You might also like
- Barangay Clearance SampleDocument2 pagesBarangay Clearance SampleIssan Villaruel92% (13)
- Indiabulls PILDocument64 pagesIndiabulls PILPGurus100% (1)
- Reso Change Signatories Brgy DaigDocument3 pagesReso Change Signatories Brgy DaigHeraiah Faith50% (2)
- Sample Brgy DTPDocument43 pagesSample Brgy DTPpagangpang galimuyod100% (19)
- December + Yearly ReviewDocument2 pagesDecember + Yearly ReviewNick FabrioNo ratings yet
- CERTIFICATION FormDocument1 pageCERTIFICATION FormSK TIMBANGANNo ratings yet
- Actual Occupany BlankDocument1 pageActual Occupany BlankBong RocoNo ratings yet
- 74 Indigency Form - 1Document11 pages74 Indigency Form - 1Metal WeebNo ratings yet
- Certification: Barangay CatininganDocument3 pagesCertification: Barangay CatininganArlanLaderasManhicNo ratings yet
- Barangay Baculanad: Republic of The Philippines Province of Leyte Municipality of Sta. FeDocument3 pagesBarangay Baculanad: Republic of The Philippines Province of Leyte Municipality of Sta. FeBarangay BaculanadNo ratings yet
- FormDocument1 pageFormPaulo SimNo ratings yet
- 74 Residency Form 1Document4 pages74 Residency Form 1Metal WeebNo ratings yet
- Certification DSWDDocument1 pageCertification DSWDcupisconnerapayao25No ratings yet
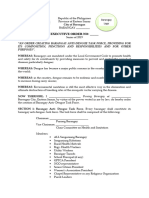
- Barangay Dengue Executive OrderDocument2 pagesBarangay Dengue Executive Orderbarangayg2023No ratings yet
- BPOC-Resolution Half NakedDocument5 pagesBPOC-Resolution Half NakedCath SanoNo ratings yet
- BSB FORM NO. 1 - Barangay Official's Information SheetDocument1 pageBSB FORM NO. 1 - Barangay Official's Information SheetRudejane Tan0% (1)
- MoaDocument11 pagesMoaanon-798485100% (1)
- Business 2020Document1 pageBusiness 2020Kristelle Anne Mae GayamatNo ratings yet
- Facility Based Delivery ResolutionDocument2 pagesFacility Based Delivery ResolutionGarik GarciaNo ratings yet
- Tanod and Lupon FormDocument1 pageTanod and Lupon FormdhEnz Jan100% (5)
- Application For Barangay Certification: First Time Jobseekers Personal Information Sheet FormDocument3 pagesApplication For Barangay Certification: First Time Jobseekers Personal Information Sheet FormDonavel Nodora Jojuico100% (3)
- Certificate of Indigency: Office of The Punong BarangayDocument3 pagesCertificate of Indigency: Office of The Punong BarangayDanmar CamilotNo ratings yet
- First Time Job SeekersDocument1 pageFirst Time Job SeekersNicolai Andrei RodriguezNo ratings yet
- Budget AIPDocument13 pagesBudget AIPAdona Besonia Concepcion SubongNo ratings yet
- Cert. Travel TRAVELDocument1 pageCert. Travel TRAVELNorie Cabilogan GarcesNo ratings yet
- Three Years Contingency Plan: Republic of The Philippines Province of Tarlac Municipality of MoncadaDocument24 pagesThree Years Contingency Plan: Republic of The Philippines Province of Tarlac Municipality of MoncadaRaziel Baldonado100% (1)
- Barangay Clearance BlankDocument1 pageBarangay Clearance BlankJeni LagahitNo ratings yet
- Barangay ClearanceDocument9 pagesBarangay Clearanceanon_910333265100% (1)
- Barangay Clearance: Republic of The Philippines Province of Nueva Ecija City of CabanatuanDocument1 pageBarangay Clearance: Republic of The Philippines Province of Nueva Ecija City of CabanatuanNarkSunder100% (1)
- Barangay ClearanceDocument2 pagesBarangay ClearanceBarangaySanLuisNo ratings yet
- Annexes A G I Templates For BarangayDocument8 pagesAnnexes A G I Templates For BarangayJeni LagahitNo ratings yet
- Bois SK BlankDocument1 pageBois SK BlankstimelindagalenoNo ratings yet
- Health Certificate New and Indigency NewDocument33 pagesHealth Certificate New and Indigency NewBarangay can-abujonNo ratings yet
