You might also like
- Synthesis of 2-methyl-4-selenoquinazolone, 2-phenylbenzoselenazole, and its derivativesFrom EverandSynthesis of 2-methyl-4-selenoquinazolone, 2-phenylbenzoselenazole, and its derivativesNo ratings yet
- 21 Cephalosp 2015 Mandell Douglas and Bennett S Principles and PracticeDocument20 pages21 Cephalosp 2015 Mandell Douglas and Bennett S Principles and PracticeHelen DyNo ratings yet
- Patrick: An Introduction To Medicinal Chemistry 5e: PenicillinsDocument40 pagesPatrick: An Introduction To Medicinal Chemistry 5e: PenicillinsSumiya HaqueNo ratings yet
- Acid, Protons and Helicobacter PyloriDocument16 pagesAcid, Protons and Helicobacter PyloriJessa De GuzmanNo ratings yet
- Proton Pump Inhibitors PDFDocument4 pagesProton Pump Inhibitors PDFBintoo SharmaNo ratings yet
- Penicillin PharmacologyDocument8 pagesPenicillin Pharmacologygulshan araNo ratings yet
- Antiulcer Proton Pump Inhibitor: Dr. Mai Ramadan Pharm Chem 4Document42 pagesAntiulcer Proton Pump Inhibitor: Dr. Mai Ramadan Pharm Chem 4Ahmed FouadNo ratings yet
- The Proton-Pump Inhibitors: Similarities and DifferencesDocument15 pagesThe Proton-Pump Inhibitors: Similarities and Differencesnikhil bhandiwadNo ratings yet
- Betalactam I-Dai Hoc-Janvier 2012.SVDocument67 pagesBetalactam I-Dai Hoc-Janvier 2012.SVsinhnocNo ratings yet
- CephalosporinsrinDocument25 pagesCephalosporinsrinIsrar Qureshi100% (1)
- B-Lactam Ab 2Document34 pagesB-Lactam Ab 2Ph.first SNo ratings yet
- An Overview On Asenapine MaleateDocument6 pagesAn Overview On Asenapine MaleatePetar DimkovNo ratings yet
- Beta Lactams PenicillinsDocument46 pagesBeta Lactams PenicillinsJoel GamaNo ratings yet
- Cephalosporins Andes Craig PDFDocument18 pagesCephalosporins Andes Craig PDFMansi singhNo ratings yet
- Cardinal Requirements Namely:: Capable, in Small Concentrations, of Inhibiting The Life Processes of Micro-Organisms.'Document20 pagesCardinal Requirements Namely:: Capable, in Small Concentrations, of Inhibiting The Life Processes of Micro-Organisms.'SalmanNo ratings yet
- NIH Public Access: Author ManuscriptDocument28 pagesNIH Public Access: Author Manuscriptfirman wicaksanaNo ratings yet
- Cell Wall Inhibitors: Robert L. Copeland, Ph.D. 28 January 2013Document61 pagesCell Wall Inhibitors: Robert L. Copeland, Ph.D. 28 January 2013Fawaazulla KhanNo ratings yet
- NIH Public Access: Author ManuscriptDocument11 pagesNIH Public Access: Author Manuscriptmonarch01No ratings yet
- The Dramatic Success of Pharmacological Acid Suppression in Healing Peptic Ulcers and Managing Patients With Gastroesophageal Reflux DiseaseDocument27 pagesThe Dramatic Success of Pharmacological Acid Suppression in Healing Peptic Ulcers and Managing Patients With Gastroesophageal Reflux DiseaseTổ 29 D20CNo ratings yet
- Proteus Mirabilis and Is The Agent of Choice Against Haemophilus Influenzae Infections. Ampicillin, TogetherDocument1 pageProteus Mirabilis and Is The Agent of Choice Against Haemophilus Influenzae Infections. Ampicillin, TogetherYap JackyNo ratings yet
- Pharmacology of OxaliplatinDocument16 pagesPharmacology of OxaliplatinAliza JafriNo ratings yet
- Review Article: The Clinical Pharmacology of Proton Pump InhibitorsDocument7 pagesReview Article: The Clinical Pharmacology of Proton Pump InhibitorsNurul Kamilah SadliNo ratings yet
- CEPHALOSPORINSDocument38 pagesCEPHALOSPORINSnasibdin50% (2)
- Product Information: CAS Registry NumberDocument18 pagesProduct Information: CAS Registry Numbermdlc6878No ratings yet
- CeftarolinaDocument9 pagesCeftarolinaLavinia RizeaNo ratings yet
