You might also like
- Endo Test Bank 1Document6 pagesEndo Test Bank 1mildred alidon100% (1)
- Swedish Massage InfoDocument5 pagesSwedish Massage InfoJoy CelestialNo ratings yet
- Naplex Complete Study Outline A Topic-Wise Approach DiabetesFrom EverandNaplex Complete Study Outline A Topic-Wise Approach DiabetesRating: 4 out of 5 stars4/5 (2)
- Guideline/Drug Updates: 2020 Rxprep Course Book: Update Type DescriptionDocument5 pagesGuideline/Drug Updates: 2020 Rxprep Course Book: Update Type Descriptionsyed100% (1)
- NCLEX: Pharmacology for Nurses: 100 Practice Questions with Rationales to help you Pass the NCLEX!From EverandNCLEX: Pharmacology for Nurses: 100 Practice Questions with Rationales to help you Pass the NCLEX!Rating: 5 out of 5 stars5/5 (4)
- Conginital Heart DiseaseDocument19 pagesConginital Heart DiseaseSanthosh.S.UNo ratings yet
- Antimicrobial Therapy in Veterinary MedicineFrom EverandAntimicrobial Therapy in Veterinary MedicineSteeve GiguèreRating: 4 out of 5 stars4/5 (1)
- Slle Examination Content Guideline - March 05 PDFDocument16 pagesSlle Examination Content Guideline - March 05 PDFYahya Alkamali100% (1)
- Antibiotics in Periodontics PerioDocument51 pagesAntibiotics in Periodontics PerioSiddhartha BanerjeeNo ratings yet
- LincosamidesDocument19 pagesLincosamidesManahil RiazNo ratings yet
- Clindamycin - ClinicalKeyDocument78 pagesClindamycin - ClinicalKeyTRI SETYA NINGSIHNo ratings yet
- Cleocin HCL Clindamycin Hydrochloride Capsules, USP: Reference ID: 4092165Document14 pagesCleocin HCL Clindamycin Hydrochloride Capsules, USP: Reference ID: 4092165krizelNo ratings yet
- Minireview: Clindamycin As An Antimalarial Drug: Review of Clinical TrialsDocument6 pagesMinireview: Clindamycin As An Antimalarial Drug: Review of Clinical TrialsZoel NikonianNo ratings yet
- Micafungin Sodium-100mg Powder For Solution For InfusionDocument6 pagesMicafungin Sodium-100mg Powder For Solution For InfusionMd. Abdur RahmanNo ratings yet
- Vancomycin TDMDocument24 pagesVancomycin TDMAbubakr AurangzebNo ratings yet
- Azithromycin NMFv1.0 Full 20180620Document5 pagesAzithromycin NMFv1.0 Full 20180620Lütfiye ÖzlemNo ratings yet
- Cleocin Clindamycin Phosphate Vaginal Cream, USPDocument19 pagesCleocin Clindamycin Phosphate Vaginal Cream, USPAurelio Villanueva ValleNo ratings yet
- Ganci C LovirDocument8 pagesGanci C LovirJagan JackNo ratings yet
- Clindamycin: A Drug Study OnDocument7 pagesClindamycin: A Drug Study Ondanica grace gubaNo ratings yet
- ClarithromycinDocument4 pagesClarithromycinGAYATHIRINo ratings yet
- New Drugs: Self-Test QuestionsDocument3 pagesNew Drugs: Self-Test QuestionscNo ratings yet
- AzithromycinDocument10 pagesAzithromycinShaina MentangNo ratings yet
- Management of Malaria in Children: Update 2008: GuidelinesDocument5 pagesManagement of Malaria in Children: Update 2008: GuidelinesSaumilNo ratings yet
- ClindaDocument9 pagesClindaAshish KumarNo ratings yet
- How I Treat Methicillin-Resistant Staphylococcal Pyoderma - WSAVA 2014 Congress - VINDocument5 pagesHow I Treat Methicillin-Resistant Staphylococcal Pyoderma - WSAVA 2014 Congress - VINAdil HussainNo ratings yet
- Individualised Dosing of Amikacin in Neonates: A Pharmacokinetic/pharmacodynamic AnalysisDocument9 pagesIndividualised Dosing of Amikacin in Neonates: A Pharmacokinetic/pharmacodynamic AnalysisVeronica Diaz MedinaNo ratings yet
- Product Monograph: (Clindamycin Phosphate Topical Solution USP)Document13 pagesProduct Monograph: (Clindamycin Phosphate Topical Solution USP)igunpharmNo ratings yet
- DownloadDocument2 pagesDownloadfebyNo ratings yet
- Review of Fluconazole Treatment and Prophylaxis For Invasive CandidiasisDocument8 pagesReview of Fluconazole Treatment and Prophylaxis For Invasive CandidiasisOleOhhNo ratings yet
- Clostridium Difficile Guideline - UMMCDocument5 pagesClostridium Difficile Guideline - UMMCdamondouglas100% (3)
