You might also like
- Immunization Report PDFDocument2 pagesImmunization Report PDFJag UnathNo ratings yet
- PSW6 - PPHFDocument16 pagesPSW6 - PPHFanishthNo ratings yet
- Univ of Florida ImmunisationDocument2 pagesUniv of Florida ImmunisationPavan Kumar MangipudiNo ratings yet
- Pre-Registration Nursing Information For Prospective StudentsDocument4 pagesPre-Registration Nursing Information For Prospective StudentsbthangarajNo ratings yet
- Immunizations Page Effective Spring 2010 Guidelines For Completing Immunization InformationDocument7 pagesImmunizations Page Effective Spring 2010 Guidelines For Completing Immunization InformationShubham TrivediNo ratings yet
- Form B - Other Jobs - High - V High Risk TBDocument8 pagesForm B - Other Jobs - High - V High Risk TBMorshed HumayunNo ratings yet
- Immunization Requirement Form - UpdateDocument2 pagesImmunization Requirement Form - UpdateManojkumar ANo ratings yet
- Immunisation Compliance Certificate 1Document2 pagesImmunisation Compliance Certificate 1api-687735091No ratings yet
- Undertaking Declaration PD2022 - 030Document2 pagesUndertaking Declaration PD2022 - 030MejoNo ratings yet
- Memorandum: Faculty of DentistryDocument3 pagesMemorandum: Faculty of Dentistryabhinav guptaNo ratings yet
- Pre-Placement Assessment Form - Jan 2023Document4 pagesPre-Placement Assessment Form - Jan 2023Nicole KhouryNo ratings yet
- Immunization Record PART I: To Be Completed by The Student. Please Print or TypeDocument3 pagesImmunization Record PART I: To Be Completed by The Student. Please Print or Typeruhayl khanNo ratings yet
- Immunisation Compliance Form 1 2018 Version 5 FinalDocument2 pagesImmunisation Compliance Form 1 2018 Version 5 FinalAnthony Farquhar WuNo ratings yet
- Medical Record FormDocument4 pagesMedical Record FormДария КоваленкоNo ratings yet
- AMOpportunities Certificate of ImmunizationDocument1 pageAMOpportunities Certificate of ImmunizationАида АрзуманянNo ratings yet
- Immunization Letter NB FORM RevisedDocument6 pagesImmunization Letter NB FORM RevisedUddhavendra Pal SinghNo ratings yet
- An Important FormDocument3 pagesAn Important FormRachel ColeNo ratings yet
- Immunization Record: Form Is Due at OrientationDocument3 pagesImmunization Record: Form Is Due at OrientationCasey JonesNo ratings yet
- Appendix 6 Undertaking - Declaration FormDocument1 pageAppendix 6 Undertaking - Declaration FormAr AsifNo ratings yet
- Dd/Mm/Yyyy Dd/Mm/Yyyy Dd/Mm/YyyyDocument6 pagesDd/Mm/Yyyy Dd/Mm/Yyyy Dd/Mm/YyyyJohn50% (2)
- Immuz FormDocument2 pagesImmuz Formapi-250919827No ratings yet
- Good Health in the Tropics: Advice to Travellers and SettlersFrom EverandGood Health in the Tropics: Advice to Travellers and SettlersNo ratings yet
- VSLO Immunization Form 22-23Document6 pagesVSLO Immunization Form 22-23Will HNo ratings yet
- Immun RecordDocument2 pagesImmun RecordNonofYaNo ratings yet
- Infectious Disease Screening Immunisation Policyincluding BBVV 4Document13 pagesInfectious Disease Screening Immunisation Policyincluding BBVV 4aqeelNo ratings yet
- Immreq15 16Document2 pagesImmreq15 16api-234991765No ratings yet
- Phase II To III - 324 Pregnant Women - Randomized Placebo-Controlled Observer-Blind Study of BNT162b2 or Placebo. Start Feb 2021 and End Aug 2022Document11 pagesPhase II To III - 324 Pregnant Women - Randomized Placebo-Controlled Observer-Blind Study of BNT162b2 or Placebo. Start Feb 2021 and End Aug 2022Mary-Jane StevensNo ratings yet
- FIU Immunization Documentation FormDocument2 pagesFIU Immunization Documentation FormMO MONo ratings yet
- Rhodes Immunization RecordDocument5 pagesRhodes Immunization RecordDr.P.S.N RajuNo ratings yet
- University of Minnesota Academic Health Center Student Tuberculosis & Immunization FormDocument2 pagesUniversity of Minnesota Academic Health Center Student Tuberculosis & Immunization Formmikey pNo ratings yet
