You might also like
- Evidence-Based LaryngologyFrom EverandEvidence-Based LaryngologyDavid E. RosowNo ratings yet
- Teaching The Neurological Examination in A Rapidly Evolving Clinical ClimateDocument13 pagesTeaching The Neurological Examination in A Rapidly Evolving Clinical Climatemh8m58brjnNo ratings yet
- Nxi 0000000000200168Document12 pagesNxi 0000000000200168Johanna ValentinaNo ratings yet
- 1 PBDocument6 pages1 PBAde Puji AstutiNo ratings yet
- Prognosis of Six-Month Functioning After Moderate To Severe Traumatic Brain Injury: A Systematic Review of Prospective Cohort StudiesDocument12 pagesPrognosis of Six-Month Functioning After Moderate To Severe Traumatic Brain Injury: A Systematic Review of Prospective Cohort StudiesYan Sheng HoNo ratings yet
- FOUR - Peds Manuscript REV Oct 21Document24 pagesFOUR - Peds Manuscript REV Oct 21Riandini Pramudita RNo ratings yet
- If It: ProblemDocument9 pagesIf It: ProblemMafe SanchezNo ratings yet
- JPSP - 2022 - 50Document11 pagesJPSP - 2022 - 50İpek OMURNo ratings yet
- A Systematic Review and Meta-Analysis of Risk 2022Document10 pagesA Systematic Review and Meta-Analysis of Risk 2022Claudia Mei Lan JaeNo ratings yet
- CNSexam PDFDocument8 pagesCNSexam PDFkarthiktsvmcNo ratings yet
- Van Midden Dorp 2013Document14 pagesVan Midden Dorp 2013Raveli KalvinNo ratings yet
- 00130478-202105000-00006 Serial Neurologic Assessment in Pediatrics (SNAP) : A New Tool For Bedside Neurologic Assessment of Critically Ill ChildrenDocument13 pages00130478-202105000-00006 Serial Neurologic Assessment in Pediatrics (SNAP) : A New Tool For Bedside Neurologic Assessment of Critically Ill ChildrenYo MeNo ratings yet
- Attention and Executive Functions in Microsurgically Treated Patients After Subarachnoid HemorrhageDocument6 pagesAttention and Executive Functions in Microsurgically Treated Patients After Subarachnoid HemorrhageDURRAH FARARESANo ratings yet
- Jurnal Clinical L OutcomeDocument14 pagesJurnal Clinical L OutcomeaesunnitheticNo ratings yet
- Management of The Undescended Testis in ChildrenDocument16 pagesManagement of The Undescended Testis in ChildrenRashmeeta ThadhaniNo ratings yet
- 2013 - Novak - Interventions For Children With CPDocument26 pages2013 - Novak - Interventions For Children With CPFriendlymeNo ratings yet
- ADNIannualchangebiomarkers clinicaloutcomeA&D10Document8 pagesADNIannualchangebiomarkers clinicaloutcomeA&D10brunoabramoffNo ratings yet
- A Real-Time FMRI Neurofeedback System For The Clinical Alleviation of Depression With A Subject-Independent Classification of Brain States A Proof of Principle StudyDocument12 pagesA Real-Time FMRI Neurofeedback System For The Clinical Alleviation of Depression With A Subject-Independent Classification of Brain States A Proof of Principle Studysiowan wongNo ratings yet
- BR J Sports Med-2008-Hegedus-80-92 PDFDocument14 pagesBR J Sports Med-2008-Hegedus-80-92 PDFAnonymous Jx2UvBeteNo ratings yet
- Machine LearningDocument11 pagesMachine LearningAlexNo ratings yet
- Sugammadex For Reversal of Rocuronium-Induced Neuromuscular Blockade in Pediatric PatientsDocument7 pagesSugammadex For Reversal of Rocuronium-Induced Neuromuscular Blockade in Pediatric PatientsAllonsiny GutierrezNo ratings yet
- Early Management of Spinal Cord Injury: WFNS Spine Committee RecommendationsDocument26 pagesEarly Management of Spinal Cord Injury: WFNS Spine Committee RecommendationsFernando Ruben Rivera CastilloNo ratings yet
- Aroojis 2019Document10 pagesAroojis 2019Irb azNo ratings yet
