleural Effusiont4tranNo ratings yet
- White Paper Early Identification of Haematologic MalignanciesDocument5 pagesWhite Paper Early Identification of Haematologic MalignanciesNikhitha Mariya JohnNo ratings yet
- CSCR MedscapeDocument13 pagesCSCR MedscapeFelix Valerian HalimNo ratings yet
- Evaluation of Specific Cytomorphologic Features and CA19-9 LevelsDocument6 pagesEvaluation of Specific Cytomorphologic Features and CA19-9 LevelsТетяна МагасьNo ratings yet
- s41598 019 45312 XDocument8 pagess41598 019 45312 XrakaNo ratings yet
- Hypopituitarism in Langerhans Cell Histiocytosis Seven Cases and Literature ReviewDocument8 pagesHypopituitarism in Langerhans Cell Histiocytosis Seven Cases and Literature ReviewafdtfngqbNo ratings yet
- EScholarship UC Item 7s43p5x8Document4 pagesEScholarship UC Item 7s43p5x8Hafich ErnandaNo ratings yet
- CID Coagulación Intravascular TratamientoDocument16 pagesCID Coagulación Intravascular Tratamientoaraceli garciaNo ratings yet
- Advances in Cutaneous Vasculitis Research and Clinical Care: Avrom Caplan, Robert G. MichelettiDocument8 pagesAdvances in Cutaneous Vasculitis Research and Clinical Care: Avrom Caplan, Robert G. Michelettiarif fatkhurNo ratings yet
- Morphologic Criteria of Invasive Colonic Adenocarcinoma On Biopsy SpecimensDocument8 pagesMorphologic Criteria of Invasive Colonic Adenocarcinoma On Biopsy SpecimensFadilatul HalimahNo ratings yet
- COVID Cholangiopathy Can Occur Despite Mild COVIDDocument2 pagesCOVID Cholangiopathy Can Occur Despite Mild COVIDnaqibsakila4286No ratings yet
- Title For Leukemia Research PaperDocument7 pagesTitle For Leukemia Research Paperjicbmhrif100% (1)
- Retinoblastoma: ProblemsDocument1 pageRetinoblastoma: ProblemsArdianNo ratings yet
- 10 11648 J CRJ 20200802 14Document3 pages10 11648 J CRJ 20200802 14Marj MendezNo ratings yet
- AD1110894Document5 pagesAD1110894dhawalduvey95No ratings yet
- Adeocarcinoma in Colonic Brushing CytologyDocument5 pagesAdeocarcinoma in Colonic Brushing CytologyCarl DonaireNo ratings yet
- AML Presenting With TBDocument10 pagesAML Presenting With TBshahzadNo ratings yet
- Chronic Lymphocytic LeukemiaFrom EverandChronic Lymphocytic LeukemiaMichael HallekNo ratings yet
- Final Project ModelDocument35 pagesFinal Project ModelRichard LiuNo ratings yet
- James Mapp Jr.-Maryland-RAW Powerlifting-JUNIOR MEN 20 TO 23Document1 pageJames Mapp Jr.-Maryland-RAW Powerlifting-JUNIOR MEN 20 TO 23Richard LiuNo ratings yet
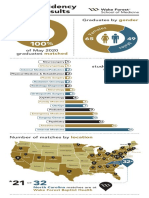
- Wake Forest School of Medicine Match Day Infographic 2020Document1 pageWake Forest School of Medicine Match Day Infographic 2020Richard LiuNo ratings yet
- SA Shigaki OtherSubjectsRuinedMyWritingDocument2 pagesSA Shigaki OtherSubjectsRuinedMyWritingRichard LiuNo ratings yet
- G9S PDS PDFDocument1 pageG9S PDS PDFRichard LiuNo ratings yet
- Arrhythmia Therapy: Henry Halperin, MD, MA, FAHA, FHRSDocument91 pagesArrhythmia Therapy: Henry Halperin, MD, MA, FAHA, FHRSRichard LiuNo ratings yet
- Stochastic protein dynamics, fluctuation-dissipation theoremDocument2 pagesStochastic protein dynamics, fluctuation-dissipation theoremRichard LiuNo ratings yet
- Sbe II Hw5q3Document1 pageSbe II Hw5q3Richard LiuNo ratings yet
- Zombie Apocolypse: The Five Themes of GeographyDocument6 pagesZombie Apocolypse: The Five Themes of Geographyapi-663760583No ratings yet
- Rouge No DengonDocument2 pagesRouge No DengonNaylimar D Alvarez CNo ratings yet
