You might also like
- Elif KI (2021) - Tibiotalocalcaneal Intramedullary Nailing For Unstable Geriatric Ankle FracturesDocument7 pagesElif KI (2021) - Tibiotalocalcaneal Intramedullary Nailing For Unstable Geriatric Ankle FracturesHariom ShuklaNo ratings yet
- Catastrophic Talar Bone Loss From High Velocity Trauma Treated With Structural Tricorticate Fibula Autograft Compression Frame and Midfoot Distraction ArthroplastyDocument9 pagesCatastrophic Talar Bone Loss From High Velocity Trauma Treated With Structural Tricorticate Fibula Autograft Compression Frame and Midfoot Distraction ArthroplastyAthenaeum Scientific PublishersNo ratings yet
- Osteogenesis InglesDocument4 pagesOsteogenesis InglesJulio TorresNo ratings yet
- Schlund 2019Document3 pagesSchlund 2019mesescuNo ratings yet
- Artigo ClamshellDocument15 pagesArtigo ClamshellbritocirurgiadamaoNo ratings yet
- Distraction Osteogenesis of The Maxillofacial Skeleton: Clinical and Radiological EvaluationDocument27 pagesDistraction Osteogenesis of The Maxillofacial Skeleton: Clinical and Radiological EvaluationDevata RaviNo ratings yet
- Management of Bone Defects in Primary Knee Arthroplasty: A Case ReportDocument4 pagesManagement of Bone Defects in Primary Knee Arthroplasty: A Case ReportInternational Journal of Recent Innovations in Academic ResearchNo ratings yet
- Manuscript ARMDocument11 pagesManuscript ARMMahardika PutraNo ratings yet
- Intramedullary Interlocking Nailing Versus Plating in Distal Tibial Shaft Fractures in Adults: A Comparative StudyDocument7 pagesIntramedullary Interlocking Nailing Versus Plating in Distal Tibial Shaft Fractures in Adults: A Comparative StudysidharthNo ratings yet
- Admin, Journal Manager, 08-GazzottiDocument9 pagesAdmin, Journal Manager, 08-GazzottistedorasNo ratings yet
- Transporte Oseo Postinfeccion en TibiaDocument7 pagesTransporte Oseo Postinfeccion en TibiaSusan Ly VillalobosNo ratings yet
- Clinical Application of Scaffolds For Cartilage Tissue EngineeringDocument17 pagesClinical Application of Scaffolds For Cartilage Tissue EngineeringikulNo ratings yet
- Distal Tibia Paper 2Document6 pagesDistal Tibia Paper 2Rajib DebnathNo ratings yet
- Articulo en Inglés 2Document8 pagesArticulo en Inglés 2Luis Ramirez BenaventeNo ratings yet
- Mandibulectomy PDFDocument4 pagesMandibulectomy PDFrekabiNo ratings yet
- Morbidity and Total Knee Arthroplasty As A Long Term Sequela of Tibial Plateau FracturesDocument8 pagesMorbidity and Total Knee Arthroplasty As A Long Term Sequela of Tibial Plateau FracturesAthenaeum Scientific PublishersNo ratings yet
- FAI.2007.0529Document7 pagesFAI.2007.0529milenabogojevskaNo ratings yet
- Ma 2021Document6 pagesMa 2021bigben9262No ratings yet
- Güven2013 Article MinimallyInvasiveOsteosynthesiDocument7 pagesGüven2013 Article MinimallyInvasiveOsteosynthesifebyan yohanesNo ratings yet
- Anehosur Et Al 2020 Concepts and Challenges in The Surgical Management of Edentulous Mandible Fractures A Case SeriesDocument7 pagesAnehosur Et Al 2020 Concepts and Challenges in The Surgical Management of Edentulous Mandible Fractures A Case SeriesHenry Adhy SantosoNo ratings yet
- Realignment Surgery For Malunited Ankle Fracture: Clinical ArticleDocument5 pagesRealignment Surgery For Malunited Ankle Fracture: Clinical ArticleGio VandaNo ratings yet
- Aps 39 345Document9 pagesAps 39 345isabelNo ratings yet
- Complications and Outcomes of The Transfibular Approach For Posterolateral Fractures of The Tibial Plateau PDFDocument19 pagesComplications and Outcomes of The Transfibular Approach For Posterolateral Fractures of The Tibial Plateau PDFSergio Tomas Cortés MoralesNo ratings yet
- Distal Humeral Fractures-Current Concepts PDFDocument11 pagesDistal Humeral Fractures-Current Concepts PDFRina AlvionitaNo ratings yet