- Local Anaesthetic Agents: Learning ObjectivesDocument5 pagesLocal Anaesthetic Agents: Learning ObjectivesMoises EscobarNo ratings yet
- Medicinal Chemistry of Beta-Lactam AntibioticsDocument13 pagesMedicinal Chemistry of Beta-Lactam AntibioticsJosiah O OmobaNo ratings yet
- 9... Bendale Mol, Vanilin, P-Toluidin, Eluen KLT, Sonikator, MetanolDocument7 pages9... Bendale Mol, Vanilin, P-Toluidin, Eluen KLT, Sonikator, MetanolTalitha Zulis INo ratings yet
- Bioorganic Chemistry: SciencedirectDocument12 pagesBioorganic Chemistry: SciencedirectPooja NaikNo ratings yet
- Antibiotics PDFDocument49 pagesAntibiotics PDFgautamtajesh1983No ratings yet
- Antihistamines: Student Learning GoalsDocument45 pagesAntihistamines: Student Learning GoalsDaniel WangNo ratings yet
- Chapter 6 Answers An Introduction To Medicinal Chemistry Patrick 4e Questions in The Book AnswersDocument3 pagesChapter 6 Answers An Introduction To Medicinal Chemistry Patrick 4e Questions in The Book Answersnishi kNo ratings yet
- Pharmacokinetics and Pharmacodynamics of The Proton Pump InhibitorsDocument11 pagesPharmacokinetics and Pharmacodynamics of The Proton Pump InhibitorsHadiNugrahaNo ratings yet
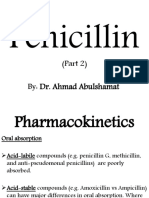
- Penicillin: (Part 2) By: Dr. Ahmad AbulshamatDocument25 pagesPenicillin: (Part 2) By: Dr. Ahmad AbulshamatLubna AliNo ratings yet
- Sahoo 2020Document31 pagesSahoo 2020quanleminh1203No ratings yet
- Yagiela John A Et Al Pharmacology and Therapeutics For Denti1Document1 pageYagiela John A Et Al Pharmacology and Therapeutics For Denti1AntonPurpurovNo ratings yet
- 2001 FullDocument6 pages2001 FullAndréRochaNo ratings yet
- Lecture-PPI 20230226Document25 pagesLecture-PPI 20230226Mahadi Hasan KhanNo ratings yet
- Discovery of PenicillinDocument25 pagesDiscovery of PenicillinBhagyashree BachhavNo ratings yet
- Amb Cyclodextrin 3Document2 pagesAmb Cyclodextrin 3habibNo ratings yet
- Asam Basa BahanDocument6 pagesAsam Basa BahanM Fathur Arief KurniawanNo ratings yet
- Organophosphate and Carbamate Poisoning: Review of The Current Literature and Summary of Clinical and Laboratory Experience in Southern IsraelDocument4 pagesOrganophosphate and Carbamate Poisoning: Review of The Current Literature and Summary of Clinical and Laboratory Experience in Southern IsraelIstigfarani InNo ratings yet
- Chemical Compound Formula C H O: Adolf Von Baeyer AcidDocument4 pagesChemical Compound Formula C H O: Adolf Von Baeyer AcidEduard TanNo ratings yet
- Penicillin and Semisynthetic Penicillins in Dermatology: Disease-a-Month June 2004Document13 pagesPenicillin and Semisynthetic Penicillins in Dermatology: Disease-a-Month June 2004Darajjee mokonninNo ratings yet
- Hitesha & KrupeshDocument25 pagesHitesha & KrupeshkishanNo ratings yet
- OrganicDocument27 pagesOrganicمحمد رحمان محمد الدليميNo ratings yet
- Medicinal Chemistry - PenicillinDocument39 pagesMedicinal Chemistry - PenicillinV G Viju KumarNo ratings yet
- Antibacterial AntibioticsDocument13 pagesAntibacterial AntibioticsMuhamed ArsalanNo ratings yet
- Antibiotic 1Document10 pagesAntibiotic 1echsrykNo ratings yet
- Adrenergic AgentsDocument7 pagesAdrenergic AgentsMuhamed ArsalanNo ratings yet
- Antimalarial Drugs History, New Antimalarial Drugs and Antimalarial Vaccines MalariaDocument9 pagesAntimalarial Drugs History, New Antimalarial Drugs and Antimalarial Vaccines MalariainzemamNo ratings yet
- Medichem CA 2Document5 pagesMedichem CA 2Tejsingh BhatiNo ratings yet
