You might also like
- Acid BaseDocument89 pagesAcid BaseEdouinaNo ratings yet
- Residency: Called - To.See - Patient V1.1Document111 pagesResidency: Called - To.See - Patient V1.1Glen OngNo ratings yet
- Ruppels Manual of Pulmonary Function Testing 10th Edition Mottram Test BankDocument13 pagesRuppels Manual of Pulmonary Function Testing 10th Edition Mottram Test Bankkhuyentryphenakj1100% (32)
- Criteria For Diagnosing Personality DisordersDocument43 pagesCriteria For Diagnosing Personality DisordersKhrycys Olairez RNNo ratings yet
- Approach To Acid-Base Disorders: Quran 5:32Document34 pagesApproach To Acid-Base Disorders: Quran 5:32Hina BatoolNo ratings yet
- Arterial Blood Gas Analysis - making it easyFrom EverandArterial Blood Gas Analysis - making it easyRating: 4.5 out of 5 stars4.5/5 (4)
- Coconut CookbookDocument23 pagesCoconut CookbookNatalia Stone100% (1)
- Arterial Blood GasesDocument10 pagesArterial Blood GasesSoumya BhattacharyaNo ratings yet
- ABG Lecture DR Lenora FernandezDocument60 pagesABG Lecture DR Lenora Fernandezapi-19431894No ratings yet
- ABG Arterial Blood Gas: Interpretation .. Simplified ApproachDocument62 pagesABG Arterial Blood Gas: Interpretation .. Simplified ApproachPrasanna Kumar100% (1)
- SarcoidosisDocument95 pagesSarcoidosisvnybhagat100% (2)
- UNIT: PH and Blood GasesDocument14 pagesUNIT: PH and Blood Gasesbiddyusmc100% (2)
- Arterial Blood Gas - ppt1Document53 pagesArterial Blood Gas - ppt1Madhuri100% (2)
- Metabolism Lippincott's Q&ADocument86 pagesMetabolism Lippincott's Q&Alina amjadNo ratings yet
- Abg Analysis ReviewerDocument21 pagesAbg Analysis ReviewerAyiessa_AJNo ratings yet
- Solar Return ReportDocument5 pagesSolar Return ReportJOYYANo ratings yet
- E RDocument10 pagesE Rroy_linaoNo ratings yet
- Acid-Base Disorders and The ABGDocument28 pagesAcid-Base Disorders and The ABGPaul KelnerNo ratings yet
- Eating Disorders: by Group A1: Marwa Alsaleh, Zahra Almousa, Maha Alshrywi, Israa AlagnamDocument28 pagesEating Disorders: by Group A1: Marwa Alsaleh, Zahra Almousa, Maha Alshrywi, Israa AlagnamYuki HimeNo ratings yet
- Labor Case Digests 7Document7 pagesLabor Case Digests 7Ezra Joy Angagan CanosaNo ratings yet
- Acidosis Alkalosis BiochemistryDocument31 pagesAcidosis Alkalosis BiochemistryliyaNo ratings yet
- ABG Made Simple: DR Satish Deopujari Founder National Chairman (India) PICC 1998Document19 pagesABG Made Simple: DR Satish Deopujari Founder National Chairman (India) PICC 1998Bimantoko Hadi Sriyono100% (1)
- Clinical Chemistry II ELECTROLYTESDocument2 pagesClinical Chemistry II ELECTROLYTESEden MaeNo ratings yet
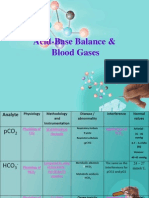
- Acid-Base Balance & Blood GasesDocument39 pagesAcid-Base Balance & Blood GasesSulaiman TahsinNo ratings yet
- StudentDocument2 pagesStudentAnonymous hF5zAdvwCCNo ratings yet
- Acid BaseDocument6 pagesAcid BasejyayNo ratings yet
- Internal Medicine - Phase 3: Important Legal InformationDocument19 pagesInternal Medicine - Phase 3: Important Legal InformationClaire YabaNo ratings yet
- Spirometry and ABG AnalysisDocument23 pagesSpirometry and ABG AnalysisRaihanShaheedNo ratings yet
- Arterial Blood Gas: Interpretation and Clinical ImplicationsDocument112 pagesArterial Blood Gas: Interpretation and Clinical ImplicationsmatrixtrinityNo ratings yet
- Arterial Blood Gases: Laboratory InsightsDocument9 pagesArterial Blood Gases: Laboratory InsightsYusuf NugrohoNo ratings yet
- Abg AnalysisDocument65 pagesAbg AnalysisSyed Farooque AliNo ratings yet
- Arterial Blood Gas Analysis: BY-Shivam Sachan (JR Ii) Moderator - Dr. R.K YADAV (M.D)Document52 pagesArterial Blood Gas Analysis: BY-Shivam Sachan (JR Ii) Moderator - Dr. R.K YADAV (M.D)imranqazi11No ratings yet
