You might also like
- Proximal Hamstring Tears: From Endoscopic Repair to Open ReconstructionFrom EverandProximal Hamstring Tears: From Endoscopic Repair to Open ReconstructionThomas YoumNo ratings yet
- (Iii) Extensor Tendon Injuries: Mini-Symposium: Hand InjuriesDocument5 pages(Iii) Extensor Tendon Injuries: Mini-Symposium: Hand InjuriesAndre MaharadjaNo ratings yet
- Flexor Tendon Injury of Hand and Its ReconstructionDocument3 pagesFlexor Tendon Injury of Hand and Its ReconstructionTeja LaksanaNo ratings yet
- Interphalangeal Joint (Hand Complex)Document6 pagesInterphalangeal Joint (Hand Complex)VIRESH VNo ratings yet
- Current Methods and Biomechanics of Extensor Tendon RepairDocument8 pagesCurrent Methods and Biomechanics of Extensor Tendon RepairMiguel Angel Lamas RamirezNo ratings yet
- Currentmethodsand Biomechanicsofextensor Tendonrepairs: Christopher J. Dy,, Lauren Rosenblatt,, Steve K. LeeDocument8 pagesCurrentmethodsand Biomechanicsofextensor Tendonrepairs: Christopher J. Dy,, Lauren Rosenblatt,, Steve K. LeeMiguel Angel Lamas RamirezNo ratings yet
- Lesiones Extensores PDFDocument8 pagesLesiones Extensores PDFJames Carvajal AcostaNo ratings yet
- Jathtrain00002 0050Document11 pagesJathtrain00002 0050NeerajNo ratings yet
- Biomechanics of Mallet Finger A Case ReportDocument4 pagesBiomechanics of Mallet Finger A Case ReportAkbar GazaliNo ratings yet
- Elbow and Antebrachium NotesDocument8 pagesElbow and Antebrachium NoteschadNo ratings yet
- Hand Injuries & Their ManagementsDocument78 pagesHand Injuries & Their ManagementsKuruNo ratings yet
- Posttraumatic Boutonniere and Swan Neck Deformities Mckeon2015Document10 pagesPosttraumatic Boutonniere and Swan Neck Deformities Mckeon2015yerec51683No ratings yet
- Prometric ReviewerDocument134 pagesPrometric ReviewerWilyam SerilNo ratings yet
- Surgical Exposure of The Flexor Pollicis Longus Tendon - Julian M. BrunetDocument5 pagesSurgical Exposure of The Flexor Pollicis Longus Tendon - Julian M. BrunetTeja LaksanaNo ratings yet
- 1-1 Anatomie Des Extenseurs Des Doigts LongsDocument20 pages1-1 Anatomie Des Extenseurs Des Doigts LongsProfesseur Christian DumontierNo ratings yet
- Ulnar Nerve Examination For Ulnar Nerve PalsyDocument14 pagesUlnar Nerve Examination For Ulnar Nerve Palsyalimran MahmudNo ratings yet
- Temporomandibular Joint-Anatomy and Movement Disorders: ISSN: 2278 - 0211 (Online)Document12 pagesTemporomandibular Joint-Anatomy and Movement Disorders: ISSN: 2278 - 0211 (Online)Krupali JainNo ratings yet
- Fibrous Flexor Sheath of the Fingers vFDocument6 pagesFibrous Flexor Sheath of the Fingers vFRichard DahildahilNo ratings yet
- Hand PDFDocument179 pagesHand PDFRadenSiwi Bagus HadhiningratNo ratings yet
- Management of Extensor Tendon Injuries: M. Griffin, S. Hindocha, D. Jordan, M. Saleh and W. KhanDocument7 pagesManagement of Extensor Tendon Injuries: M. Griffin, S. Hindocha, D. Jordan, M. Saleh and W. KhanAndre MaharadjaNo ratings yet
- The Structures of the HandDocument34 pagesThe Structures of the HandMichael SelvarajNo ratings yet