- STPM Trial 2009 Bio Q&A (Kedah)Document39 pagesSTPM Trial 2009 Bio Q&A (Kedah)SimPorNo ratings yet
- Pharmacokinetics Sample Problem With RatioDocument2 pagesPharmacokinetics Sample Problem With RatioAnneNo ratings yet
- Vonoprazan Diference From PPIDocument11 pagesVonoprazan Diference From PPIHaseeb KhanNo ratings yet
- Efficient Synthesis of Benzo...Document7 pagesEfficient Synthesis of Benzo...Douglas DíazNo ratings yet
- Beta Lactam AntibioticsDocument51 pagesBeta Lactam Antibioticsghostcallofduty101propNo ratings yet
- Bioteehnology: App//ed ., Microb/ok GyDocument7 pagesBioteehnology: App//ed ., Microb/ok GySandraColoradoNo ratings yet
- OMEPRAZOLE Is The First of A New Class of Drugs That Inhibit Gastric Secretion by Altering The Activity of HDocument39 pagesOMEPRAZOLE Is The First of A New Class of Drugs That Inhibit Gastric Secretion by Altering The Activity of HRinNo ratings yet
- ابيجينين غلوكوز PDFDocument5 pagesابيجينين غلوكوز PDFMahmoud MokdadNo ratings yet
- Intravitreal DrugsDocument14 pagesIntravitreal Drugsch_prathi7654100% (1)
- PEDIATRIC Drug Formulary 2019-20Document56 pagesPEDIATRIC Drug Formulary 2019-20Eva Marie GonzalesNo ratings yet
- Daftar Harga: NO Nama Produk Komposisi Kemasan HNA Produk PsikiatriDocument3 pagesDaftar Harga: NO Nama Produk Komposisi Kemasan HNA Produk Psikiatriaudy moraniNo ratings yet
- Sildenafil Citrate: Sexual DysfunctionDocument8 pagesSildenafil Citrate: Sexual DysfunctionPits MitsNo ratings yet
- Pharmacology NotesDocument87 pagesPharmacology NotesAnonymous anXPzpy4100% (1)
- Buvanendran 2009 Acute-PainDocument2 pagesBuvanendran 2009 Acute-PainOmar BazalduaNo ratings yet
- GloveOn COATS Full SpecsDocument9 pagesGloveOn COATS Full Specsbob50% (2)
- RA & Gout Case StudyDocument4 pagesRA & Gout Case StudyJossua RyanNo ratings yet
- Stok Obat April 2019Document102 pagesStok Obat April 2019SITIMUTHOHHAROHNo ratings yet
- Drug CalculationDocument34 pagesDrug CalculationMalathi VarnaNo ratings yet
- History of Pharmaceutical IndustryDocument2 pagesHistory of Pharmaceutical IndustryEswar Gupta Maddi67% (6)
- BIODATA GauravDocument11 pagesBIODATA Gauravgaurav tiwariNo ratings yet
- Exercise 5 InternDocument5 pagesExercise 5 InternJ-Mi AlejanoNo ratings yet
- Guidelines For Treatment of OnychomycosisDocument9 pagesGuidelines For Treatment of OnychomycosisOlga Cîrstea100% (1)
- Medication Errors: BY DR - Divya Ashok Kulkarni. Pharm DDocument68 pagesMedication Errors: BY DR - Divya Ashok Kulkarni. Pharm DShrenil LagadNo ratings yet
- Drug of ChoiceDocument5 pagesDrug of ChoiceAsmaa RadwanNo ratings yet
- Christopher Bales Grew Up in Josephine County and Died of A Drug Overdose Two Years Ago in Portland.Document1 pageChristopher Bales Grew Up in Josephine County and Died of A Drug Overdose Two Years Ago in Portland.GeorgiaNo ratings yet
- Biperiden (C)Document2 pagesBiperiden (C)Mae Ann Bueno CastillonNo ratings yet
- InformasiStokBarang2Detil 20180428 075423Document50 pagesInformasiStokBarang2Detil 20180428 075423Bahtiar LangitNo ratings yet
- Antibiotics - FosfomycinDocument2 pagesAntibiotics - FosfomycinSsNo ratings yet
- Duavent DrugstudyDocument1 pageDuavent DrugstudyJustine Garcia67% (3)
- Keto LogDocument7 pagesKeto LogKim Justin InfantadoNo ratings yet
- Drug InteractionDocument20 pagesDrug InteractionRajendra Moorthy RajendranNo ratings yet
- Obat EdDocument6 pagesObat EdMurniyantiNo ratings yet
- Pengantar Farmasi IndustriDocument14 pagesPengantar Farmasi IndustriNorma YunitaNo ratings yet
- Teva PharmaceuticalDocument17 pagesTeva PharmaceuticalGanesh VedhachalamNo ratings yet