- Chapter 044Document5 pagesChapter 044borisdevic223No ratings yet
- ClindamycinDocument5 pagesClindamycinRatna HusnanisaNo ratings yet
- Toxo - OcularDocument2 pagesToxo - OcularviltinivilNo ratings yet
- Comparison of In-Vitro Efficacy of Vanc, LNZ and Dapto Angainst MRSA.Document6 pagesComparison of In-Vitro Efficacy of Vanc, LNZ and Dapto Angainst MRSA.Nawwal NaeemNo ratings yet
- Guidelines AntibioterapieDocument50 pagesGuidelines AntibioterapieVictor Daniel IureaNo ratings yet
- Thyme Increase The Levothyroxine Dose by 30-50%: This Is For Mild To Moderate But For Severe We Will Give Him TriptansDocument66 pagesThyme Increase The Levothyroxine Dose by 30-50%: This Is For Mild To Moderate But For Severe We Will Give Him TriptansOuf'ra AbdulmajidNo ratings yet
- Management of Infection Guidance For Primary Care in IrelandDocument29 pagesManagement of Infection Guidance For Primary Care in IrelandLouise GleesonNo ratings yet
- Brand Name: Dalacin C Generic Name: Clindamycin HCL Drug ClassificationDocument2 pagesBrand Name: Dalacin C Generic Name: Clindamycin HCL Drug Classificationianecunar100% (1)
- NAG Skin and Soft Tissue Infections AdultsDocument21 pagesNAG Skin and Soft Tissue Infections AdultsJun JimenezNo ratings yet
- New JaneDocument34 pagesNew JaneniputusellyowNo ratings yet
- Clinical Management Guidelines For Suspected or Confirmed COVID 19 Infection in Adults Version 4 April 2023 MOH NUGDocument94 pagesClinical Management Guidelines For Suspected or Confirmed COVID 19 Infection in Adults Version 4 April 2023 MOH NUGFrozenboy. 1993No ratings yet
- 18 OctDocument82 pages18 OctAseel AlsheeshNo ratings yet
- I.5 - Ab Necrotizing FasciitisDocument16 pagesI.5 - Ab Necrotizing FasciitisShameen KhanNo ratings yet
- Bedaquiline-Pretomanid-Linezolid Regimens For Drug-Resistant Tuberculosis 2022Document14 pagesBedaquiline-Pretomanid-Linezolid Regimens For Drug-Resistant Tuberculosis 2022awaluddin andyNo ratings yet
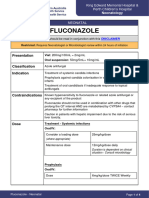
- FluconazoleDocument4 pagesFluconazoleeucaNo ratings yet
- Gentamicin in NeonatusDocument9 pagesGentamicin in NeonatusSalsabila RaniahNo ratings yet
- Individualising Netilmicin Dosing in NeonatesDocument8 pagesIndividualising Netilmicin Dosing in Neonatesainun endarwatiNo ratings yet
- 10 1 1 894 8805 PDFDocument3 pages10 1 1 894 8805 PDFSyahrida Dian ArdhanyNo ratings yet
- Buletin Farmasi 02/2013Document19 pagesBuletin Farmasi 02/2013afiq83No ratings yet
- Pedoman Penggunaan Antibiotik Pada PasienDocument5 pagesPedoman Penggunaan Antibiotik Pada PasienErvina Lie100% (1)
- Spontaneous Bacterial Peritonitis Organism-Specific Therapy - Specific Organisms and Therapeutic RegimensDocument2 pagesSpontaneous Bacterial Peritonitis Organism-Specific Therapy - Specific Organisms and Therapeutic RegimensDung TranNo ratings yet
- ClindamycinDocument2 pagesClindamycinarkee_06No ratings yet
- Enteral InfectionsDocument6 pagesEnteral InfectionsAshley CheungNo ratings yet
- S 013 LBLDocument6 pagesS 013 LBLNexi anessaNo ratings yet
- Diagnosis and Treatment of Clostridioides (Clostridium) Difficile Infection in Adults in 2020Document2 pagesDiagnosis and Treatment of Clostridioides (Clostridium) Difficile Infection in Adults in 2020Alem OrihuelaNo ratings yet
- Guideline: Antibiotic Drug Monitoring: Aminoglycosides and GlycopeptidesDocument8 pagesGuideline: Antibiotic Drug Monitoring: Aminoglycosides and GlycopeptidesKenRodulfReyesVillaruelNo ratings yet
- Clindamycin 1Document21 pagesClindamycin 1ksachchuNo ratings yet
- Clinical Practice Guideline For The Management of Candidiasis: 2016 Update by The Infectious Diseases Society of AmericaDocument50 pagesClinical Practice Guideline For The Management of Candidiasis: 2016 Update by The Infectious Diseases Society of Americalama rashedNo ratings yet
