You might also like
- Osgood SlaterDocument5 pagesOsgood Slaterpruebaunodos123No ratings yet
- OsteotomyDocument4 pagesOsteotomyMihai DuduNo ratings yet
- Closing Wedge Osteotomy of The Tibia and The FemurDocument12 pagesClosing Wedge Osteotomy of The Tibia and The Femuralyek92No ratings yet
- Hip OsteotmyDocument4 pagesHip OsteotmyAhmed KeshkNo ratings yet
- Os 13 1465Document9 pagesOs 13 1465Mar HernandezNo ratings yet
- ArthroplastyDocument64 pagesArthroplastyAmit Kochhar75% (4)
- True Ponte Osteotomy Ponte 2018Document10 pagesTrue Ponte Osteotomy Ponte 2018Azmi FarhadiNo ratings yet
- 03 de RoeckDocument5 pages03 de RoeckAntonio FagaNo ratings yet
- Percutaneous Osteotomies in Pediatric Deformity Correction: Nickolas Nahm,, Louise Reid Boyce NicholsDocument16 pagesPercutaneous Osteotomies in Pediatric Deformity Correction: Nickolas Nahm,, Louise Reid Boyce NicholsAnonymous kdBDppigENo ratings yet
- Fixation of The Distal Tibiofibular Bone-Bridge in Transtibial Amputation PDFDocument4 pagesFixation of The Distal Tibiofibular Bone-Bridge in Transtibial Amputation PDFThomas BowersNo ratings yet
- (Literally "Re-Forming of Joint") : ArthroplastyDocument93 pages(Literally "Re-Forming of Joint") : ArthroplastykotraeNo ratings yet
- Kacnkkle KC L CqlkecDocument25 pagesKacnkkle KC L CqlkecLing101No ratings yet
- Solomon 2010Document10 pagesSolomon 2010Roger WatersNo ratings yet
- Presented By: DR Venkatesh V Moderator: DR Harish KDocument81 pagesPresented By: DR Venkatesh V Moderator: DR Harish KPankaj VatsaNo ratings yet
- Surgical Technique For Combined D Wyer Calcaneal Osteotomy and PeronealDocument6 pagesSurgical Technique For Combined D Wyer Calcaneal Osteotomy and PeronealleahbayNo ratings yet
- Use of Allograft in Skeletally Immature Patients For Calcaneal Neck Lengthening OsteotomyDocument5 pagesUse of Allograft in Skeletally Immature Patients For Calcaneal Neck Lengthening OsteotomyMonem ShakeerNo ratings yet
- Implant Selection in Revision Total Knee ArthroplastyDocument10 pagesImplant Selection in Revision Total Knee ArthroplastyAndrés KnubelNo ratings yet
- Cope Land Op TechDocument24 pagesCope Land Op Techsiddig7No ratings yet
- 10 1016@j Jos 2016 04 015Document7 pages10 1016@j Jos 2016 04 015osmann52No ratings yet
- Percutaneous Femoral Derotational Osteotomy For Excessive Femoral TorsionDocument7 pagesPercutaneous Femoral Derotational Osteotomy For Excessive Femoral TorsionDouglas PrinaNo ratings yet
- Osteotomies Jarthrodesis JDocument41 pagesOsteotomies Jarthrodesis Jdesire kbpNo ratings yet
- Pelvic Osteotomies in The Child and Young Adult Hip: Indications and Surgical TechniqueDocument8 pagesPelvic Osteotomies in The Child and Young Adult Hip: Indications and Surgical TechniqueLeonardo Guerrero CardozoNo ratings yet
- Arthroscopic Synovectomy of The Hip Joint: The Regional Surgical TechniqueDocument7 pagesArthroscopic Synovectomy of The Hip Joint: The Regional Surgical TechniqueMoustafa MohamedNo ratings yet