- Referat Claw and Club Hand: Ribka Theodora - Hand 3 Mentor: Dr. Betha Egih Riestiano, Spbp-ReDocument25 pagesReferat Claw and Club Hand: Ribka Theodora - Hand 3 Mentor: Dr. Betha Egih Riestiano, Spbp-ReRibka TheodoraNo ratings yet
- Wrist and HandDocument27 pagesWrist and Handtayestewart14No ratings yet
- GRDA Infratemporal FossaDocument10 pagesGRDA Infratemporal FossaKingNo ratings yet
- Examination of Hand & Common Hand InjuriesDocument165 pagesExamination of Hand & Common Hand InjuriesPriya GK100% (1)
- Anatomy of the Forearm, Wrist, and HandDocument66 pagesAnatomy of the Forearm, Wrist, and HandJoo Se HyukNo ratings yet
- The Radiology Assistant Shoulder - Rotator Cuff InjuryDocument1 pageThe Radiology Assistant Shoulder - Rotator Cuff InjuryKhalid Al maneiNo ratings yet
- Claw HandDocument54 pagesClaw HandArum MaharaniNo ratings yet
- DIPJ Denervation Arenas-PratDocument3 pagesDIPJ Denervation Arenas-PratanindyaNo ratings yet
- J Sart 2004 12 004Document7 pagesJ Sart 2004 12 004Fabio Sales VieiraNo ratings yet
- Wrist Drop Claw Hand Median Nerve Palsy: Dr. Srivatsa.NDocument46 pagesWrist Drop Claw Hand Median Nerve Palsy: Dr. Srivatsa.NMurali KarthikkNo ratings yet
- Radial Nerve PalsyDocument10 pagesRadial Nerve PalsyMahardika PutraNo ratings yet
- Lower Extremities 1Document27 pagesLower Extremities 1Abbas OmerNo ratings yet
- Lui 2007Document3 pagesLui 2007Minh ChíNo ratings yet
- Analgesia For Iliac Crest Bone GraftDocument9 pagesAnalgesia For Iliac Crest Bone GraftDominik Chirito PastorNo ratings yet
- 1-2 Anatomy-Biomechanics Extensor FESSHDocument45 pages1-2 Anatomy-Biomechanics Extensor FESSHProfesseur Christian Dumontier100% (1)
- Finger DeformitiesDocument42 pagesFinger DeformitiesYusufNo ratings yet
- The ElbowDocument10 pagesThe ElbowKatalinNo ratings yet
- Swan Neck DeformityDocument36 pagesSwan Neck Deformityn-gNo ratings yet
- Hand and Wrist WorkbookDocument16 pagesHand and Wrist WorkbookMarcos Perez AlbertNo ratings yet
- Fractures of The Distal Interphalangeal Joint: John D. Lubahn, MD and John M. Hood, MDDocument9 pagesFractures of The Distal Interphalangeal Joint: John D. Lubahn, MD and John M. Hood, MDArthur FranciscoNo ratings yet
- Essentials of Plastic SurgeryDocument12 pagesEssentials of Plastic SurgeryjoryadelmNo ratings yet
- 4 in 1 Quadricepsplasty For Fixed and Habitual DisDocument8 pages4 in 1 Quadricepsplasty For Fixed and Habitual DisMinh ChíNo ratings yet
- Pa Tho Physiology of AmputationDocument5 pagesPa Tho Physiology of AmputationMary Karen Rose BorjaNo ratings yet
- Forearm Osseofacial Compartments: Retinaculum Presented By: Amna NaveedDocument28 pagesForearm Osseofacial Compartments: Retinaculum Presented By: Amna NaveedHafizNo ratings yet
- Hand Anatomy: A. Hand Functions 1. TouchDocument10 pagesHand Anatomy: A. Hand Functions 1. Touchalis yakioNo ratings yet
- Loewenstein 2019Document9 pagesLoewenstein 2019Deborah SalinasNo ratings yet
- V1 PLCDocument18 pagesV1 PLCBartoszNo ratings yet
- Reoperation Rates After Fenestration For Lumbar Spinal Canal Stenosis: A 20-Year Period Survival Function Method AnalysisDocument7 pagesReoperation Rates After Fenestration For Lumbar Spinal Canal Stenosis: A 20-Year Period Survival Function Method AnalysisYusuf BrilliantNo ratings yet