- Acid Base and Electrolyte BalanceDocument6 pagesAcid Base and Electrolyte BalanceMuhammad Hamza AlviNo ratings yet
- MCQs of AHN Unit-2 Fluid, Electrolytes & Acid Base ImbalanceDocument7 pagesMCQs of AHN Unit-2 Fluid, Electrolytes & Acid Base Imbalanceloferk44No ratings yet
- ABG - Acidbase Disorders Elmenya University Hospital EGYPTDocument127 pagesABG - Acidbase Disorders Elmenya University Hospital EGYPTkhaledNo ratings yet
- Blood Gas AnalysisDocument5 pagesBlood Gas AnalysisLucy BrittainNo ratings yet
- Blood Gases (Abgs) Interpretation Dr/Baha Eldin Hassan Ahmed Fellow Paediatric Critical CareDocument48 pagesBlood Gases (Abgs) Interpretation Dr/Baha Eldin Hassan Ahmed Fellow Paediatric Critical Carehagir alhajNo ratings yet
- Blood Gases and Acid-Base Disorders: Dr. Wan Nedra Sp. A Pediatricts Departement University of YARSIDocument39 pagesBlood Gases and Acid-Base Disorders: Dr. Wan Nedra Sp. A Pediatricts Departement University of YARSIIQBAL HAKKIKINo ratings yet
- Arterial Blood Gas InterpretationDocument74 pagesArterial Blood Gas InterpretationSarina AsuncionNo ratings yet
- AGD 16 JAN 23. Dr. HERIDocument35 pagesAGD 16 JAN 23. Dr. HERImutiara firdausyNo ratings yet
- Michael Chansky Acid Base Made Easy Handout PDFDocument18 pagesMichael Chansky Acid Base Made Easy Handout PDFAustine OsaweNo ratings yet
- Maimun Zulhaidah A Tinny R Indra Clinical Pathology DeptDocument47 pagesMaimun Zulhaidah A Tinny R Indra Clinical Pathology DeptSunny AghniNo ratings yet
- Clinical Scenario 01Document480 pagesClinical Scenario 01Emon FaizNo ratings yet
- Blood Gases, PH, & Buffer SystemsDocument51 pagesBlood Gases, PH, & Buffer SystemsDiether LanderoNo ratings yet
- Thursday 15 1-30 Jonathan TaliercioDocument74 pagesThursday 15 1-30 Jonathan TaliercioCroitoru CosminNo ratings yet
- ABG Lecture PDFDocument11 pagesABG Lecture PDFbianca maaliwNo ratings yet
- Biochem Acid Base Electrolytes ABGDocument12 pagesBiochem Acid Base Electrolytes ABGNaser Hamdi ZalloumNo ratings yet
- Abg SakshiDocument59 pagesAbg SakshiSakshi GuptaNo ratings yet
- Acid-Base Balance + Arterial Blood GasesDocument30 pagesAcid-Base Balance + Arterial Blood GasesQusai IbraheemNo ratings yet
- Arterial Blood Gas Analysis: DR - Rakesh Chandra Chaurasia PGT 3 Ims, Bhu Moderator: DR - Manjaree Mishra Asset - ProfDocument64 pagesArterial Blood Gas Analysis: DR - Rakesh Chandra Chaurasia PGT 3 Ims, Bhu Moderator: DR - Manjaree Mishra Asset - ProfArmaanjeet SinghNo ratings yet
- 4 5969878728963002643Document21 pages4 5969878728963002643peternady202No ratings yet
- Acid-Base Imbalances: Dr. Emmanuel Sandy Department of Chemical Pathology Comahs-UslDocument49 pagesAcid-Base Imbalances: Dr. Emmanuel Sandy Department of Chemical Pathology Comahs-UslVivian KamaraNo ratings yet
- ABGAnalysis Resident LectureDocument71 pagesABGAnalysis Resident LecturePutu AdhekNo ratings yet
- Metabolic AcidosisDocument102 pagesMetabolic AcidosisShajahan SideequeNo ratings yet
- Arterial Blood Gas Interpretation: Associate Professor Dr. Samah ShehataDocument44 pagesArterial Blood Gas Interpretation: Associate Professor Dr. Samah Shehataraed faisalNo ratings yet
- Computer-Based Scenario Biochemistry: How To Read Bloods?Document66 pagesComputer-Based Scenario Biochemistry: How To Read Bloods?Haytham KhalifaNo ratings yet
- Cases Acid BaseDocument3 pagesCases Acid BaseSa MoNo ratings yet
- Blood Gas Analysis: Respiratory DisordersDocument15 pagesBlood Gas Analysis: Respiratory DisordersYogeshRavalNo ratings yet
- 9.3 Bedside Rules For Acid-Base DisordersDocument4 pages9.3 Bedside Rules For Acid-Base DisordersmahchusNo ratings yet
