You might also like
- 20 Home Remedies For Diabetes Type 2Document5 pages20 Home Remedies For Diabetes Type 2leonard1971No ratings yet
- Chronic Complications of Diabetes MellitusDocument40 pagesChronic Complications of Diabetes MellitusironNo ratings yet
- GlargineDocument22 pagesGlargineAgus SuwiryawanNo ratings yet
- ADA Diabetes Management Guidelines 2015Document117 pagesADA Diabetes Management Guidelines 2015Fakhri Firman GunawanNo ratings yet
- Clinical Pharmacy Department Clinical Pharmacy and Drug Information PL 504Document61 pagesClinical Pharmacy Department Clinical Pharmacy and Drug Information PL 504Bassant Ahmed Mahmoud Ragab Abdallah AyaadNo ratings yet
- RX For Selected PtsDocument22 pagesRX For Selected PtsBubu ToNo ratings yet
- Haramaya University College of Health and Medical ScienceDocument39 pagesHaramaya University College of Health and Medical Scienceani gadaNo ratings yet
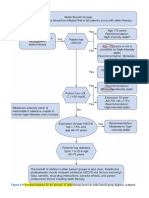
- Recommendations For The Intensity of Statin Therapy Based On Statin Benefit Group Diagram. (AdaptedDocument8 pagesRecommendations For The Intensity of Statin Therapy Based On Statin Benefit Group Diagram. (Adaptedعزالدين الطيارNo ratings yet
- Management of Dyslipidemia and The Prevention of Cardiovascular DiseaseDocument2 pagesManagement of Dyslipidemia and The Prevention of Cardiovascular DiseaseBenny TrisaktyariNo ratings yet
- 2013 ACC/AHA Guideline On The Treatment of Blood Cholesterol To Reduce Atherosclerotic Cardiovascular Risk in AdultsDocument37 pages2013 ACC/AHA Guideline On The Treatment of Blood Cholesterol To Reduce Atherosclerotic Cardiovascular Risk in AdultsIman SaksoukNo ratings yet
- Slide Speaker Candesartan For Hypertension in CKD PatientsDocument43 pagesSlide Speaker Candesartan For Hypertension in CKD Patientsesdras pramuditaNo ratings yet
- LipidsupdateDocument23 pagesLipidsupdatedrshekarforyouNo ratings yet
- Dipiro Edisi 9 KolestrolDocument10 pagesDipiro Edisi 9 KolestrolFriska tampuboLonNo ratings yet
- Dyslipidaemias 2019Document30 pagesDyslipidaemias 2019Adinda DianNo ratings yet
- Cardiometabolic Syndrome: & DR Dhafir A. MahmoodDocument62 pagesCardiometabolic Syndrome: & DR Dhafir A. MahmoodJacob AlphaNo ratings yet
- Cardiometabolic RiskDocument1 pageCardiometabolic RiskVaidya Priyanka SharmaNo ratings yet
- Cardiometabolic syndrome-HOSSAMDocument44 pagesCardiometabolic syndrome-HOSSAMHossam atefNo ratings yet
- Dyslipidaemia - CSA322 Therapeutics in Practice 3ADocument25 pagesDyslipidaemia - CSA322 Therapeutics in Practice 3AV MNo ratings yet
- Screening and Management of Lipids: Patient Population: ObjectiveDocument20 pagesScreening and Management of Lipids: Patient Population: ObjectiveKatie Kroll BradyNo ratings yet
- 2019 - ESC - Guidelines SLIDESDocument23 pages2019 - ESC - Guidelines SLIDESFa CurieNo ratings yet
- Ann Soehee - Tctap2021 - SPCDocument43 pagesAnn Soehee - Tctap2021 - SPCSaad KhanNo ratings yet
- DyslipidemiaDocument12 pagesDyslipidemiawalaaahmed213No ratings yet
- Imaging Detection of PT For Lipid Lowering RXDocument24 pagesImaging Detection of PT For Lipid Lowering RXBubu ToNo ratings yet
- Diabetes LectureDocument65 pagesDiabetes LecturebailovinaflorNo ratings yet
- CCRR 1 114 PDFDocument3 pagesCCRR 1 114 PDFBruno Mario AngelNo ratings yet
- Dyslipidemia 2018Document8 pagesDyslipidemia 2018R JannahNo ratings yet
- Dyslipidemia ATP4 GUIDLINESDocument9 pagesDyslipidemia ATP4 GUIDLINESSandy GunawanNo ratings yet
- Dyslipidemia: Signs and SymptomsDocument24 pagesDyslipidemia: Signs and Symptomschrissanto chandraNo ratings yet
- Dislipid 2 PDFDocument4 pagesDislipid 2 PDFWahyuningsih HamidNo ratings yet
- Classification of DiabetesDocument94 pagesClassification of DiabetesTHAO DANGNo ratings yet
- DiabetesDocument11 pagesDiabetestasneem.salah92No ratings yet