- Best Practice For Concussion Management: Carroll University Doctor of Physical Therapy Program Critically Appraised TopicDocument9 pagesBest Practice For Concussion Management: Carroll University Doctor of Physical Therapy Program Critically Appraised Topicapi-301127234No ratings yet
- Acupuncture in The Treatment of Abnormal Muscle Tone in Children With Cerebral Palsy: A Meta-AnalysisDocument11 pagesAcupuncture in The Treatment of Abnormal Muscle Tone in Children With Cerebral Palsy: A Meta-AnalysisrezteevicNo ratings yet
- Stem Cells Therapy in Cerebral Palsy: A Systematic ReviewDocument7 pagesStem Cells Therapy in Cerebral Palsy: A Systematic Reviewallyssa rahmadittaNo ratings yet
- A Meta-Analysis On Progressive Atrophy in Intractable Temporal Lobe EpilepsyDocument12 pagesA Meta-Analysis On Progressive Atrophy in Intractable Temporal Lobe EpilepsyBeny RiliantoNo ratings yet
- Evaluating The Impact of Evidence-Based Nursing inDocument3 pagesEvaluating The Impact of Evidence-Based Nursing inahmadalipoland25No ratings yet
- The Impact of Sealer Extrusion On Endodontic Outcome: A Systematic Review With Meta-AnalysisDocument7 pagesThe Impact of Sealer Extrusion On Endodontic Outcome: A Systematic Review With Meta-Analysisitsme543210No ratings yet
- Clinical Examination of Children With Cerebral PalsyDocument10 pagesClinical Examination of Children With Cerebral PalsyYogin PatelNo ratings yet
- Citicoline For Traumatic Brain Injury: A Systematic Review & Meta-AnalysisDocument10 pagesCiticoline For Traumatic Brain Injury: A Systematic Review & Meta-AnalysisAdria Putra FarhandikaNo ratings yet
- Novak2013 PDFDocument26 pagesNovak2013 PDFRifa YulitaNo ratings yet
- 2019 Article 5476Document10 pages2019 Article 5476Gaspar ContrerasNo ratings yet
- A Systematic Review of Treatments For Mild Traumatic Brain InjuryDocument3 pagesA Systematic Review of Treatments For Mild Traumatic Brain InjurySergio Machado NeurocientistaNo ratings yet
- Nihms 726255Document18 pagesNihms 726255Jem Rhod CamenseNo ratings yet
- Exercise and Sleep: A Systematic Review of Previous Meta-AnalysesDocument11 pagesExercise and Sleep: A Systematic Review of Previous Meta-AnalysesAlexPsrNo ratings yet
- A Study To Assess The Effectiveness of Structured Teaching Programme On Knowledge Regarding Kidney Transplantation Among ESRD Patients at Selected Hospitals at Mandya (Dist.)Document8 pagesA Study To Assess The Effectiveness of Structured Teaching Programme On Knowledge Regarding Kidney Transplantation Among ESRD Patients at Selected Hospitals at Mandya (Dist.)International Journal of Innovative Science and Research TechnologyNo ratings yet
- Official Position of The American Academy of Clinical Neuropsychology On Test SecurityDocument24 pagesOfficial Position of The American Academy of Clinical Neuropsychology On Test SecurityGustav RSRNo ratings yet
- (10920684 - Neurosurgical Focus) Informed Consent in Neurosurgery - A Systematic ReviewDocument10 pages(10920684 - Neurosurgical Focus) Informed Consent in Neurosurgery - A Systematic ReviewOnilis RiveraNo ratings yet
- Sci1301 1Document10 pagesSci1301 1Edwin Ade SaputraNo ratings yet
- Keperawatan Bencana Jurnal 3Document14 pagesKeperawatan Bencana Jurnal 3Fitriani HanifahNo ratings yet
- Medicina Basada en Evidencias - Artículo - Semana 13Document9 pagesMedicina Basada en Evidencias - Artículo - Semana 13gazaly garayNo ratings yet
- 1547 5654 Article p607Document10 pages1547 5654 Article p607wilsonwqaNo ratings yet
- Research Article CritiqueDocument8 pagesResearch Article Critiqueapi-654257930No ratings yet
- Factores CPPDocument7 pagesFactores CPPNoé Alejandro SánchezNo ratings yet
- Pharmaceutical Sciences: Cognitive Schemes For Clinical Diagnostic Reasoning by Medical StudentsDocument8 pagesPharmaceutical Sciences: Cognitive Schemes For Clinical Diagnostic Reasoning by Medical StudentsiajpsNo ratings yet