- Bleazey-2012-Recon of Complex Oc Lesions of The Talus With Cylindrical Sponge Allograft and Particulate Juvenile Cartilage GraftDocument7 pagesBleazey-2012-Recon of Complex Oc Lesions of The Talus With Cylindrical Sponge Allograft and Particulate Juvenile Cartilage Graftapi-212907483No ratings yet
- The Ertl Osteomyoplastic Amputation: History, Philosophy, Misconceptions, MisapplicationsDocument8 pagesThe Ertl Osteomyoplastic Amputation: History, Philosophy, Misconceptions, MisapplicationsanujNo ratings yet
- Total Knee Replacement Prosthesis AssignmentDocument33 pagesTotal Knee Replacement Prosthesis Assignmentdr neha gaggarNo ratings yet
- A Technical Tip To Treat The Intraoperative Lateral Cortex Fracture During A Medial Open Wedge High Tibial OsteotomyDocument5 pagesA Technical Tip To Treat The Intraoperative Lateral Cortex Fracture During A Medial Open Wedge High Tibial OsteotomyAthenaeum Scientific PublishersNo ratings yet
- Conferences and Reviews Total Hip Arthroplasty: or An A ReconDocument7 pagesConferences and Reviews Total Hip Arthroplasty: or An A ReconSekar CitrasariNo ratings yet
- Artigo ClamshellDocument15 pagesArtigo ClamshellbritocirurgiadamaoNo ratings yet
- Osteoarthritis of HipDocument3 pagesOsteoarthritis of Hipjcachica21No ratings yet
- Total Knee Arthroplasty in Osteopetrosis Using Patient-Specific InstrumentationDocument4 pagesTotal Knee Arthroplasty in Osteopetrosis Using Patient-Specific InstrumentationDavidBeatonComuladaNo ratings yet
- Ankle ArthrodesisDocument10 pagesAnkle ArthrodesisariearifinNo ratings yet
- Recurrent Dislocations and Complete NecrosisDocument11 pagesRecurrent Dislocations and Complete NecrosisDiegoNo ratings yet
- Combined Surgical-Orthodontic Treatment: How Did It Evolve and What Are The Best Practices Now?Document11 pagesCombined Surgical-Orthodontic Treatment: How Did It Evolve and What Are The Best Practices Now?tamkeen_farahNo ratings yet
- Spinal Osteotomies PDFDocument3 pagesSpinal Osteotomies PDFbandil deepanshuNo ratings yet
- Tratamiento No Convencional de ArtrosisDocument11 pagesTratamiento No Convencional de ArtrosisHenny CasanovaNo ratings yet
- Marcheggianimuccioli 2019Document12 pagesMarcheggianimuccioli 2019Ghusun MadaniNo ratings yet
- Orthodontically Driven Corticotomy: Tissue Engineering to Enhance Orthodontic and Multidisciplinary TreatmentFrom EverandOrthodontically Driven Corticotomy: Tissue Engineering to Enhance Orthodontic and Multidisciplinary TreatmentFederico BrugnamiNo ratings yet
- Knee Joint ThesisDocument5 pagesKnee Joint Thesisamywashingtonpittsburgh100% (2)
- Proximal Femoral NewDocument34 pagesProximal Femoral NewHimanshu HemantNo ratings yet
- Hip AssessDocument6 pagesHip AssessAhmed SalmanNo ratings yet
- Chirurgia Piciorului ºi GlezneiDocument28 pagesChirurgia Piciorului ºi GlezneiAngela PascarNo ratings yet
- Simultaneous Bilateral Opening-Wedge High Tibial Osteotomy With Early Full Weight-Bearing ExerciseDocument8 pagesSimultaneous Bilateral Opening-Wedge High Tibial Osteotomy With Early Full Weight-Bearing Exercisepamelascortez.luanNo ratings yet