- Peripheral Nerve Injuries c61Document69 pagesPeripheral Nerve Injuries c61Kevo YoungNo ratings yet
- Patella Osteotomy A New Approach For Complex Trauma Around The KneeDocument5 pagesPatella Osteotomy A New Approach For Complex Trauma Around The KneeToño Solano NogueraNo ratings yet
- Biomechanics and Pathomechanics of the HandDocument48 pagesBiomechanics and Pathomechanics of the HandShree PatelNo ratings yet
- Imaging The Infrapatellar Tendon in The Elite Athlete: K.A.L. Peace, J.C. Lee, J. HealyDocument9 pagesImaging The Infrapatellar Tendon in The Elite Athlete: K.A.L. Peace, J.C. Lee, J. HealytoaldoNo ratings yet
- The Leg: - Orthopedic Anatomy - Clinical Anatomy - Radiologic AnatomyDocument50 pagesThe Leg: - Orthopedic Anatomy - Clinical Anatomy - Radiologic Anatomyspeedy.catNo ratings yet
- 20-Hip, Knee & Ankle JointsDocument9 pages20-Hip, Knee & Ankle JointsKainat LatifNo ratings yet
- The Hand Complex NEWDocument11 pagesThe Hand Complex NEWVIRESH VNo ratings yet
- Applied Anatomy of The Wrist, Thumb and Hand: Joints, Joint Capsules and LigamentsDocument10 pagesApplied Anatomy of The Wrist, Thumb and Hand: Joints, Joint Capsules and LigamentsroyvillafrancaNo ratings yet
- 3-9 Anatomy Biomechanics ExtensorDocument31 pages3-9 Anatomy Biomechanics ExtensorProfesseur Christian DumontierNo ratings yet
- Repair Tendon FlexorDocument10 pagesRepair Tendon Flexorshera firanaNo ratings yet
- S0749806321003303Document20 pagesS0749806321003303Deborah SalinasNo ratings yet
- Smith 2011Document6 pagesSmith 2011Deborah SalinasNo ratings yet
- 10 1016@j Jhsa 2019 03 014Document6 pages10 1016@j Jhsa 2019 03 014Deborah SalinasNo ratings yet
- Helical 6-Strand Cruciate Tenorrhaphy: Description of A New Technique and Biomechanical Comparative Analysis With 2 Standard TechniquesDocument8 pagesHelical 6-Strand Cruciate Tenorrhaphy: Description of A New Technique and Biomechanical Comparative Analysis With 2 Standard TechniquesDeborah SalinasNo ratings yet
- 10 1016@j Jhsa 2020 08 001Document8 pages10 1016@j Jhsa 2020 08 001Deborah SalinasNo ratings yet
- Pone 0257038Document9 pagesPone 0257038Deborah SalinasNo ratings yet
- Fsurg 08 662720Document6 pagesFsurg 08 662720Deborah SalinasNo ratings yet
- Pi Is 0363502317301211Document8 pagesPi Is 0363502317301211Deborah SalinasNo ratings yet
- Fsurg 08 662720Document6 pagesFsurg 08 662720Deborah SalinasNo ratings yet
- HandbookNeurorehabilitation UnknownDocument195 pagesHandbookNeurorehabilitation UnknownDeborah SalinasNo ratings yet
- 10 1016@j Jhsa 2018 11 012Document5 pages10 1016@j Jhsa 2018 11 012Deborah SalinasNo ratings yet
- Early Breast Cancer ESMO Clinical Practice Guidelines For Diagnosis, Treatment and PDFDocument77 pagesEarly Breast Cancer ESMO Clinical Practice Guidelines For Diagnosis, Treatment and PDFDeborah SalinasNo ratings yet
- Chappell 2020Document9 pagesChappell 2020Deborah SalinasNo ratings yet
- Effects of Pulmonary Rehabilitation in Patients With Restrictive Lung DiseasesDocument7 pagesEffects of Pulmonary Rehabilitation in Patients With Restrictive Lung DiseasesDeborah SalinasNo ratings yet