- Test-Retest Reliability of Remote Impact AdministrationDocument8 pagesTest-Retest Reliability of Remote Impact AdministrationMOHAMMAD HOLIP holipNo ratings yet
- Novack Etal2013Document43 pagesNovack Etal2013eebook123456No ratings yet
- Eye Tracking Metrics To Screen and Assess Cognitive Impairment in Patients With Neurological DisordersDocument8 pagesEye Tracking Metrics To Screen and Assess Cognitive Impairment in Patients With Neurological DisordersSyed Abdul Qadir GilaniNo ratings yet
- Medi 101 E29150 2 PDFDocument5 pagesMedi 101 E29150 2 PDFSam SamNo ratings yet
- E014478 FullDocument6 pagesE014478 FullГанбат М.No ratings yet
- Clinical Research Study Designs: The EssentialsDocument8 pagesClinical Research Study Designs: The EssentialsKanar MahmoodNo ratings yet
- Alyesha Proctor, Mark Lyttle, Jedd Billing, Pauline Shaw, Julian Simpson, Sarah Voss, Jonathan Richard BengerDocument13 pagesAlyesha Proctor, Mark Lyttle, Jedd Billing, Pauline Shaw, Julian Simpson, Sarah Voss, Jonathan Richard Bengerstardust.m002No ratings yet
- Epilepsy Duration and Seizure Outcome in Epilepsy Surgery: A Systematic Review and Meta-AnalysisDocument9 pagesEpilepsy Duration and Seizure Outcome in Epilepsy Surgery: A Systematic Review and Meta-Analysisbaba ababNo ratings yet
- Brolucizumab EstudioDocument13 pagesBrolucizumab EstudioJuan Carlos Mejía SernaNo ratings yet
- Clinical Neurology and Neurosurgery: Xuemei Zhang, Siheng Lian, Yingshi Zhang, Qingchun ZhaoDocument8 pagesClinical Neurology and Neurosurgery: Xuemei Zhang, Siheng Lian, Yingshi Zhang, Qingchun ZhaoLi LianNo ratings yet
- VNS EpilepsiaDocument3 pagesVNS EpilepsiaDiana Isabel ZeaNo ratings yet
- Neuromuscular Electrical Stimulation For Children With Dysphagia - A Systematic ReviewDocument11 pagesNeuromuscular Electrical Stimulation For Children With Dysphagia - A Systematic ReviewJaviera PalmaNo ratings yet
- Spinal Cord Injury: A Systematic Review of Current Treatment OptionsDocument10 pagesSpinal Cord Injury: A Systematic Review of Current Treatment OptionsEtika Tunjung KencanaNo ratings yet
- He Clinical Integrative Puzzle For Teaching and Assessing Clinical Reasoning Preliminary Feasibility, Reliability, and Validity EvidenceDocument7 pagesHe Clinical Integrative Puzzle For Teaching and Assessing Clinical Reasoning Preliminary Feasibility, Reliability, and Validity EvidenceFrederico PóvoaNo ratings yet
- Circular (24-2020) - EngDocument3 pagesCircular (24-2020) - EngdrnamithapedNo ratings yet
- Afp Case Investigation FormDocument3 pagesAfp Case Investigation Formአብይ በላይነሽ ጥላሁንNo ratings yet
- V G M For Allied Health Cbaa 1 5Document4 pagesV G M For Allied Health Cbaa 1 5Migz BolivarNo ratings yet
- Nausea and VomitingDocument3 pagesNausea and VomitingAlthea AlbaniaNo ratings yet
- Daftar Harga JuliDocument3 pagesDaftar Harga JuliRomandaniNo ratings yet
- Covid 19 PCR Test Results - JTH LAB - 2021.10.28 - For THJaffnaDocument2 pagesCovid 19 PCR Test Results - JTH LAB - 2021.10.28 - For THJaffnaArshathNo ratings yet
- CP-07 Workflow For Daycare Ambulatory CareDocument1 pageCP-07 Workflow For Daycare Ambulatory CareNatasha BhasinNo ratings yet
- ICRP 53 Radiation Dose To Patients From RadiofarmaceuticalsDocument387 pagesICRP 53 Radiation Dose To Patients From RadiofarmaceuticalsEduardo BuonoNo ratings yet
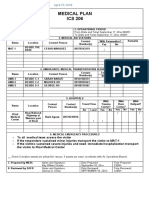
- Ics 206Document1 pageIcs 206Ldrrmo RamonNo ratings yet
- Generic Product ListDocument35 pagesGeneric Product Listangel cunananNo ratings yet
- Tugas EFN 1&2Document8 pagesTugas EFN 1&2Annisa DaniantiNo ratings yet