- PeterLloyd On AcidbaseDocument12 pagesPeterLloyd On AcidbaseThatikala AbhilashNo ratings yet
- 2016 Acid Base DisordersDocument48 pages2016 Acid Base DisordersbellabelbonNo ratings yet
- กรณีศึกษา (case study) อ.เพ็ญนภาDocument8 pagesกรณีศึกษา (case study) อ.เพ็ญนภาKanisthita ChutikittidechapatNo ratings yet
- AbgDocument38 pagesAbgroopaNo ratings yet
- Acid - Base BalanceDocument37 pagesAcid - Base BalanceSittie RamosNo ratings yet
- Arterial Blood Gas AnalysisDocument6 pagesArterial Blood Gas AnalysisMaribee Tagayun EspirituNo ratings yet
- Blood GasesDocument3 pagesBlood GasesFaithNo ratings yet
- Selected Constants: Oxidation–Reduction Potentials of Inorganic Substances in Aqueous SolutionFrom EverandSelected Constants: Oxidation–Reduction Potentials of Inorganic Substances in Aqueous SolutionNo ratings yet
- Chemistry and Biochemistry of Oxygen Therapeutics: From Transfusion to Artificial BloodFrom EverandChemistry and Biochemistry of Oxygen Therapeutics: From Transfusion to Artificial BloodAndrea MozzarelliNo ratings yet
- PlasmidsDocument53 pagesPlasmidsPrerana SikarwarNo ratings yet
- Human Body Systems ProjectDocument9 pagesHuman Body Systems ProjectmrdornNo ratings yet
- Current Affairs Concept Notes For Class 6 To 8.Document2 pagesCurrent Affairs Concept Notes For Class 6 To 8.Learning 360No ratings yet
- Procedure On Knee Orthroscopy-2Document15 pagesProcedure On Knee Orthroscopy-2pslokesha84No ratings yet
- Prescription For Addiction: UpdateDocument8 pagesPrescription For Addiction: Updateoptions1No ratings yet
- Obesity Cultural and Biocultural Perspectives by Alexandra A. BrewisDocument231 pagesObesity Cultural and Biocultural Perspectives by Alexandra A. BrewisDiana Fernanda Espinosa SerranoNo ratings yet
- Acquired Hypopigmentation Disorders Other Than Vitiligo - UpToDateDocument23 pagesAcquired Hypopigmentation Disorders Other Than Vitiligo - UpToDateBhargav YagnikNo ratings yet
- S7A - Guideline - Safety Pharmacology Studies For Human PharmaceuticalsDocument13 pagesS7A - Guideline - Safety Pharmacology Studies For Human Pharmaceuticalsmogmo TsaiNo ratings yet
- English Project: AcknowledgementDocument11 pagesEnglish Project: AcknowledgementAbhishek ChauhanNo ratings yet
- Anemia AplasicaDocument9 pagesAnemia AplasicaCARLOS ALBERTO TORRES SALASNo ratings yet
- Five Myths On Fathers and FamilyDocument42 pagesFive Myths On Fathers and FamilyJOEMAFLAGENo ratings yet
- Initial Data Base To Priority Setting NotesDocument4 pagesInitial Data Base To Priority Setting NotesTangonan DarrelNo ratings yet
- 5 Do We Need Economics in MedicineDocument24 pages5 Do We Need Economics in MedicineHanan AhmedNo ratings yet
- Family Nursing Analysis LatestDocument143 pagesFamily Nursing Analysis LatestLyca Mae AurelioNo ratings yet
- Sas 1-3Document3 pagesSas 1-3Lyons SchimttNo ratings yet
- Hematopoiesis: Part 2: Erythropoiesis and LeukopoiesisDocument62 pagesHematopoiesis: Part 2: Erythropoiesis and LeukopoiesisJohn Marie IdavaNo ratings yet
- By:Dr Herbert Sihite Spog: Divisi Feto Maternal FK Usu /rs HamDocument26 pagesBy:Dr Herbert Sihite Spog: Divisi Feto Maternal FK Usu /rs HamDyn AdrianiNo ratings yet
- ICSE Board Class X Geography Board Paper - 2013: Time: 2 Hrs Total Marks: 80 General InstructionsDocument5 pagesICSE Board Class X Geography Board Paper - 2013: Time: 2 Hrs Total Marks: 80 General InstructionsAmanNo ratings yet
- Shiatsu - Case Study - Diseases - Problems Helped by ShiatsuDocument1 pageShiatsu - Case Study - Diseases - Problems Helped by ShiatsunaveenNo ratings yet
- CattleHandbookApril 2008Document70 pagesCattleHandbookApril 2008majdirossrossNo ratings yet
- Carbon TetrachlorideDocument5 pagesCarbon Tetrachloridesummi64No ratings yet