You might also like
- Claim: HealthDocument2 pagesClaim: Healthheidigirard1985No ratings yet
- Amount Due: Quest Diagnostics Quest DiagnosticsDocument2 pagesAmount Due: Quest Diagnostics Quest DiagnosticsCurtis SavageNo ratings yet
- FeafeDocument6 pagesFeafemike currieNo ratings yet
- Commission StatementDocument16 pagesCommission StatementJavon DawsonNo ratings yet
- Document PDFDocument2 pagesDocument PDFgregory binghamNo ratings yet
- Enrollment PackageDocument11 pagesEnrollment PackageJose EspinozaNo ratings yet
- Renters InsuranceDocument1 pageRenters InsuranceQuintinaNo ratings yet
- Bar InvoiceDocument8 pagesBar InvoicedelanaNo ratings yet
- Amount Due: Radiology Associates of North Radiology Associates of North Texas TexasDocument2 pagesAmount Due: Radiology Associates of North Radiology Associates of North Texas TexasJordan LouisNo ratings yet
- Secured Card: Trans Post Reference Number Description Credits ChargesDocument3 pagesSecured Card: Trans Post Reference Number Description Credits Chargesinversiones reussi c.a50% (2)
- "High Blood Pressure": Page 1 of 1Document1 page"High Blood Pressure": Page 1 of 1Mark Kevin IIINo ratings yet
- Format LuzDocument2 pagesFormat LuzPaul RiosNo ratings yet
- Climate Action Incentive Payment Notice 2022 06 25 09 46 45 07823 PDFDocument3 pagesClimate Action Incentive Payment Notice 2022 06 25 09 46 45 07823 PDFalex mac dougallNo ratings yet
- Your Settlement NoteDocument3 pagesYour Settlement NoteAbdullatifNo ratings yet
- Account Information: For More Information About Residential Electric Service Please VisitDocument2 pagesAccount Information: For More Information About Residential Electric Service Please VisitJosh FieldsNo ratings yet
- TXUENERGYDocument4 pagesTXUENERGYgarrettloehrNo ratings yet
- TXU - BILL BackupDocument4 pagesTXU - BILL BackupgarrettloehrNo ratings yet
- SignedApplication 9511954983-01 Angela MartinDocument12 pagesSignedApplication 9511954983-01 Angela Martinangelalynnmartin4No ratings yet
- Eob RemittanceDocument2 pagesEob RemittanceAndres ChavarrioNo ratings yet
- Climate Action Incentive Payment Notice 2022 06 25 10 43 34 05652Document3 pagesClimate Action Incentive Payment Notice 2022 06 25 10 43 34 05652Augusto Di MariaNo ratings yet
- RCN Statement 8101-0012997-01.2022-04-03.13022Document4 pagesRCN Statement 8101-0012997-01.2022-04-03.13022Jorge Luis Guerra FlorezNo ratings yet
- ASTCT Invoice7405Document1 pageASTCT Invoice7405HEMATOLOGYCARE DR SK GUPTANo ratings yet
- Invoice J3 Auto RanchDocument2 pagesInvoice J3 Auto Ranchhighpacific71No ratings yet
- 03-23-2017 PDFDocument6 pages03-23-2017 PDFal pomerantzNo ratings yet
- Edi - 20689603 - 20689603-Broker-Mrs Febylyn Rodrigue-07 - 04 - 2018-pdx35439512 PDFDocument6 pagesEdi - 20689603 - 20689603-Broker-Mrs Febylyn Rodrigue-07 - 04 - 2018-pdx35439512 PDFVenis ManahanNo ratings yet
- Amount Due: Radiology Associates of North TexasDocument2 pagesAmount Due: Radiology Associates of North TexasJordan LouisNo ratings yet
- Income StatementDocument3 pagesIncome Statementmichelle.marsh82No ratings yet
- Kyle L Sullivan Game Creek Video LLC 23 Executive DR HUDSON NH 03051-494499Document2 pagesKyle L Sullivan Game Creek Video LLC 23 Executive DR HUDSON NH 03051-494499Валентина Швечикова100% (1)
- Yates Logistics BofA SepDocument7 pagesYates Logistics BofA SepJonathan Seagull LivingstonNo ratings yet
- Payplan TaylorDocument2 pagesPayplan TayloraaronulloaeNo ratings yet
- Estatement 1Document4 pagesEstatement 1Holy Trinity ChapelsNo ratings yet
- BILLDocument1 pageBILLRAMIRESNo ratings yet
- I CRMDocument2 pagesI CRMAnupesh PachoriNo ratings yet
- Summary of Account Activity Payment Information: Protecting What Matters MostDocument4 pagesSummary of Account Activity Payment Information: Protecting What Matters MostJames BergmanNo ratings yet