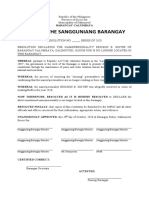
- Office of The Sangguniang BarangayDocument2 pagesOffice of The Sangguniang Barangayleo Bacuaden100% (8)
- No Work No Pay CertificationDocument1 pageNo Work No Pay CertificationJervel GuanzonNo ratings yet
- BDC Reso 01Document3 pagesBDC Reso 01Joseph Sumaoy100% (1)
- AGREEMEN1Document6 pagesAGREEMEN1Babuu BabuuNo ratings yet
- Barangay ClearanceDocument1 pageBarangay ClearancejaphethNo ratings yet
- Eo 1Document64 pagesEo 1Joan Real Baturiano100% (1)
- Certificate of Indigency-Barangay Social Services1Document1 pageCertificate of Indigency-Barangay Social Services1Joshua AssinNo ratings yet
- Resolution of AppointmentDocument3 pagesResolution of AppointmentFrancis Danver EmerzNo ratings yet
- 1% CPC Aip Res Tugbo '20Document1 page1% CPC Aip Res Tugbo '20Lito TiongNo ratings yet
- Aics OldDocument1 pageAics OldIBABA DEL SURNo ratings yet
- Disbursement Voucher DV NoDocument6 pagesDisbursement Voucher DV NoDelilah VillalobosNo ratings yet
- Brgy Clear 1st PageDocument1 pageBrgy Clear 1st PageJoshua Ray MananquilNo ratings yet
- Sample Brgy DTPDocument43 pagesSample Brgy DTPohm silvaNo ratings yet
- Barangay CertificationDocument1 pageBarangay CertificationReymar GallardoNo ratings yet
- RHU Various Sanitary FormsDocument5 pagesRHU Various Sanitary FormsJessa MaeNo ratings yet
- Fund TransferDocument2 pagesFund TransferMark anthony PranadaNo ratings yet
- Rbi Form ADocument1 pageRbi Form ARazel ArnuzaNo ratings yet
- Barangay EO Barangay Development CouncilDocument14 pagesBarangay EO Barangay Development CouncilPatrick Jorge Sibayan100% (23)
- BrgyresDocument1 pageBrgyresrandy-m-cadiente-4966No ratings yet
- CERTIFICATE of CommunityWorkService - 2023Document1 pageCERTIFICATE of CommunityWorkService - 2023Barangay CabulihanNo ratings yet
- Certificate of Residency Barangay ClearaDocument2 pagesCertificate of Residency Barangay ClearaRichelle Alejandro Ibea100% (1)
- Barangay PaligawanDocument3 pagesBarangay Paligawanbarangay paligawanNo ratings yet
- Memorandum of AgreementDocument2 pagesMemorandum of Agreementbhagzc khuya100% (1)
- Clearance: Office of The Punong BarangayDocument12 pagesClearance: Office of The Punong BarangayAuza JpNo ratings yet
- Cabaruyan Cert MasterlistDocument6 pagesCabaruyan Cert MasterlistRochelle UrbodaNo ratings yet
- Welcome to the Agrihood: Housing, Shopping, and Gardening for a Farm-to-Table LifestyleFrom EverandWelcome to the Agrihood: Housing, Shopping, and Gardening for a Farm-to-Table LifestyleNo ratings yet
- The backbone of Bangladesh’s development: Bangladesh's development: The challenges and ways of addressingFrom EverandThe backbone of Bangladesh’s development: Bangladesh's development: The challenges and ways of addressingNo ratings yet
- July 2021 Rao MooeDocument145 pagesJuly 2021 Rao MooeJeni LagahitNo ratings yet
- Coop Front FolderDocument1 pageCoop Front FolderJeni LagahitNo ratings yet
- Coop Cert MemberDocument1 pageCoop Cert MemberJeni LagahitNo ratings yet
- Ordinance STRAY DOGS AdlawanDocument2 pagesOrdinance STRAY DOGS AdlawanJeni LagahitNo ratings yet
- Columnar MarkingsDocument4 pagesColumnar MarkingsJeni LagahitNo ratings yet
- Cacao GrowersDocument2 pagesCacao GrowersJeni LagahitNo ratings yet
- Coop Attendance 2023 GaDocument1 pageCoop Attendance 2023 GaJeni LagahitNo ratings yet
- Coop Attendance 2023 GaDocument1 pageCoop Attendance 2023 GaJeni LagahitNo ratings yet
- Bcpc-Work-And-Financial-Plan TemplateDocument3 pagesBcpc-Work-And-Financial-Plan TemplateJeni Lagahit0% (1)
- Certificate of ResidencyDocument1 pageCertificate of ResidencyJeni LagahitNo ratings yet