- Management of Incarcerating Pincer-Type Femoroacetabular Impingement With Hip Arthroscopy - Arthroscopy TechniquesDocument1 pageManagement of Incarcerating Pincer-Type Femoroacetabular Impingement With Hip Arthroscopy - Arthroscopy TechniquesNica ReyesNo ratings yet
- Chapter 19Document25 pagesChapter 19MuhammadMusa47No ratings yet
- Pes Cavus ....Document34 pagesPes Cavus ....Rupika Sodhi100% (2)
- JOHCD-Adult Orthodontics Versus Adolescent OrthodonticsDocument128 pagesJOHCD-Adult Orthodontics Versus Adolescent OrthodonticsMohamed FaragNo ratings yet
- Spinal Pedicle Subtraction Osteotomy For Fixed Sagittal Imbalance Patients. Hyun 2013Document8 pagesSpinal Pedicle Subtraction Osteotomy For Fixed Sagittal Imbalance Patients. Hyun 2013Arsène NtiniNo ratings yet
- Anatomy and Bio Mechanics of The KneeDocument15 pagesAnatomy and Bio Mechanics of The KneeaimanshalpyNo ratings yet
- Young KyunDocument6 pagesYoung Kyunodontologia uvNo ratings yet
- Journal of Orthopaedic Surgery and ResearchDocument6 pagesJournal of Orthopaedic Surgery and ResearchDewye SartikaNo ratings yet
- Anterolateral Ligament Reconstruction Technique An Anatomic BasedDocument5 pagesAnterolateral Ligament Reconstruction Technique An Anatomic BasedEmilio Eduardo ChoqueNo ratings yet
- A New Posterolateral Approach Without Fibula Osteotomy For The Treatment of Tibial Plateau FracturesDocument6 pagesA New Posterolateral Approach Without Fibula Osteotomy For The Treatment of Tibial Plateau FracturesEduardo GonzalezNo ratings yet
- ArthroereisisDocument28 pagesArthroereisisNate HensleyNo ratings yet
- Bone and Jont Surgery Engl2020Document86 pagesBone and Jont Surgery Engl2020Timbur IgorNo ratings yet
- Coste Et Al. - 1968 - Rheumatoid ForefootDocument2 pagesCoste Et Al. - 1968 - Rheumatoid ForefootYuki SATAKENo ratings yet
- Bio EssayDocument5 pagesBio EssayWeston MooreNo ratings yet
- Modified Osteotomy of Posterolateral Overhanging Part of The Trochanter Via Posterior Approach For HA An Anatomical StudyDocument8 pagesModified Osteotomy of Posterolateral Overhanging Part of The Trochanter Via Posterior Approach For HA An Anatomical StudyVALENTIN THOMASNo ratings yet
- Osteotomies For Bunionette Deformity: Lowell Weil JR,, Lowell Scott Weil SRDocument24 pagesOsteotomies For Bunionette Deformity: Lowell Weil JR,, Lowell Scott Weil SRMiguel Angel Palacios FloresNo ratings yet
- Anterior Cruciate Ligament Reconstruction: A Practical Surgical GuideFrom EverandAnterior Cruciate Ligament Reconstruction: A Practical Surgical GuideNo ratings yet
- Price: Pediatric Nursing, 10 Edition: Open Book Quizzes Chapter 10: Disorders of The ToddlerDocument2 pagesPrice: Pediatric Nursing, 10 Edition: Open Book Quizzes Chapter 10: Disorders of The ToddlermickjagerNo ratings yet
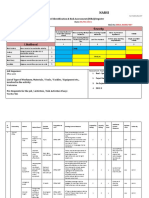
- Job Safety Analysis and Risk Assessment A Case Study of Frontier Ceramics LTDDocument13 pagesJob Safety Analysis and Risk Assessment A Case Study of Frontier Ceramics LTDaraaela 25No ratings yet
- Approach To Hip and Groin Pain in The Athlete and Active AdultDocument21 pagesApproach To Hip and Groin Pain in The Athlete and Active AdultAman DuggalNo ratings yet