- Fuhrmann 2002Document6 pagesFuhrmann 2002DentalErNo ratings yet
- Bleazey-2012-Recon of Complex Oc Lesions of The Talus With Cylindrical Sponge Allograft and Particulate Juvenile Cartilage GraftDocument7 pagesBleazey-2012-Recon of Complex Oc Lesions of The Talus With Cylindrical Sponge Allograft and Particulate Juvenile Cartilage Graftapi-212907483No ratings yet
- 13b Collagen 1Document7 pages13b Collagen 1María Fernanda EstévezNo ratings yet
- Ankle ArthrodesisDocument10 pagesAnkle ArthrodesisariearifinNo ratings yet
- Distraction Osteogenesis EbookDocument27 pagesDistraction Osteogenesis EbookSundeep SharmaNo ratings yet
- Journal of Orthopaedic Science: Hidenori Matsubara, Hiroyuki TsuchiyaDocument8 pagesJournal of Orthopaedic Science: Hidenori Matsubara, Hiroyuki TsuchiyaNeta Aza MaineztNo ratings yet
- Corticotomia Tunel AsistidoDocument7 pagesCorticotomia Tunel Asistidokatya Serrano LemusNo ratings yet
- Outcome Assesment of Proximal Fibular Osteotomy in Medial Compartment Knee OsteoarthritisDocument3 pagesOutcome Assesment of Proximal Fibular Osteotomy in Medial Compartment Knee OsteoarthritisPrashant GuptaNo ratings yet
- Raffaini Bioss CollagenDocument7 pagesRaffaini Bioss CollagenÂngelo Rosso LlantadaNo ratings yet
- Successful Outcome With Minimally Invasive Plate Osteosynthesis For Periprosthetic Tibial Fracture After Total Knee ArthroplastyDocument6 pagesSuccessful Outcome With Minimally Invasive Plate Osteosynthesis For Periprosthetic Tibial Fracture After Total Knee ArthroplastyMohebNo ratings yet
- Preliminary Report On A Staged Ridge Splitting Technique For Implant Placement in The Mandible: A Technical NoteDocument5 pagesPreliminary Report On A Staged Ridge Splitting Technique For Implant Placement in The Mandible: A Technical NoteSaurabh SatheNo ratings yet
- Stabilization of Distal Humerus Fractures by Precontoured Bi-Condylar Plating in A 90-90 PatternDocument5 pagesStabilization of Distal Humerus Fractures by Precontoured Bi-Condylar Plating in A 90-90 PatternmayNo ratings yet
- Neglected Intertrochanteric Fractures Treated With Valgus OsteotomyDocument4 pagesNeglected Intertrochanteric Fractures Treated With Valgus OsteotomyYashinta MaharaniNo ratings yet
- All-Epiphyseal, All-Inside Anterior Cruciate Ligament Reconstruction Technique For Skeletally Immature PatientsDocument9 pagesAll-Epiphyseal, All-Inside Anterior Cruciate Ligament Reconstruction Technique For Skeletally Immature Patientshieuminhduong7No ratings yet
- A Double-Plating Approach To Distal Femur Fracture. INJURY2017Document6 pagesA Double-Plating Approach To Distal Femur Fracture. INJURY2017Eduardo Gonzalez100% (1)
- Reconstrução de Severa Reabsorção Maxilar Com Distração OsteogenicaDocument7 pagesReconstrução de Severa Reabsorção Maxilar Com Distração OsteogenicaNelson UzunNo ratings yet
- Comminuted Intraarticular Fractures of The Tibial Plateau Lead To Posttraumatic Osteoarthritis of The Knee: Current Treatment ReviewDocument7 pagesComminuted Intraarticular Fractures of The Tibial Plateau Lead To Posttraumatic Osteoarthritis of The Knee: Current Treatment ReviewGustavoBecerraNo ratings yet
- The Effect of Conventional Surgery and Piezoelectric Surgery Bone Harvesting Techniques On The Donor Site Morbidity of The Mandibular Ramus and SymphysisDocument7 pagesThe Effect of Conventional Surgery and Piezoelectric Surgery Bone Harvesting Techniques On The Donor Site Morbidity of The Mandibular Ramus and SymphysisguhanderNo ratings yet
- Os 13 1465Document9 pagesOs 13 1465Mar HernandezNo ratings yet
- Iwanaga 2017Document5 pagesIwanaga 2017zj7n2rhtb4No ratings yet
- Split Technique 2Document8 pagesSplit Technique 2Alejandro RuizNo ratings yet