- Padmaja Devi - FEMALE - 62 Yrs APJ1.0013308310 1779459Document2 pagesPadmaja Devi - FEMALE - 62 Yrs APJ1.0013308310 1779459John DaveNo ratings yet
- Medical Writing Jobs - EssayDocument1 pageMedical Writing Jobs - EssayRoselily Flores CoquillaNo ratings yet
- SOP For Personnel Gowning QualificationDocument3 pagesSOP For Personnel Gowning QualificationSunil Murkikar (GM - PMI Quality Operations)100% (1)
- Denial Codes 05aug2020Document9 pagesDenial Codes 05aug2020naharmampillyNo ratings yet
- GRP4Integrated Application Form XLSX FormatDocument15 pagesGRP4Integrated Application Form XLSX FormatIsabel PeraltaNo ratings yet
- Rangs Childrens Fractures (3rd Edition) PDFDocument326 pagesRangs Childrens Fractures (3rd Edition) PDFairbear1115No ratings yet
- City of Plantation Vaccination Policy MemoDocument3 pagesCity of Plantation Vaccination Policy MemoAmanda Rojas100% (1)
- Peritonitis Et Causa Demam Typhoid: Kelompok D6Document21 pagesPeritonitis Et Causa Demam Typhoid: Kelompok D6Anjas PrabowoNo ratings yet
- Laporan Registrasi Pasien by ShiftDocument8 pagesLaporan Registrasi Pasien by ShiftDewi DayuntariNo ratings yet
- RMA HP Footprint 02.02.2021 NamibiaDocument14 pagesRMA HP Footprint 02.02.2021 NamibiaPerera KusalNo ratings yet
- Se MeritDocument200 pagesSe MeritShlok RathodNo ratings yet
- Narcolarm, Inc. (A) : The Crimson Press Curriculum Center The Crimson Group, IncDocument2 pagesNarcolarm, Inc. (A) : The Crimson Press Curriculum Center The Crimson Group, IncNitin GautamNo ratings yet
- Is Iso 10555 1 1995Document21 pagesIs Iso 10555 1 1995Hemant SharmaNo ratings yet
- Gambaran Kejadian Medication Error Di Instalasi Gawat Darurat Rsu Elim RantepaoDocument7 pagesGambaran Kejadian Medication Error Di Instalasi Gawat Darurat Rsu Elim RantepaoRahmi Eka PutriNo ratings yet
- African CultureDocument10 pagesAfrican CultureChelsy Allaine Dela CruzNo ratings yet
- Neuro DirectoryDocument142 pagesNeuro Directoryhazel tongsonNo ratings yet
- 75dda96a56832eb55b170518e36a9939Document89 pages75dda96a56832eb55b170518e36a9939Sagarika ChoudhuryNo ratings yet
- 15 Juni StockDocument11 pages15 Juni StockLalu EyiqNo ratings yet
- Bonneau Thomas Resume-2Document1 pageBonneau Thomas Resume-2api-510472433No ratings yet
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (23)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (80)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 4 out of 5 stars4/5 (5)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- Sleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningFrom EverandSleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningRating: 4 out of 5 stars4/5 (3)
- Gut: the new and revised Sunday Times bestsellerFrom EverandGut: the new and revised Sunday Times bestsellerRating: 4 out of 5 stars4/5 (392)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDFrom EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDRating: 5 out of 5 stars5/5 (1)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisFrom EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisRating: 3.5 out of 5 stars3.5/5 (2)
- An Autobiography of Trauma: A Healing JourneyFrom EverandAn Autobiography of Trauma: A Healing JourneyRating: 5 out of 5 stars5/5 (2)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Summary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisFrom EverandSummary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (9)
- 12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosFrom Everand12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosRating: 4.5 out of 5 stars4.5/5 (207)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)