- TB PosterDocument1 pageTB PosterSucie 1997No ratings yet
- Clinical Practice Guideline For The Management of Candidiasis: 2016 Update by The Infectious Diseases Society of AmericaDocument50 pagesClinical Practice Guideline For The Management of Candidiasis: 2016 Update by The Infectious Diseases Society of AmericaRosangel GomezNo ratings yet
- Management of Infection in Primary Care Adapted For Local UseDocument15 pagesManagement of Infection in Primary Care Adapted For Local UseWizri SuharianiNo ratings yet
- Case Presentation: Clostridium DifficileDocument35 pagesCase Presentation: Clostridium DifficileDnse LucidoNo ratings yet
- Amoxicillin (Amoxycillin) : PresentationDocument4 pagesAmoxicillin (Amoxycillin) : PresentationRavikiran SuryanarayanamurthyNo ratings yet
- Biomedical Waste Management Colour Coding For BeginnersDocument3 pagesBiomedical Waste Management Colour Coding For BeginnersMotherterrasa VocationalNo ratings yet
- Do Not Resuscitate: Words Used in The EMS DNR Order Act and FormDocument2 pagesDo Not Resuscitate: Words Used in The EMS DNR Order Act and FormSteven EtheredgeNo ratings yet
- 37 - Acute Rheumatic FeverDocument1 page37 - Acute Rheumatic FevernasibdinNo ratings yet
- Chronic Kidney Disease (CKD) and DiabetesDocument35 pagesChronic Kidney Disease (CKD) and Diabetesm29hereNo ratings yet
- Referensi Referat ObgynDocument10 pagesReferensi Referat ObgynFaradiba NoviandiniNo ratings yet
- Thesis Statement For Breast Cancer Paper PDFDocument6 pagesThesis Statement For Breast Cancer Paper PDFgcq5c1pv100% (1)
- New Diagnostic Criteria For Acute Pericarditis A Cardiac MRIDocument6 pagesNew Diagnostic Criteria For Acute Pericarditis A Cardiac MRIsaNo ratings yet
- Fat: An Emerging Player in The Field of Atrial FibrillationDocument4 pagesFat: An Emerging Player in The Field of Atrial FibrillationKevinJuliusTanadyNo ratings yet
- Adults 6Document7 pagesAdults 6Bshara SleemNo ratings yet
- NDocument136 pagesNLove HumanNo ratings yet
- S - "Sakit Ahong Tinahian" As Verbalized byDocument6 pagesS - "Sakit Ahong Tinahian" As Verbalized bylandilinoNo ratings yet
- Iem India Perspective N B Kumta MaharashtraDocument8 pagesIem India Perspective N B Kumta Maharashtraavijitcu2007No ratings yet
- Gauze-Based Negative Pressure Wound TherapyDocument20 pagesGauze-Based Negative Pressure Wound TherapyAbdilla RidhwanNo ratings yet
- Cerebrospinal Fluid: Learning ObjectivesDocument18 pagesCerebrospinal Fluid: Learning ObjectivesJonalyn LumantasNo ratings yet
- BAER - Brainstem Auditory Evoked ResponseDocument2 pagesBAER - Brainstem Auditory Evoked ResponseAhmad Badrul AminNo ratings yet
- Jurnal MeiristaDocument8 pagesJurnal Meiristameirista deviNo ratings yet
- In Favour of An Investigation of The Relationship Between Vitamin B12 Deficiency and HIV InfectionDocument3 pagesIn Favour of An Investigation of The Relationship Between Vitamin B12 Deficiency and HIV InfectionPJ 123No ratings yet
- Medicaid Family TherapyDocument685 pagesMedicaid Family TherapyfejjinsNo ratings yet
- Vascular TraumaDocument16 pagesVascular TraumaAndi Suchy Qumala SarieNo ratings yet
- Peptic Ulcer DiseaseDocument7 pagesPeptic Ulcer DiseaseDiriba FedasaNo ratings yet
- Hepatitis ADocument11 pagesHepatitis AIGA ABRAHAMNo ratings yet
- Important Notice - 59 - 2022 Dated 22.03.2022 Available Seats Foreign National Spon INI CET PG Courses July 2022Document2 pagesImportant Notice - 59 - 2022 Dated 22.03.2022 Available Seats Foreign National Spon INI CET PG Courses July 2022Bilal Ahmed MultaniNo ratings yet
- Nursing Hyperthyroidism Study GuideDocument4 pagesNursing Hyperthyroidism Study GuideLin SookdeeNo ratings yet
- Septic ShockDocument26 pagesSeptic ShockIma SoniaNo ratings yet
- Inpatient Glycemic ManagementDocument13 pagesInpatient Glycemic Managementmiss betawiNo ratings yet
- DuchenneDocument13 pagesDuchennejenika studiesNo ratings yet