- GW Hospital MOU & Observer Health Information FormDocument2 pagesGW Hospital MOU & Observer Health Information Formengel0321hotmail.comNo ratings yet
- Immunization FormsDocument8 pagesImmunization FormsJobin JosephNo ratings yet
- MD Occupational Health ProtocolDocument6 pagesMD Occupational Health ProtocolGareth GrechNo ratings yet
- Vaccination Requirements of IFMSA Exchange Progam in Israel-9.15Document2 pagesVaccination Requirements of IFMSA Exchange Progam in Israel-9.15Niko DobrilovicNo ratings yet
- COVID 19 Consent FormDocument2 pagesCOVID 19 Consent FormfvdssfdNo ratings yet
- Kindergarten WorksheetDocument2 pagesKindergarten WorksheetJayRAjNo ratings yet
- Screenshot 2022-08-09 at 1.33.29 PMDocument6 pagesScreenshot 2022-08-09 at 1.33.29 PMsivapraveenaNo ratings yet
- Health Information FormDocument13 pagesHealth Information FormArtero-Cavallaro PabloNo ratings yet
- 2014-2015 Texas Minimum State Vaccine Requirements For Students Grades K-12Document4 pages2014-2015 Texas Minimum State Vaccine Requirements For Students Grades K-12James AllenNo ratings yet
- Immunization Requirement - Student Health Center - The University of UtahDocument2 pagesImmunization Requirement - Student Health Center - The University of Utahmithun916No ratings yet
- Examinee's Guide FOE 2022-10 (Pandemic Edition) ADocument22 pagesExaminee's Guide FOE 2022-10 (Pandemic Edition) ASam DeeNo ratings yet
- Instruction For Medical Examination - eDocument2 pagesInstruction For Medical Examination - emanueltsibiaNo ratings yet
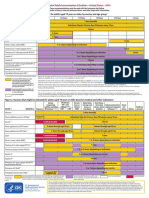
- Figure 1. Recommended Immunization Schedule For Adults Aged 19 Years or Older, by Vaccine and Age GroupDocument2 pagesFigure 1. Recommended Immunization Schedule For Adults Aged 19 Years or Older, by Vaccine and Age GroupmsarasNo ratings yet
- Vaccination Requirement International Students 022019Document2 pagesVaccination Requirement International Students 022019KryzNo ratings yet
- Dear Healthcare Provider 2014Document1 pageDear Healthcare Provider 2014TanuNo ratings yet
- PSW Clinical Requirements Package Fall 2023 InternationalDocument16 pagesPSW Clinical Requirements Package Fall 2023 InternationalAnish KumarNo ratings yet
- Occupational Health QuestionnaireDocument13 pagesOccupational Health QuestionnaireMohamed HafezNo ratings yet
- CUB - Immunisation FormDocument2 pagesCUB - Immunisation FormArcane BeingNo ratings yet
- Ocfs-Medical Statement of Child in ChildcareDocument2 pagesOcfs-Medical Statement of Child in ChildcareNikki NievesNo ratings yet
- 2021 Immunisations FormDocument3 pages2021 Immunisations Formmilksheikh2004No ratings yet
- Health Immunization Clearance Form: Section A: ImmunizationsDocument3 pagesHealth Immunization Clearance Form: Section A: ImmunizationsFaith SetikNo ratings yet
- Adult ScheduleDocument3 pagesAdult ScheduledrmanojvimalNo ratings yet
- ImmunizationCertificate PDFDocument2 pagesImmunizationCertificate PDFAnonymous kq5iEDxxhrNo ratings yet
- Immunization FormsDocument6 pagesImmunization FormsNadya IrsalinaNo ratings yet
- Reading VaccineImmunizationDocument13 pagesReading VaccineImmunizationelztly4694No ratings yet
- ScheduleDocument2 pagesScheduleapi-286634335No ratings yet
- 2019 - 2020 - Boston Immunization - Hult Immunization FormDocument4 pages2019 - 2020 - Boston Immunization - Hult Immunization FormOscar RomainvilleNo ratings yet
- Influenza vaccination: What does the scientific proof say?: Could it be more harmful than useful to vaccinate indiscriminately elderly people, pregnant women, children and health workers?From EverandInfluenza vaccination: What does the scientific proof say?: Could it be more harmful than useful to vaccinate indiscriminately elderly people, pregnant women, children and health workers?No ratings yet
- USMLE Step 3 Lecture Notes 2021-2022: Internal Medicine, Psychiatry, EthicsFrom EverandUSMLE Step 3 Lecture Notes 2021-2022: Internal Medicine, Psychiatry, EthicsRating: 5 out of 5 stars5/5 (9)
