You might also like
- NeuroendosDocument25 pagesNeuroendosBabu Ramakrishnan100% (1)
- ACLS EP Manual Comparison ChartDocument9 pagesACLS EP Manual Comparison Chartkhairunnisa tanjungNo ratings yet
- Lungs & Pleura PDFDocument24 pagesLungs & Pleura PDFEl SpinnerNo ratings yet
- WHO Surgical Safety ChecklistDocument1 pageWHO Surgical Safety ChecklistneculavNo ratings yet
- Nursing Care Plan On Breast Cancer: Encourage Adequate Rest PeriodsDocument1 pageNursing Care Plan On Breast Cancer: Encourage Adequate Rest PeriodsZen Haven100% (4)
- Principles of Safe LaparosDocument28 pagesPrinciples of Safe Laparosolyviutza16No ratings yet
- Anatomia Del Nervio Intercostal Cutaneo Anterior y Su Relacion Con El AcnesDocument5 pagesAnatomia Del Nervio Intercostal Cutaneo Anterior y Su Relacion Con El AcnesBolivar IseaNo ratings yet
- 581.fullDocument19 pages581.fulleric22hkNo ratings yet
- Henne Man 1965Document21 pagesHenne Man 1965Brayan BuitragoNo ratings yet
- s12630-020-01875-2Document22 pagess12630-020-01875-2dalozpa23No ratings yet
- Sonoanatomic ultrasoundDocument6 pagesSonoanatomic ultrasoundsayed imadNo ratings yet
- Interpleural Block - Part 1: ReviewarticleDocument11 pagesInterpleural Block - Part 1: ReviewarticleAlfredo Salinas CastilloNo ratings yet
- Fiber Dissection Technique: Lateral Aspect of The Brain: Surgical Anatomy and TechniqueDocument11 pagesFiber Dissection Technique: Lateral Aspect of The Brain: Surgical Anatomy and TechniqueRafaelNo ratings yet
- ибуки.pdf 2Document3 pagesибуки.pdf 2Platon PopkhadzeNo ratings yet
- Feigl 2020Document8 pagesFeigl 2020eralp cevikkalpNo ratings yet
- Disorders of The Spinal Cord and RootsDocument9 pagesDisorders of The Spinal Cord and RootsMariana Hoyos GallegoNo ratings yet
- Fernandez-Miranda JC. 2007 - Three-Dimensional Microsurgical and Tractographic Anatomy of The White Matter..Document40 pagesFernandez-Miranda JC. 2007 - Three-Dimensional Microsurgical and Tractographic Anatomy of The White Matter..Beyza ZeyrekNo ratings yet
- Ambient CisternDocument8 pagesAmbient CisternAmrutha PCNo ratings yet
- Jurnal 1Document18 pagesJurnal 1YonaaasNo ratings yet
- Harry Et Al-1997-Clinical AnatomyDocument3 pagesHarry Et Al-1997-Clinical AnatomyJuan José CabezasNo ratings yet
- Anatomy of The Deep Fascia of The UpperDocument8 pagesAnatomy of The Deep Fascia of The UpperwladjaNo ratings yet
- Spinal and Epidural Anesthesia: Kenneth Drasner and Merlin D. LarsonDocument32 pagesSpinal and Epidural Anesthesia: Kenneth Drasner and Merlin D. LarsonAngky SatriawanNo ratings yet
- Joa 231 121Document8 pagesJoa 231 121marcelonorisNo ratings yet
- Neuro AnatomyDocument24 pagesNeuro Anatomybirijik7979No ratings yet
- Esp Vs RetrolaminarDocument7 pagesEsp Vs RetrolaminarEdson Mercado100% (1)
- j.ajog.2005.02.108Document9 pagesj.ajog.2005.02.108José Vivas EspinozaNo ratings yet
- 1 PB PDFDocument12 pages1 PB PDFHajar Rafika RaniNo ratings yet
- Nerve Sparing Surgery in Cervical CarcinomaDocument8 pagesNerve Sparing Surgery in Cervical CarcinomaJoana Mikee RasayNo ratings yet
- The Myodural Bridge - A Review of The Literature and Clinical Implications 2014Document9 pagesThe Myodural Bridge - A Review of The Literature and Clinical Implications 2014lukeNo ratings yet
- Femoral Hernia - A Review of Clinical AnatomyDocument6 pagesFemoral Hernia - A Review of Clinical AnatomyFatur RasyidNo ratings yet
- SANCHEZ GONZALEZ FEDERICO. White Matter Topographic Anatomy Applied To Temporal Lobe Surgery. WORLD NEUROSURGERY 2019Document10 pagesSANCHEZ GONZALEZ FEDERICO. White Matter Topographic Anatomy Applied To Temporal Lobe Surgery. WORLD NEUROSURGERY 2019Federicos Sánchez GonzálezNo ratings yet
- CP CommentaryDocument2 pagesCP Commentarykaan_yagmur7711No ratings yet