- Pulmonary Rehabilitation in Patients With Idiopathic Pulmonary Fibrosis ReviewDocument11 pagesPulmonary Rehabilitation in Patients With Idiopathic Pulmonary Fibrosis ReviewDeborah SalinasNo ratings yet
- Effectiveness of Pulmonary Rehabilitation in Restrictive Lung DiseaseDocument7 pagesEffectiveness of Pulmonary Rehabilitation in Restrictive Lung DiseaseDeborah SalinasNo ratings yet
- Chronic Pain Assessment PDFDocument15 pagesChronic Pain Assessment PDFDeborah SalinasNo ratings yet
- Adaptacion Emocional de La Perdida de Una ExtremidadDocument22 pagesAdaptacion Emocional de La Perdida de Una ExtremidadDeborah SalinasNo ratings yet
- Gaitan 1 PDFDocument12 pagesGaitan 1 PDFDeborah SalinasNo ratings yet
- Home Exercise Program Is An Effective Tool Inimporving Upper Limb Function and Quality of Life in Breat Cancer SurvivoorDocument14 pagesHome Exercise Program Is An Effective Tool Inimporving Upper Limb Function and Quality of Life in Breat Cancer SurvivoorDeborah SalinasNo ratings yet
- Imporving Orientation in Head Injued Adults by Repeat Parctice Multisensory Input and Peer ParticipátionDocument10 pagesImporving Orientation in Head Injued Adults by Repeat Parctice Multisensory Input and Peer ParticipátionDeborah SalinasNo ratings yet
- CitoDocument10 pagesCitoMajo HGNo ratings yet
- Rehabilitation AmbulationDocument14 pagesRehabilitation AmbulationDeborah SalinasNo ratings yet
- Ambulation and Parkinson DiseaseDocument22 pagesAmbulation and Parkinson DiseaseDeborah SalinasNo ratings yet
- Multiple Sclerosis PDFDocument15 pagesMultiple Sclerosis PDFDeborah SalinasNo ratings yet
- AMBULATIONDocument12 pagesAMBULATIONDeborah SalinasNo ratings yet
- Ambulation Spin Cord InjuryDocument16 pagesAmbulation Spin Cord InjuryDeborah SalinasNo ratings yet
- Assistive Devices For AmbulationDocument13 pagesAssistive Devices For AmbulationDeborah Salinas100% (1)
- Falls, Aging and Disability PDFDocument17 pagesFalls, Aging and Disability PDFDeborah SalinasNo ratings yet
- Postural Assessment SheetsDocument2 pagesPostural Assessment SheetsFebryLasantiNo ratings yet
- Reverse Lunge With Single-Arm Kettlebell Overhead PressDocument5 pagesReverse Lunge With Single-Arm Kettlebell Overhead PressSheril MarekNo ratings yet
- ACL ExplainedDocument52 pagesACL ExplainedBalamurugan jayakumarNo ratings yet
- Myofascial LinesDocument14 pagesMyofascial Lineskabshiel100% (2)
- Genovarum and GenovalgumDocument7 pagesGenovarum and GenovalgumVerli Fajriati NofliNo ratings yet
- Types of Joints in the Human BodyDocument11 pagesTypes of Joints in the Human BodyCelina NassarNo ratings yet
- Range of Joint Motion Evaluation Chart OK PDFDocument2 pagesRange of Joint Motion Evaluation Chart OK PDFcesamav100% (4)
- Movement Phase 1 4Document5 pagesMovement Phase 1 4Matt Siniscalchi100% (1)
- Elbow Complex (Kinesiology)Document2 pagesElbow Complex (Kinesiology)Kimmybee Garcia50% (2)
- Hybrid Workout P90x/insanityDocument3 pagesHybrid Workout P90x/insanityVelagarza92100% (1)
- Arthroscopic Partial Medial MeniscectomyDocument6 pagesArthroscopic Partial Medial MeniscectomyLucas CifuentesNo ratings yet