- Knee ExaminationDocument5 pagesKnee ExaminationQandeelNo ratings yet
- HIRA NARSI Office AreaDocument3 pagesHIRA NARSI Office AreaNisanth ThulasidasNo ratings yet
- Biomechanics of The Shoulder ComplexDocument83 pagesBiomechanics of The Shoulder ComplexAdri An0% (1)
- Radial Nerve: Rajadurai R Crri, Orthopedics Ii Unit RGGGHDocument31 pagesRadial Nerve: Rajadurai R Crri, Orthopedics Ii Unit RGGGHrajaeasNo ratings yet
- Acute Respiratory Failure For StudentDocument41 pagesAcute Respiratory Failure For Studentapi-379952350% (4)
- Legion Porous CR 40830105 UsDocument16 pagesLegion Porous CR 40830105 UsSufyanNo ratings yet
- Review ATLS & Post TestDocument41 pagesReview ATLS & Post TestNugraha Arganda Ginting100% (2)
- Orthapedic Taping, Wrapping, and BracingDocument479 pagesOrthapedic Taping, Wrapping, and BracingJeffrey Conway-Jones67% (3)
- App Asst Loco PilotDocument339 pagesApp Asst Loco PilotHarithachandu86% (7)
- Deadlands Combat Guide PDFDocument2 pagesDeadlands Combat Guide PDFstryke99No ratings yet
- Silat Anatomy Course 09-Module3Document6 pagesSilat Anatomy Course 09-Module3Michael Paton100% (1)
- Trend t4Document23 pagesTrend t4blancofrank545No ratings yet
- Army Command TasksDocument20 pagesArmy Command TasksabkcomNo ratings yet
- Incident Reporting and Investigation PolicyDocument2 pagesIncident Reporting and Investigation PolicyNoor Muddassir KhanNo ratings yet
- Kneehab XP Instructions and UsageDocument16 pagesKneehab XP Instructions and UsageMVP Marketing and DesignNo ratings yet
- Diabetes MellitusDocument64 pagesDiabetes MellitusCris Tine67% (6)
- 2021 Rock Falls Little League Baseball Registration ApplicationDocument2 pages2021 Rock Falls Little League Baseball Registration ApplicationNeddie WattsNo ratings yet
- Structural Organisation in AnimalsDocument22 pagesStructural Organisation in AnimalsShiva PrabhakarNo ratings yet
- All American Operating Instructions For Non-Electric Pressure Steam Sterilizers Models 1915x, 1925x 1941xDocument24 pagesAll American Operating Instructions For Non-Electric Pressure Steam Sterilizers Models 1915x, 1925x 1941xSummer RaderNo ratings yet
- Fufen Bl-41: Bladder Channel 1Document1 pageFufen Bl-41: Bladder Channel 1BDI92No ratings yet
- Anatomy and Physiology For First AidersDocument19 pagesAnatomy and Physiology For First AidersRitakamal Bin Mohamad YunusNo ratings yet
- Fugl-Meyer Assessment Upper Extremity (Fma-Ue) Assessment of Sensorimotor FunctionDocument3 pagesFugl-Meyer Assessment Upper Extremity (Fma-Ue) Assessment of Sensorimotor FunctionFlorin MarinescuNo ratings yet
- Manual Unidades LRPDocument33 pagesManual Unidades LRPcarlos eduardo gutierrez gomezNo ratings yet
- The Female Pelvis Is Shorter and Wider Than The Male PelvisDocument2 pagesThe Female Pelvis Is Shorter and Wider Than The Male Pelvisarman gonzagaNo ratings yet
- Electrical Burn PDFDocument5 pagesElectrical Burn PDFsubbaiah54No ratings yet
- Defensive Line ManualDocument18 pagesDefensive Line Manualcanerican83100% (3)
- 6.blood Supply of Upper LimbDocument52 pages6.blood Supply of Upper LimbBlessed LoveNo ratings yet