- Antioxidants 12 02091Document46 pagesAntioxidants 12 02091dr.martynchukNo ratings yet
- Asap LipidDocument131 pagesAsap LipidagassiNo ratings yet
- Tratament HipolipemiantDocument11 pagesTratament HipolipemiantClaudiu NicolaievNo ratings yet
- DyslipidemiaDocument30 pagesDyslipidemiaNour Sa'eedNo ratings yet
- Diabetes PDFDocument4 pagesDiabetes PDFAadit GuptaNo ratings yet
- Jhs v3 Id1044 PDFDocument4 pagesJhs v3 Id1044 PDFUrsheila HaekmatiarNo ratings yet
- Management of Blood Cholesterol 2019Document2 pagesManagement of Blood Cholesterol 2019Luis Alberto Alvarez AnkassNo ratings yet
- ObesityDocument33 pagesObesitySusy QuirozNo ratings yet
- Original Article Evaluation of Dyslipidaemia in Type 2 Diabetes Mellitus PatientsDocument6 pagesOriginal Article Evaluation of Dyslipidaemia in Type 2 Diabetes Mellitus PatientsEnvhy AmaliaNo ratings yet
- Dm:Improving Outcomes: A. Consensus RecommendationsDocument21 pagesDm:Improving Outcomes: A. Consensus RecommendationsNarayananNo ratings yet
- Clinical Practice Guidelines For Diabetes ManagementDocument5 pagesClinical Practice Guidelines For Diabetes ManagementIqbal Fida MaulanaNo ratings yet
- Description: C C C C C C C CDocument1 pageDescription: C C C C C C C CEndah budi ArsihNo ratings yet
- Recent Updates To Clinical Practice Guidelines For Diabetes MellituDocument12 pagesRecent Updates To Clinical Practice Guidelines For Diabetes Mellitujimmy HerreraNo ratings yet
- Hypertriglyceridemia - Common Causes, Prevention and Treatment StrategiesDocument10 pagesHypertriglyceridemia - Common Causes, Prevention and Treatment Strategiesfaqihu rizkyNo ratings yet
- A Comprehensive Review On Metabolic SyndromeDocument41 pagesA Comprehensive Review On Metabolic Syndromeveerraju tvNo ratings yet
- Pediatric Patients (10-17 Years of Age)Document18 pagesPediatric Patients (10-17 Years of Age)asdwasdNo ratings yet
- DM LipidDocument5 pagesDM Lipidfelixhalim39No ratings yet
- Case Study 2 MNTDocument11 pagesCase Study 2 MNTapi-242547654No ratings yet
- Diabetes Type 2 PharmacotherapyDocument37 pagesDiabetes Type 2 Pharmacotherapyali khanNo ratings yet
- Cholesterol Guidelines Review 2020Document6 pagesCholesterol Guidelines Review 2020oriannaocantoNo ratings yet
- ADA Standards of Medical Care 2010 FINALDocument130 pagesADA Standards of Medical Care 2010 FINALPram PramonoNo ratings yet
- HypertensionDocument8 pagesHypertensionchandra9000No ratings yet
- Cad Guidelines Secondary 10.04Document2 pagesCad Guidelines Secondary 10.04Wira LinNo ratings yet
- New Frontiers Hipertensi Part2Document8 pagesNew Frontiers Hipertensi Part2Eunike_oisNo ratings yet
- A Study On Evaluating Lipid Profile of Patients With Diabetes MellitusDocument4 pagesA Study On Evaluating Lipid Profile of Patients With Diabetes MellitusPhelix O DaniyanNo ratings yet
- DM Type 2 Practice EssentialsDocument31 pagesDM Type 2 Practice Essentialskuchaibaru90No ratings yet
- New Recommendations and Revised Concepts in Recent Guidelines On The Management of Dyslipidemias To Prevent Cardiovascular Disease-The 2018 ACC-AHA and 2019 ESC-EAS GuidelinesDocument6 pagesNew Recommendations and Revised Concepts in Recent Guidelines On The Management of Dyslipidemias To Prevent Cardiovascular Disease-The 2018 ACC-AHA and 2019 ESC-EAS GuidelinesJustinaNo ratings yet
- 2013 ACC/AHA Blood Cholesterol Treatment Guidelines: "Intensity of Statin Therapy"Document51 pages2013 ACC/AHA Blood Cholesterol Treatment Guidelines: "Intensity of Statin Therapy"dr_yasserNo ratings yet
- Diabetes 2Document18 pagesDiabetes 2Moonjia TyasantiNo ratings yet
- Li 2017Document32 pagesLi 2017akshayNo ratings yet
- Mod 9 DMDocument3 pagesMod 9 DMRoxanne Nasingao100% (1)
- Idf Diabetes Atlas: Middle East and North AfricaDocument2 pagesIdf Diabetes Atlas: Middle East and North Africayogi oktavianNo ratings yet