- Rapm Agosto 2010 Anatomia Del Canal Espinal Toraxico Por RMNDocument6 pagesRapm Agosto 2010 Anatomia Del Canal Espinal Toraxico Por RMNIvette M. Carroll D.No ratings yet
- Anatomy of the Trigeminal Nerve MRIDocument7 pagesAnatomy of the Trigeminal Nerve MRISaurabh SatheNo ratings yet
- Normal Anorectal Musculatures and Changes in Anorectal MalformationDocument9 pagesNormal Anorectal Musculatures and Changes in Anorectal MalformationNaeNo ratings yet
- Exploring Gerota's Fascia Revealing A Gross Image Through Cadaver DissectionDocument3 pagesExploring Gerota's Fascia Revealing A Gross Image Through Cadaver Dissectioneditorial.boardNo ratings yet
- Abdominal Wall Blocks For Intra-Abdominal SurgeryDocument6 pagesAbdominal Wall Blocks For Intra-Abdominal SurgerypitriaNo ratings yet
- Innervation of The Pancreas by Neurons in The GutDocument17 pagesInnervation of The Pancreas by Neurons in The GutGrigorina MitrofanNo ratings yet
- Chapter 20Document8 pagesChapter 20Thái Bảo Nguyễn LêNo ratings yet
- Microsurgical Approaches To The Pulvinar. A Comparative Analysis. J Clin Neurosci 2022Document6 pagesMicrosurgical Approaches To The Pulvinar. A Comparative Analysis. J Clin Neurosci 2022Jorge Alberto MirandaNo ratings yet
- Dura Mater Anatomy and Clinical ImplicationDocument9 pagesDura Mater Anatomy and Clinical ImplicationdcNo ratings yet
- Surgical Pelvic Anatomy in Gynecologic OncologyDocument7 pagesSurgical Pelvic Anatomy in Gynecologic OncologyLuisa MorenoNo ratings yet
- Fundamental of Anatomy: Including THEDocument96 pagesFundamental of Anatomy: Including THEDr-Syed Hammad Hussain-GilaniNo ratings yet
- 1203 FullDocument6 pages1203 FulldaniloNo ratings yet
- Surgery of Intraventricular Tumors.10Document13 pagesSurgery of Intraventricular Tumors.10J. Mario Vasquez MorenoNo ratings yet
- Fetos Autonomico en PelvicDocument8 pagesFetos Autonomico en PelvicSantiago Tomas QuinterosNo ratings yet
- Etchevers Et Al., 1999Document11 pagesEtchevers Et Al., 1999Fabiana R.No ratings yet
- Post - Triangle of NeckDocument5 pagesPost - Triangle of NeckAjay Pal NattNo ratings yet
- 10.2478 - Cejcr 2018 0005Document12 pages10.2478 - Cejcr 2018 0005Rully ZenNo ratings yet
- 1 s2.0 S0007091218304355 MainDocument7 pages1 s2.0 S0007091218304355 MainDanilo SarzuriNo ratings yet
- 10.1007@s40140 019 00333 0Document10 pages10.1007@s40140 019 00333 0TM AnNo ratings yet
- Reicunaculo e MovimentoDocument11 pagesReicunaculo e MovimentoAndre GuimaraesNo ratings yet
- Gamss 2015Document12 pagesGamss 2015angelica cuevasNo ratings yet
- Ultrasound-Guided Fascial PlaneDocument19 pagesUltrasound-Guided Fascial PlaneEnano Narigudo TresNo ratings yet
- 74f4a5 FasciaendopelvicaDocument9 pages74f4a5 Fasciaendopelvicajavieralorenzo1No ratings yet
- Anatomy and Approaches Along The Cerebellar-Brainstem FissuresDocument16 pagesAnatomy and Approaches Along The Cerebellar-Brainstem Fissureskaan_yagmur7711No ratings yet
- 1 s2.0 S0002961004004295 MainDocument6 pages1 s2.0 S0002961004004295 MainResidentes CirugíaNo ratings yet
- Pancoast Tumors: Surgical Approaches and TechniquesDocument13 pagesPancoast Tumors: Surgical Approaches and TechniquesReski Harlianty HarliNo ratings yet
- There Are No Three Physiological Narrowings in The Upper Urinary Tract: A New Concept of The Retroperitoneal Anatomy Around The UreterDocument7 pagesThere Are No Three Physiological Narrowings in The Upper Urinary Tract: A New Concept of The Retroperitoneal Anatomy Around The UreterqweqweqwNo ratings yet
- Thoracic Wall Blocks - From Paravertebral To Retrolaminar To Serratus To Erector Spinae and Back Again e A Review of EvidenceDocument11 pagesThoracic Wall Blocks - From Paravertebral To Retrolaminar To Serratus To Erector Spinae and Back Again e A Review of Evidencediogofc123No ratings yet