- LIST OF REGISTERED DRUGS As of December 2012: DR No Generic Brand Strength Form CompanyDocument35 pagesLIST OF REGISTERED DRUGS As of December 2012: DR No Generic Brand Strength Form CompanyBenjamin TantiansuNo ratings yet
- Spravato For Treatment Resistant DepressionDocument7 pagesSpravato For Treatment Resistant DepressionRobert ChambersNo ratings yet
- Drug Distribution in Hospital PharmacyDocument69 pagesDrug Distribution in Hospital PharmacyAnjali TakkeNo ratings yet
- Substance AbuseDocument32 pagesSubstance AbuseBryan Mae H. Degorio100% (3)
- Periodic Tales: A Cultural History of the Elements, from Arsenic to ZincFrom EverandPeriodic Tales: A Cultural History of the Elements, from Arsenic to ZincRating: 3.5 out of 5 stars3.5/5 (137)
- The Nature of Drugs Vol. 1: History, Pharmacology, and Social ImpactFrom EverandThe Nature of Drugs Vol. 1: History, Pharmacology, and Social ImpactRating: 5 out of 5 stars5/5 (5)
- Essential Chemistry for Formulators of Semisolid and Liquid DosagesFrom EverandEssential Chemistry for Formulators of Semisolid and Liquid DosagesRating: 5 out of 5 stars5/5 (2)
- ICH Quality Guidelines: An Implementation GuideFrom EverandICH Quality Guidelines: An Implementation GuideAndrew TeasdaleNo ratings yet
- Chemistry for Breakfast: The Amazing Science of Everyday LifeFrom EverandChemistry for Breakfast: The Amazing Science of Everyday LifeRating: 4.5 out of 5 stars4.5/5 (14)
- The Nature of Drugs Vol. 1: History, Pharmacology, and Social ImpactFrom EverandThe Nature of Drugs Vol. 1: History, Pharmacology, and Social ImpactRating: 5 out of 5 stars5/5 (1)
- Chemistry: a QuickStudy Laminated Reference GuideFrom EverandChemistry: a QuickStudy Laminated Reference GuideRating: 5 out of 5 stars5/5 (1)
- The Periodic Table: A Very Short IntroductionFrom EverandThe Periodic Table: A Very Short IntroductionRating: 4.5 out of 5 stars4.5/5 (4)
- Lime and Limestone: Chemistry and Technology, Production and UsesFrom EverandLime and Limestone: Chemistry and Technology, Production and UsesRating: 4 out of 5 stars4/5 (1)
- The Regenerative Grower's Guide to Garden Amendments: Using Locally Sourced Materials to Make Mineral and Biological Extracts and FermentsFrom EverandThe Regenerative Grower's Guide to Garden Amendments: Using Locally Sourced Materials to Make Mineral and Biological Extracts and FermentsRating: 5 out of 5 stars5/5 (3)
- Dust Explosion and Fire Prevention Handbook: A Guide to Good Industry PracticesFrom EverandDust Explosion and Fire Prevention Handbook: A Guide to Good Industry PracticesNo ratings yet
- The Production of Volatile Oils and Perfumery Plants in the United StatesFrom EverandThe Production of Volatile Oils and Perfumery Plants in the United StatesNo ratings yet
- AP Chemistry Flashcards, Fourth Edition: Up-to-Date Review and PracticeFrom EverandAP Chemistry Flashcards, Fourth Edition: Up-to-Date Review and PracticeNo ratings yet
- The Nature of Drugs Vol. 2: History, Pharmacology, and Social ImpactFrom EverandThe Nature of Drugs Vol. 2: History, Pharmacology, and Social ImpactNo ratings yet
- Handbook of Formulating Dermal Applications: A Definitive Practical GuideFrom EverandHandbook of Formulating Dermal Applications: A Definitive Practical GuideNo ratings yet
- An Introduction to the Periodic Table of Elements : Chemistry Textbook Grade 8 | Children's Chemistry BooksFrom EverandAn Introduction to the Periodic Table of Elements : Chemistry Textbook Grade 8 | Children's Chemistry BooksRating: 5 out of 5 stars5/5 (1)