- AA1B Index Statement of AccountsDocument5 pagesAA1B Index Statement of AccountsbscurNo ratings yet
- Important Message : Advice of DebitDocument2 pagesImportant Message : Advice of DebitGercov WongNo ratings yet
- November 2022: StatementDocument3 pagesNovember 2022: StatementLori Penn100% (1)
- Invoice 008102Document1 pageInvoice 008102Ded MarozNo ratings yet
- Notice of Reassessment 2021 08 16 06 14 37 290772Document4 pagesNotice of Reassessment 2021 08 16 06 14 37 290772api-676582318No ratings yet
- Annual Statement: 1 July 2021 - 30 June 2022Document6 pagesAnnual Statement: 1 July 2021 - 30 June 2022Thong THAONo ratings yet
- Online StatementDocument2 pagesOnline Statementriza aut0No ratings yet
- Ally-Bank-Statement - Helen ZhaoDocument4 pagesAlly-Bank-Statement - Helen ZhaoJonathan Seagull Livingston100% (1)
- Workers Insurance - Schedule of Insurance 2017Document3 pagesWorkers Insurance - Schedule of Insurance 2017Michael FarnellNo ratings yet
- Certificate of Insurance - USDocument1 pageCertificate of Insurance - USme2411506No ratings yet
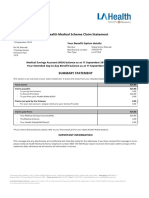
- LA Health Medical Scheme Claim Statement: Statement Number: 5 Your Benefit Option DetailsDocument3 pagesLA Health Medical Scheme Claim Statement: Statement Number: 5 Your Benefit Option DetailsNtaka SimonNo ratings yet
- TX Utility BillDocument4 pagesTX Utility Billfehijan689No ratings yet
- Landicho, Jenny Lyn CalilongDocument1 pageLandicho, Jenny Lyn CalilongJENJEN LANDICHONo ratings yet
- Lowell e Whitehead A Final Draft AmfamDocument6 pagesLowell e Whitehead A Final Draft AmfamLowell WhiteheadNo ratings yet
- New Hope Offer LetterDocument2 pagesNew Hope Offer LetterNew Hope Isabela AgricultureNo ratings yet
- Drape Payment To SIAP 2019.10.29Document1 pageDrape Payment To SIAP 2019.10.29KelvinNo ratings yet
- Notice of Assessment - Year Ended 30 June 2023: !H!ÎÈ/, g4 Î!Ef6ÄDocument4 pagesNotice of Assessment - Year Ended 30 June 2023: !H!ÎÈ/, g4 Î!Ef6Äjoshiepow3llNo ratings yet
- eINV 2022 000125Document2 pageseINV 2022 000125Kim TaehyungNo ratings yet
- Nov 2007Document3 pagesNov 2007api-3742258No ratings yet
- Karla L Erazo 02: Personal InformationDocument1 pageKarla L Erazo 02: Personal InformationDina SaenzNo ratings yet
- DP 790457Document1 pageDP 790457Nelson D. HampacNo ratings yet
- Statement of Account: 676650881 19-May-2018 1,898.99 PDocument2 pagesStatement of Account: 676650881 19-May-2018 1,898.99 PKathyNo ratings yet
- J.K. Lasser's Small Business Taxes 2021: Your Complete Guide to a Better Bottom LineFrom EverandJ.K. Lasser's Small Business Taxes 2021: Your Complete Guide to a Better Bottom LineNo ratings yet
- J.K. Lasser's Small Business Taxes 2007: Your Complete Guide to a Better Bottom LineFrom EverandJ.K. Lasser's Small Business Taxes 2007: Your Complete Guide to a Better Bottom LineNo ratings yet
- PricewaterhouseCoopers' Guide to the New Tax RulesFrom EverandPricewaterhouseCoopers' Guide to the New Tax RulesNo ratings yet
- THVC Receipt in 1OPKAfBU5kHdmwDaJMp33cIuDocument1 pageTHVC Receipt in 1OPKAfBU5kHdmwDaJMp33cIuheidigirard1985No ratings yet
- THVC Receipt in 1OPKAfBU5kHdmwDaJMp33cIuDocument1 pageTHVC Receipt in 1OPKAfBU5kHdmwDaJMp33cIuheidigirard1985No ratings yet
- THVC Receipt in 1OPKAfBU5kHdmwDaJMp33cIuDocument1 pageTHVC Receipt in 1OPKAfBU5kHdmwDaJMp33cIuheidigirard1985No ratings yet
- THVC Receipt in 1OPKAfBU5kHdmwDaJMp33cIuDocument1 pageTHVC Receipt in 1OPKAfBU5kHdmwDaJMp33cIuheidigirard1985No ratings yet
- THVC Receipt in 1OPKAfBU5kHdmwDaJMp33cIuDocument1 pageTHVC Receipt in 1OPKAfBU5kHdmwDaJMp33cIuheidigirard1985No ratings yet