- ACS Parotidectomy PDFDocument10 pagesACS Parotidectomy PDFadel santosNo ratings yet
- Diaphragmatic StructuresDocument7 pagesDiaphragmatic StructuresTameemNo ratings yet
- Microsurgical Anatomy of The Central Core of The BrainDocument18 pagesMicrosurgical Anatomy of The Central Core of The BrainZeptalanNo ratings yet
- Spinal Cord Vertebral Column Innervation 1-s2.0-S0004951414606267-MainDocument6 pagesSpinal Cord Vertebral Column Innervation 1-s2.0-S0004951414606267-MainAsadm HosshNo ratings yet
- A Step-by-Step Guide to Cerebral White Matter Fiber DissectionDocument11 pagesA Step-by-Step Guide to Cerebral White Matter Fiber Dissectionalbmu93No ratings yet
- Myology of The Thorax PDFDocument4 pagesMyology of The Thorax PDFlina taziNo ratings yet
- Strabismus and Diplopia After Refractive SurgeryDocument5 pagesStrabismus and Diplopia After Refractive Surgeryyuda saputraNo ratings yet
- Spondylolisthesis PDFDocument2 pagesSpondylolisthesis PDFkriswantiNo ratings yet
- NLE Reviewer Q and ADocument11 pagesNLE Reviewer Q and AJennifer ApostolNo ratings yet
- Download ebook Hadzics Textbook Of Regional Anesthesia And Acute Pain Management Self Assessment And Review Pdf full chapter pdfDocument68 pagesDownload ebook Hadzics Textbook Of Regional Anesthesia And Acute Pain Management Self Assessment And Review Pdf full chapter pdfdonald.mortensen170100% (22)
- Webster Uretroplastia en 4 Etapas.Document13 pagesWebster Uretroplastia en 4 Etapas.LuisamdNo ratings yet
- 2 Study of Female Pelvic Pain ..Document69 pages2 Study of Female Pelvic Pain ..Ghofran Ibrahim HassanNo ratings yet
- Download ebook Greens Operative Hand Surgery 2 Volume Set Pdf full chapter pdfDocument67 pagesDownload ebook Greens Operative Hand Surgery 2 Volume Set Pdf full chapter pdfkathleen.lloyd406100% (22)
- Chapter 16 - Digestive SystemDocument12 pagesChapter 16 - Digestive SystemmargaretNo ratings yet
- Epistaxis ManagementDocument21 pagesEpistaxis ManagementIta Aprilia SaktiNo ratings yet
- OroantfistlkitapblmDocument22 pagesOroantfistlkitapblmshehla khanNo ratings yet
- Course in The WardDocument8 pagesCourse in The WardMalshika JayatissaNo ratings yet
- Comparison of General and Regional Anesthesia in Morbidly Obese Patient Case Report Ijdmd 18Document4 pagesComparison of General and Regional Anesthesia in Morbidly Obese Patient Case Report Ijdmd 18Djustiela KarrangNo ratings yet
- Discussion On Retinal and Eye Problems by DR Somdutt PrasadDocument46 pagesDiscussion On Retinal and Eye Problems by DR Somdutt PrasadSomdutt PrasadNo ratings yet
- Revived Bcis2 TrialDocument10 pagesRevived Bcis2 TrialSundaresan SankarNo ratings yet
- Comfort Dental Fee-Schedule-MO-KS-2014-accessibleDocument1 pageComfort Dental Fee-Schedule-MO-KS-2014-accessibleAllen WilburNo ratings yet
- D 5Document28 pagesD 5Mohamed NagyNo ratings yet
- Our Daily Bread - LEOPOLDDocument4 pagesOur Daily Bread - LEOPOLDJonas Marvin AnaqueNo ratings yet
- A Shade Selection TechniqueDocument4 pagesA Shade Selection TechniqueKirti JajooNo ratings yet
- Diagnostic Laparoscopy: Reason For VisitDocument4 pagesDiagnostic Laparoscopy: Reason For Visitdrnareshkumar3281No ratings yet
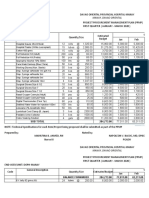
- DOPH-MANAY Procurement Plan for Medical SuppliesDocument16 pagesDOPH-MANAY Procurement Plan for Medical SuppliesJan Oneille Y. VallesNo ratings yet
- Ebp Picc Line - RevisedDocument6 pagesEbp Picc Line - Revisedapi-234544335No ratings yet
- Presentation ProstatectomyDocument38 pagesPresentation Prostatectomyabisinuola8No ratings yet
- Cardiovascular System WORKS SHEET GRANETADocument9 pagesCardiovascular System WORKS SHEET GRANETAFrederick Matthew MendozaNo ratings yet