- Impact of Product Rebranding On Organization ProfitabilityDocument63 pagesImpact of Product Rebranding On Organization ProfitabilityDaniel ObasiNo ratings yet
- State of Employee Engagement: Global Survey 2010Document16 pagesState of Employee Engagement: Global Survey 2010aptmbaNo ratings yet
- Subtraction Strategies That Lead To RegroupingDocument6 pagesSubtraction Strategies That Lead To Regroupingapi-171857844100% (1)
- Saint Aquinas and Mercantilism School of ThoughtsDocument11 pagesSaint Aquinas and Mercantilism School of ThoughtsKatunga MwiyaNo ratings yet
- Earth First's - Death ManualDocument9 pagesEarth First's - Death Manualfurious man100% (1)
- Manticore Search Case-Study Layout-InternationalDocument1 pageManticore Search Case-Study Layout-Internationalnilasoft2009No ratings yet
- ICT in Education ComponentsDocument2 pagesICT in Education ComponentsLeah RualesNo ratings yet
- Cutaneous Abscess Furuncles and CarbuclesDocument25 pagesCutaneous Abscess Furuncles and Carbuclesazmmatgowher_1219266No ratings yet
- 15-5240 enDocument14 pages15-5240 enRafa Lopez PuigdollersNo ratings yet
- Rigging & Slinging For Engineers - Purchasers PDFDocument2 pagesRigging & Slinging For Engineers - Purchasers PDFΈνκινουαν Κόγκ ΑδάμουNo ratings yet
- แนวข้อสอบความรู้ความสามารถด้านภาษาอังกฤษที่เกี่ยวข้องกับการปฏิบัติงาน (ชุด4)Document5 pagesแนวข้อสอบความรู้ความสามารถด้านภาษาอังกฤษที่เกี่ยวข้องกับการปฏิบัติงาน (ชุด4)โจโค โบะNo ratings yet
- CV - Diego Allendes - Civil EngineerDocument1 pageCV - Diego Allendes - Civil EngineerPari D. ShitPostingNo ratings yet
- Entrepreneurship Assignment 1 Business Concept ReportDocument2 pagesEntrepreneurship Assignment 1 Business Concept ReportNoor Nabi ShaikhNo ratings yet
- AmendmentDocument29 pagesAmendmentYuvraj Singh TenguriyaNo ratings yet
- Importance of Research in ArchitectureDocument9 pagesImportance of Research in ArchitectureKathleen Mae SoriaNo ratings yet
- Psat Exam 2013Document34 pagesPsat Exam 2013tacobeo50% (4)
- Love Letters Reveal Deep EmotionsDocument21 pagesLove Letters Reveal Deep EmotionsChima NnosimikeNo ratings yet
- AP Microeconomics 2016 Free-Response QuestionsDocument4 pagesAP Microeconomics 2016 Free-Response QuestionsSHIN SeoYoungNo ratings yet
- MISCOMMUNICATIONDocument20 pagesMISCOMMUNICATIONNeha Apa100% (2)
- Ambahan Poetry of The HanuooDocument4 pagesAmbahan Poetry of The HanuooJayrold Balageo MadarangNo ratings yet
- Intro To Rhetorical FunctionDocument28 pagesIntro To Rhetorical FunctiondianNo ratings yet
- Gerunds and Infinitives 8897Document3 pagesGerunds and Infinitives 8897aura lucy estupiñan gutierrezNo ratings yet
- Enterprise Poem by Nissim Ezekiel Summary and AnalysisDocument7 pagesEnterprise Poem by Nissim Ezekiel Summary and AnalysisSk BMNo ratings yet
- Stratigrapghy Mineral Potential of BalochistanDocument45 pagesStratigrapghy Mineral Potential of BalochistanMohsin Ali KhuhawarNo ratings yet
- Cns 1,2,3 CeDocument21 pagesCns 1,2,3 Cejay0% (1)
- An Introduction To The Study of Medieval Latin VersificationDocument246 pagesAn Introduction To The Study of Medieval Latin VersificationGregorio Gonzalez Moreda100% (1)
- Muscovite Mica Flakes and Mica Powder For Industrial ApplicationsDocument5 pagesMuscovite Mica Flakes and Mica Powder For Industrial ApplicationsAnuradhaPatraNo ratings yet
- Eyewitness EvidenceDocument55 pagesEyewitness EvidencenatstarterNo ratings yet