- Holiday Swimming Schedule 2023.2024Document3 pagesHoliday Swimming Schedule 2023.2024heidigirard1985No ratings yet
- THVC Receipt in 1OPKAfBU5kHdmwDaJMp33cIuDocument1 pageTHVC Receipt in 1OPKAfBU5kHdmwDaJMp33cIuheidigirard1985No ratings yet
- THVC Receipt in 1OPKAfBU5kHdmwDaJMp33cIuDocument1 pageTHVC Receipt in 1OPKAfBU5kHdmwDaJMp33cIuheidigirard1985No ratings yet
- THVC Receipt in 1OPKAfBU5kHdmwDaJMp33cIuDocument1 pageTHVC Receipt in 1OPKAfBU5kHdmwDaJMp33cIuheidigirard1985No ratings yet
- The Franchisor Feasibility StudyDocument12 pagesThe Franchisor Feasibility StudyLeighgendary CruzNo ratings yet
- Class NotesDocument24 pagesClass NotesRajat tiwariNo ratings yet
- Summer Training Project ReportDocument48 pagesSummer Training Project Reportanil_batra44100% (1)
- ENG5 Q1 W1 Lesson 3 Filling Out Forms Accurately (School Forms, Deposit Slip, Withdrawal Slip)Document29 pagesENG5 Q1 W1 Lesson 3 Filling Out Forms Accurately (School Forms, Deposit Slip, Withdrawal Slip)Catherine Rica CanonigoNo ratings yet
- Mega KPI BundleDocument11 pagesMega KPI Bundlepepito.supermarket.baliNo ratings yet
- Digital Lending: KenyaDocument31 pagesDigital Lending: KenyaRick OdomNo ratings yet
- Calculating Contractors MarkupDocument3 pagesCalculating Contractors MarkupHorace Prophetic DavisNo ratings yet
- Holiday Homework Class XI Accountancy PDFDocument8 pagesHoliday Homework Class XI Accountancy PDFAlokNo ratings yet
- F2 Joint CostDocument3 pagesF2 Joint CostMyo NaingNo ratings yet
- The General Ledger of Corso Care Corp A Veterinary CompanyDocument2 pagesThe General Ledger of Corso Care Corp A Veterinary CompanyBube KachevskaNo ratings yet
- A Project Report On Financial Statement of Icici Bank PuneDocument85 pagesA Project Report On Financial Statement of Icici Bank PuneAMIT K SINGH0% (1)
- Decision Bar ManualDocument112 pagesDecision Bar ManualAlok Kapoor100% (2)
- Income Tax Lessons July 2019 0 PDFDocument124 pagesIncome Tax Lessons July 2019 0 PDFHannah YnciertoNo ratings yet
- Ringkasan Kinerja Perusahaan TercatatDocument3 pagesRingkasan Kinerja Perusahaan TercatatDian PrasetyoNo ratings yet
- BondsDocument3 pagesBondsMaketh.Man75% (4)
- ISAK 35 Non Profit Oriented EntitiesDocument48 pagesISAK 35 Non Profit Oriented Entitiesnabila dhiyaNo ratings yet
- Debt Collector Disclosure StatementDocument8 pagesDebt Collector Disclosure StatementGreg WilderNo ratings yet
- Capital Allocation Between The Risky and The Risk-Free AssetDocument32 pagesCapital Allocation Between The Risky and The Risk-Free AssetanushreegoNo ratings yet
- (Sem. Vi) 2019 PatternDocument122 pages(Sem. Vi) 2019 PatternJayesh KudalNo ratings yet
- Business Partner Configuration in SAP REFXDocument3 pagesBusiness Partner Configuration in SAP REFXdrdjdNo ratings yet
- Chap 018Document27 pagesChap 018Xeniya Morozova Kurmayeva100% (3)
- Strategy #1 - Stochastic Oscillator + RSI + Triple EMA: Entering A TradeDocument3 pagesStrategy #1 - Stochastic Oscillator + RSI + Triple EMA: Entering A Tradegurdev singh0% (1)
- Mba General Model QPDocument134 pagesMba General Model QPshanvenkyNo ratings yet
- Annexa Prime Trading CoursesDocument11 pagesAnnexa Prime Trading CoursesFatima FX100% (1)
- Hima16 SM 11Document53 pagesHima16 SM 11vahid teymooriNo ratings yet
- 12Document16 pages12JDNo ratings yet
- Cast Study - GM MotorsDocument9 pagesCast Study - GM MotorsAbdullahIsmailNo ratings yet
- Jhurzel Anne S. Aguilar BSBA MM-2105: Personal Income/expenses of The HeirsDocument4 pagesJhurzel Anne S. Aguilar BSBA MM-2105: Personal Income/expenses of The HeirsJESTONI RAMOSNo ratings yet
- Account StatementDocument3 pagesAccount StatementSaeed AnwarNo ratings yet
- LETTER OF ADVICE OrigninalDocument2 pagesLETTER OF ADVICE OrigninalSebastian Wienbreyer67% (6)