- ADIPS 2020 Guideline For Pre-Existing Diabetes and PregnancyDocument35 pagesADIPS 2020 Guideline For Pre-Existing Diabetes and PregnancyFelipe Scipiao MouraNo ratings yet
- Carbohydrate To Insulin Ratio - Breakfast-Lunch-DinnerDocument5 pagesCarbohydrate To Insulin Ratio - Breakfast-Lunch-Dinnermario rodriguezNo ratings yet
- Diabetes: Statistics Symptoms Causes Diagnosis PreventionDocument67 pagesDiabetes: Statistics Symptoms Causes Diagnosis PreventionShanthi_KVNo ratings yet
- Afrezza Review For FDADocument12 pagesAfrezza Review For FDACREWNo ratings yet
- ADA Management Adults DKA - UpToDateDocument2 pagesADA Management Adults DKA - UpToDateHiKa SaGoNo ratings yet
- ADA 2020: T2DM Glycemic Goals & Glucose-Lowering GuidelinesDocument10 pagesADA 2020: T2DM Glycemic Goals & Glucose-Lowering GuidelinesLuckybeauty storeNo ratings yet
- Bolli Et Al-2015-Diabetes, Obesity and MetabolismDocument9 pagesBolli Et Al-2015-Diabetes, Obesity and MetabolismKaren RoseroNo ratings yet
- Gestational Diabetes Mellitus: Dr. R V S N Sarma., M.D., M.SC., (Canada)Document45 pagesGestational Diabetes Mellitus: Dr. R V S N Sarma., M.D., M.SC., (Canada)Yohannis AsefaNo ratings yet
- Gestational Diabetes Mellitus - Glycemic Control and Maternal Prognosis - UpToDateDocument46 pagesGestational Diabetes Mellitus - Glycemic Control and Maternal Prognosis - UpToDateBruno FernandesNo ratings yet
- Risk factors of diabetic retinopathy and vision threatening diabetic retinopathy and vision threatening diabetic retinopaty based on diabetic retinopathy screening program in greater bandung, west java.astriDocument14 pagesRisk factors of diabetic retinopathy and vision threatening diabetic retinopathy and vision threatening diabetic retinopaty based on diabetic retinopathy screening program in greater bandung, west java.astriSi PuputNo ratings yet
- Diabetic Keywordio Longtail KeywordsDocument12 pagesDiabetic Keywordio Longtail KeywordsVic HNNo ratings yet
- 2023 Diabetes Mellitus L1 To L8 SVDocument267 pages2023 Diabetes Mellitus L1 To L8 SVThubelihle ZuluNo ratings yet
- Penerapan Empat Pilar Penatalaksanaan Diabetes Mellitus Oleh Kader: Studi FenomenologiDocument8 pagesPenerapan Empat Pilar Penatalaksanaan Diabetes Mellitus Oleh Kader: Studi FenomenologiFauziToushiroNo ratings yet
- Controlling Blood Glucose 1Document2 pagesControlling Blood Glucose 1Tvisha PatelNo ratings yet
- Skugor TreatmentofdiabetesmellitusDocument5 pagesSkugor TreatmentofdiabetesmellitusyomiboyNo ratings yet
- The Diagnosis and Management of Atypical Types of Diabetes: Kathryn Evans Kreider, DNP, FNP-BCDocument7 pagesThe Diagnosis and Management of Atypical Types of Diabetes: Kathryn Evans Kreider, DNP, FNP-BCromyNo ratings yet
- AHG-deprescribing-algorithms-2018-English AntidiabeticDocument2 pagesAHG-deprescribing-algorithms-2018-English Antidiabeticmuhammad irsyad khresna ajiNo ratings yet
- LetterDocument2 pagesLetterapi-384670127No ratings yet
- Insulin and The Oral HypoglycemicsDocument9 pagesInsulin and The Oral HypoglycemicsHasibNo ratings yet
- So What Is Juvenile DiabetesDocument6 pagesSo What Is Juvenile Diabetesapi-274083684No ratings yet
- 1 Octeto de DefronzoDocument23 pages1 Octeto de DefronzoLesli Rodriguez50% (2)
- Stanbio Glucose Oxidase Method and Glucose Determination by ProfameDocument2 pagesStanbio Glucose Oxidase Method and Glucose Determination by ProfameQUIAL BINNo ratings yet
- Pharmaceutical Care in Dm. Apoteker UbayaDocument48 pagesPharmaceutical Care in Dm. Apoteker UbayaViona PrasetyoNo ratings yet
- Neonatal Hypoglycemia September 2022Document30 pagesNeonatal Hypoglycemia September 2022f.abrahamNo ratings yet
- Diabetes Risk Test FreeDocument1 pageDiabetes Risk Test FreeXavier FrancaisNo ratings yet
- Lesson Notes - CBGDocument6 pagesLesson Notes - CBGNicole Marin-ChingNo ratings yet