- BAMBOO U - 5 Ways To Process BambooDocument11 pagesBAMBOO U - 5 Ways To Process BambooeShappy HomeNo ratings yet
- GBC Module 1Document69 pagesGBC Module 1MOHAMED82% (129)
- Vaccum FilterationDocument6 pagesVaccum FilterationAkshay bhuranNo ratings yet
- Kali Kaula A Manual of Tantric Magick HardbackDocument3 pagesKali Kaula A Manual of Tantric Magick Hardbackalintuta20% (1)
- The Revenge of The SerpentDocument2 pagesThe Revenge of The SerpentMiyamoto MusashiNo ratings yet
- USEFUL TIPS For Repairing LAPTOPDocument17 pagesUSEFUL TIPS For Repairing LAPTOPGeronJosephusLofrancoManaiz100% (1)
- Revised EstimateDocument2 pagesRevised EstimateMd. Abdul HaiNo ratings yet
- Health Benefits of Financial Inclusion A Literature ReviewDocument7 pagesHealth Benefits of Financial Inclusion A Literature Reviewl1wot1j1fon3No ratings yet
- 118CP Selection of CP Systems For Reinforced Concrete StructuresDocument15 pages118CP Selection of CP Systems For Reinforced Concrete StructuresWill NashNo ratings yet
- What Is Splunk - (Easy Guide With Pictures) - Cyber Security KingsDocument9 pagesWhat Is Splunk - (Easy Guide With Pictures) - Cyber Security Kingsrokoman kungNo ratings yet
- Thesis Statement, Topic Sentence, and Supporting Details: Paul Christian Reforsado AbadDocument29 pagesThesis Statement, Topic Sentence, and Supporting Details: Paul Christian Reforsado AbadMicole BrodethNo ratings yet
- Valley Line LRT Preliminary DesignDocument26 pagesValley Line LRT Preliminary DesigncaleyramsayNo ratings yet
- Safety StockDocument8 pagesSafety StockIwan NovaNo ratings yet
- Synthesis of Sufanilic AcidDocument4 pagesSynthesis of Sufanilic AcidWinston Jake Gerolaga0% (1)
- Human Resource ManagementDocument86 pagesHuman Resource ManagementK V S PRASD REDDYNo ratings yet
- Study of Steam Generation Units With Their Accessories and MountingsDocument64 pagesStudy of Steam Generation Units With Their Accessories and MountingsMasudur RahmanNo ratings yet
- .50 BMG - Wikipedia PDFDocument13 pages.50 BMG - Wikipedia PDFAce ActionNo ratings yet
- Goat Fattening Rs. 0.85 MillionDocument18 pagesGoat Fattening Rs. 0.85 MillionZakir Ali100% (1)
- Lenovo Ideapad V110-15AST - LV114A (15270-1 08A03)Document64 pagesLenovo Ideapad V110-15AST - LV114A (15270-1 08A03)Mahmut KaralarNo ratings yet
- Adenosine Deaminase: Quantitative Determination of Adenosine Deaminase (ADA) in Serum and Plasma SamplesDocument1 pageAdenosine Deaminase: Quantitative Determination of Adenosine Deaminase (ADA) in Serum and Plasma Samplesmark.zac1990No ratings yet
- How To ApplyDocument129 pagesHow To ApplySasa KasaNo ratings yet
- STEP English (1-18) All Worksheets 2020Document134 pagesSTEP English (1-18) All Worksheets 2020Shema ZulfiqarNo ratings yet
- Modules in Grade 12: Quarter 1 - Week 3 Academic Track - StemDocument23 pagesModules in Grade 12: Quarter 1 - Week 3 Academic Track - StemZenarose MirandaNo ratings yet
- Energy Sector Capacity Building Diagnostic and Needs Assessment StudyDocument150 pagesEnergy Sector Capacity Building Diagnostic and Needs Assessment StudyAyoub EnergieNo ratings yet
- Special Theory of RelativityDocument16 pagesSpecial Theory of RelativityBrigita SteffyNo ratings yet
- Azam in 30 DuaDocument3 pagesAzam in 30 DuafaizaninNo ratings yet
- NCERT Exemplar Class 8 Maths Solutions Chapter 3 Square-Square Root & Cube-Cube RootDocument77 pagesNCERT Exemplar Class 8 Maths Solutions Chapter 3 Square-Square Root & Cube-Cube Rootdeep34No ratings yet
- First Quarter Examination in PracticalDocument2 pagesFirst Quarter Examination in PracticalMark Anthony B. AquinoNo ratings yet
- Data Mining ToolsDocument9 pagesData Mining Toolspuneet0303No ratings yet
- English Language Unit 1 May 2011Document3 pagesEnglish Language Unit 1 May 2011Kieran RichardsNo ratings yet