- Zebis (2012) Kettlebell Swing Targets Semitendinosus and Supine Leg Curl Targets Biceps Femoris - An EMG Study With Rehabilitation ImplicationsDocument8 pagesZebis (2012) Kettlebell Swing Targets Semitendinosus and Supine Leg Curl Targets Biceps Femoris - An EMG Study With Rehabilitation ImplicationsJuan PalomoNo ratings yet
- Crack The Core Exam - Volume 2 4th PDFDocument508 pagesCrack The Core Exam - Volume 2 4th PDFQuỳnh Trâm86% (7)
- 12 Oktober 2017 - Swan Neck Deformity Vs BoutonniereDocument48 pages12 Oktober 2017 - Swan Neck Deformity Vs BoutonniereGerard BennyNo ratings yet
- وضعيات التصوير الشعاعي 1Document30 pagesوضعيات التصوير الشعاعي 1عبدالرحمن الاريانيNo ratings yet
- Orthopaedic Intruments and Surgeries: DR Tejasvi Agarwal Senior Resident Dept of OrthopaedicsDocument43 pagesOrthopaedic Intruments and Surgeries: DR Tejasvi Agarwal Senior Resident Dept of OrthopaedicsKapil LakhwaraNo ratings yet
- Elbow ExaminationelDocument3 pagesElbow ExaminationelAboud AbbassiNo ratings yet
- Scapular Syndromes HODocument25 pagesScapular Syndromes HOsnbtx7y79sNo ratings yet
- Reverse Total Shoulder Replacement Post-Operative Rehabilitation ProgramDocument3 pagesReverse Total Shoulder Replacement Post-Operative Rehabilitation Programdr_finch511No ratings yet
- The Masculoskeletal System & Tissue MechanicsDocument29 pagesThe Masculoskeletal System & Tissue MechanicsEdara Rajesh KumarNo ratings yet
- Referat Claw and Club Hand: Ribka Theodora - Hand 3 Mentor: Dr. Betha Egih Riestiano, Spbp-ReDocument25 pagesReferat Claw and Club Hand: Ribka Theodora - Hand 3 Mentor: Dr. Betha Egih Riestiano, Spbp-ReRibka TheodoraNo ratings yet
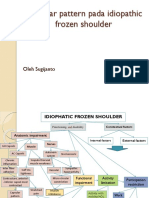
- Capsular pattern identification in idiopathic frozen shoulderDocument11 pagesCapsular pattern identification in idiopathic frozen shoulderRhany JulyatiNo ratings yet
- 9-Axillary & Median NerveDocument20 pages9-Axillary & Median NerveOxigen XenonNo ratings yet
- Joints and Body MovementsDocument4 pagesJoints and Body MovementsKyle Vincent PulaNo ratings yet
- Genanat D&R AgamDocument51 pagesGenanat D&R AgamWitty GreenNo ratings yet
- Lab 9 Gross Anatomy of The Muscular SystemDocument13 pagesLab 9 Gross Anatomy of The Muscular SystemJohn Lawrence YbanezNo ratings yet
- Locomotor ExamDocument6 pagesLocomotor Exami can always make u smile :D100% (1)
- Orthopedic Assessment Tests Adv Standing Entrance ExamDocument3 pagesOrthopedic Assessment Tests Adv Standing Entrance ExamVahid KhaveNo ratings yet
- Elbow Joint CHP 10 PDFDocument42 pagesElbow Joint CHP 10 PDFAlfionita WikaNo ratings yet
- Fitness Evaluation of the HorseFrom EverandFitness Evaluation of the HorseRating: 5 out of 5 stars5/5 (1)
- Hoof Physics: How to Recognize the Signs of Hoof DistortionFrom EverandHoof Physics: How to Recognize the Signs of Hoof DistortionRating: 5 out of 5 stars5/5 (1)
- Stable Relation: A Memoir of One Woman's Spirited Journey Home, by Way of the BarnFrom EverandStable Relation: A Memoir of One Woman's Spirited Journey Home, by Way of the BarnRating: 5 out of 5 stars5/5 (4)