- Brgy Health CenterDocument1 pageBrgy Health CenterJeni LagahitNo ratings yet
- BDRRM Accomplishment Report 2022Document1 pageBDRRM Accomplishment Report 2022Jeni Lagahit100% (1)
- Bapa 2Document11 pagesBapa 2Jeni LagahitNo ratings yet
- Property DigestDocument9 pagesProperty DigestJoy OrenaNo ratings yet
- Mystique-1 Shark Bay Block Diagram: Project Code: 91.4LY01.001 PCB (Raw Card) : 12298-2Document80 pagesMystique-1 Shark Bay Block Diagram: Project Code: 91.4LY01.001 PCB (Raw Card) : 12298-2Ion PetruscaNo ratings yet
- Agriculture Water Usage Poster ProjectDocument1 pageAgriculture Water Usage Poster Projectapi-339004071No ratings yet
- 21S18052 - Joshua Partogi Hutauruk - Review BUSNOV - Umbrella - WarsDocument5 pages21S18052 - Joshua Partogi Hutauruk - Review BUSNOV - Umbrella - WarsJoshua HutaurukNo ratings yet
- Optical Current TransformerDocument22 pagesOptical Current TransformerchallaramcharanreddyNo ratings yet
- Murugan Temple of North America: Ahkpuf F Gankd - FZGJP JizDocument8 pagesMurugan Temple of North America: Ahkpuf F Gankd - FZGJP JizOurMuruganTempleNo ratings yet
- Welcome To Our Presentation: Submitted byDocument30 pagesWelcome To Our Presentation: Submitted byShamim MridhaNo ratings yet
- Java 9 Real - TimeDocument57 pagesJava 9 Real - TimeDiego AmayaNo ratings yet
- User Mode I. System Support Processes: de Leon - Dolliente - Gayeta - Rondilla It201 - Platform Technology - TPDocument6 pagesUser Mode I. System Support Processes: de Leon - Dolliente - Gayeta - Rondilla It201 - Platform Technology - TPCariza DollienteNo ratings yet
- L8 Logistics ManagementDocument41 pagesL8 Logistics ManagementShahmien SevenNo ratings yet
- COURT CLERK NoticeDocument10 pagesCOURT CLERK NoticeED Curtis100% (3)
- MEMORIAL ON BEHALF OF APPELLANTS DocsDocument29 pagesMEMORIAL ON BEHALF OF APPELLANTS DocsPrashant KumarNo ratings yet
- FFA Test CHP INV and 16Document8 pagesFFA Test CHP INV and 16zainabNo ratings yet
- JSSG-2010-7 - Crash Systems Handbook PDFDocument155 pagesJSSG-2010-7 - Crash Systems Handbook PDFdaymonNo ratings yet
- METHODOLOG1Document3 pagesMETHODOLOG1Essa M RoshanNo ratings yet
- 2 FT Batch Recipe Editor User GuideDocument211 pages2 FT Batch Recipe Editor User GuideleandrovaffonsoNo ratings yet
- Snubbing PDFDocument134 pagesSnubbing PDFNavin SinghNo ratings yet
- Thoughts On Iphone Demand - Update On Delivery Times, Carrier IncentivesDocument10 pagesThoughts On Iphone Demand - Update On Delivery Times, Carrier Incentivesalpha123@tutopiaNo ratings yet
- Plewa2016 - Reputation in Higher Education: A Fuzzy Set Analysis of Resource ConfigurationsDocument9 pagesPlewa2016 - Reputation in Higher Education: A Fuzzy Set Analysis of Resource ConfigurationsAlice ChenNo ratings yet
- Create New Project CodeVision AVR (LED)Document5 pagesCreate New Project CodeVision AVR (LED)calvinNo ratings yet
- Lua ApiDocument176 pagesLua Apiyaotl albores tecuautzinNo ratings yet
- Shell Answer Book 07 The Driving Emergency BookDocument8 pagesShell Answer Book 07 The Driving Emergency BookKenneth100% (2)
- Queue Using Linked ListDocument2 pagesQueue Using Linked ListHassan ZiaNo ratings yet
- 8 - Surface Mining - Wire - RopeDocument11 pages8 - Surface Mining - Wire - RopeSuelen Barbosa Sdrill do BrasilNo ratings yet
- Economics: PAPER 1 Multiple ChoiceDocument12 pagesEconomics: PAPER 1 Multiple ChoiceigcsepapersNo ratings yet
- CHR Report 2017 IP Nat InquiryDocument30 pagesCHR Report 2017 IP Nat InquiryLeo Archival ImperialNo ratings yet
- Asmsc 1119 PDFDocument9 pagesAsmsc 1119 PDFAstha WadhwaNo ratings yet
- Hyperformance Plasma: Manual GasDocument272 pagesHyperformance Plasma: Manual GasSinan Aslan100% (1)