- The Faraway Horses: The Adventures and Wisdom of America's Most Renowned HorsemenFrom EverandThe Faraway Horses: The Adventures and Wisdom of America's Most Renowned HorsemenRating: 4.5 out of 5 stars4.5/5 (49)
- The Everything Horse Book: Buying, riding, and caring for your equine companionFrom EverandThe Everything Horse Book: Buying, riding, and caring for your equine companionRating: 2 out of 5 stars2/5 (1)
- Horses: 101 Super Fun Facts and Amazing Pictures (Featuring The World's Top 18 Horse Breeds)From EverandHorses: 101 Super Fun Facts and Amazing Pictures (Featuring The World's Top 18 Horse Breeds)Rating: 3.5 out of 5 stars3.5/5 (11)
- Project Solomon: The True Story of a Lonely Horse Who Found a Home--and Became a HeroFrom EverandProject Solomon: The True Story of a Lonely Horse Who Found a Home--and Became a HeroRating: 5 out of 5 stars5/5 (9)
- The Everything Horse Care Book: A Complete Guide to the Well-being of Your HorseFrom EverandThe Everything Horse Care Book: A Complete Guide to the Well-being of Your HorseNo ratings yet
- The Equine Listenology Guide - Essential Horsemanship, Horse Body Language & Behaviour, Groundwork, In-hand Exercises & Riding Lessons to Develop Softness, Connection & Collection.From EverandThe Equine Listenology Guide - Essential Horsemanship, Horse Body Language & Behaviour, Groundwork, In-hand Exercises & Riding Lessons to Develop Softness, Connection & Collection.Rating: 5 out of 5 stars5/5 (1)
- 101 Fun Facts and Trivia About Horses: All You Need To Know If You Are Crazy About HorsesFrom Everand101 Fun Facts and Trivia About Horses: All You Need To Know If You Are Crazy About HorsesNo ratings yet
- Milo's Eyes: How a Blind Equestrian and Her "Seeing Eye Horse" Rescued Each OtherFrom EverandMilo's Eyes: How a Blind Equestrian and Her "Seeing Eye Horse" Rescued Each OtherRating: 5 out of 5 stars5/5 (2)
- Groundwork with horses: Natural Horsemanship & Groundwork Training for Your HorseFrom EverandGroundwork with horses: Natural Horsemanship & Groundwork Training for Your HorseNo ratings yet
- The Ultimate Book of Horse Bits: What They Are, What They Do, and How They Work (2nd Edition)From EverandThe Ultimate Book of Horse Bits: What They Are, What They Do, and How They Work (2nd Edition)Rating: 5 out of 5 stars5/5 (1)
- Whole Heart, Whole Horse: Building Trust Between Horse and RiderFrom EverandWhole Heart, Whole Horse: Building Trust Between Horse and RiderRating: 5 out of 5 stars5/5 (9)
- Cavaletti: Cavaletti horse training and groundwork with horsesFrom EverandCavaletti: Cavaletti horse training and groundwork with horsesNo ratings yet
- There's More to Training Horses: 100 Tips, 100 Days, 100% BetterFrom EverandThere's More to Training Horses: 100 Tips, 100 Days, 100% BetterNo ratings yet
- Horse training simply explained: Basic Horse training, Foal training, Natural Horsemanship and much moreFrom EverandHorse training simply explained: Basic Horse training, Foal training, Natural Horsemanship and much moreNo ratings yet
- Dressage Training and Competition Exercises for Beginners: Flatwork & Collection Schooling for HorsesFrom EverandDressage Training and Competition Exercises for Beginners: Flatwork & Collection Schooling for HorsesNo ratings yet