- Clinical Analysis of The Frosch Approach in The Treatment of Posterolateral Tibial Plateau Fractures Combined With Lateral Tibial Plateau FracturesDocument11 pagesClinical Analysis of The Frosch Approach in The Treatment of Posterolateral Tibial Plateau Fractures Combined With Lateral Tibial Plateau FracturesraynaldidjohariofcNo ratings yet
- Oh 2010Document5 pagesOh 2010gbaez.88No ratings yet
- Reconstruction of The Lateral Tibia Plateau Fracture With A Third Triangular Support Screw: A Biomechanical StudyDocument9 pagesReconstruction of The Lateral Tibia Plateau Fracture With A Third Triangular Support Screw: A Biomechanical StudyNorin FornaNo ratings yet
- Measurement of Bone Defects Adjacent To Acetabular Components of Hip ReplacementDocument9 pagesMeasurement of Bone Defects Adjacent To Acetabular Components of Hip Replacementehabede6445No ratings yet
- Use of Allograft in Skeletally Immature Patients For Calcaneal Neck Lengthening OsteotomyDocument5 pagesUse of Allograft in Skeletally Immature Patients For Calcaneal Neck Lengthening OsteotomyMonem ShakeerNo ratings yet
- Autologous Osteochondral Mosaicplasty For Osteochondritis Dissecans of The Elbow in Teenage AthletesDocument9 pagesAutologous Osteochondral Mosaicplasty For Osteochondritis Dissecans of The Elbow in Teenage AthletesAlejandro RamírezNo ratings yet
- Ortho ArticleDocument2 pagesOrtho ArticleSamantha Dela Paz100% (1)
- Primary Total Knee Arthroplasty For Acute Fracture Around The KneeDocument10 pagesPrimary Total Knee Arthroplasty For Acute Fracture Around The KneesaraNo ratings yet
- Intra-Articular Fractures of Distal Humerus Managed With Anatomic Pre-Contoured Plates Via Olecranon Osteotomy ApproachDocument7 pagesIntra-Articular Fractures of Distal Humerus Managed With Anatomic Pre-Contoured Plates Via Olecranon Osteotomy ApproachIJAR JOURNALNo ratings yet
- Novel Surgical Technique For Clavicle Graft HarvestDocument5 pagesNovel Surgical Technique For Clavicle Graft Harvestsanchaita kohliNo ratings yet
- Ams 5 108Document4 pagesAms 5 108Alice EmailsNo ratings yet
- Bilimsel Makale Cerrahi GirişimDocument3 pagesBilimsel Makale Cerrahi GirişimBelizNo ratings yet
- Treatment of Gonarthrosis by Total Knee ArthroplasDocument6 pagesTreatment of Gonarthrosis by Total Knee ArthroplasAhmad MaulanaNo ratings yet
- Prospective Study of Management of Close or CompouDocument5 pagesProspective Study of Management of Close or CompoumaudiaNo ratings yet
- Tips and Tricks for Problem Fractures, Volume I: The Upper ExtremityFrom EverandTips and Tricks for Problem Fractures, Volume I: The Upper ExtremityDaniel S. HorwitzNo ratings yet
- A Proposed Classification of Supracondylar FemurFractures Above Total Knee ArthroplastiesDocument4 pagesA Proposed Classification of Supracondylar FemurFractures Above Total Knee ArthroplastiesDavidBeatonComuladaNo ratings yet
- UE 1 Clavicle FracturesDocument46 pagesUE 1 Clavicle FracturesDavidBeatonComuladaNo ratings yet
- Synergy Hip System-SmallerDocument20 pagesSynergy Hip System-SmallerDavidBeatonComuladaNo ratings yet
- Vahedi2020 PDFDocument4 pagesVahedi2020 PDFDavidBeatonComuladaNo ratings yet
- Periprosthetic Fractures of The Proximal Femur Beyond The Vancouver ClassificationDocument8 pagesPeriprosthetic Fractures of The Proximal Femur Beyond The Vancouver ClassificationDavidBeatonComuladaNo ratings yet
- Osteoarthritis Associated With Osteopetrosis.30Document6 pagesOsteoarthritis Associated With Osteopetrosis.30DavidBeatonComuladaNo ratings yet
- Matching Nail Angle and Native Neck-Shaft AngleDocument4 pagesMatching Nail Angle and Native Neck-Shaft AngleDavidBeatonComuladaNo ratings yet
- Does Femoral Notching During Total Knee Arthroplasty Influence Periprosthetic Fracture. A Prospective StudyDocument6 pagesDoes Femoral Notching During Total Knee Arthroplasty Influence Periprosthetic Fracture. A Prospective StudyDavidBeatonComuladaNo ratings yet
- Basic Guitar Chords PDFDocument4 pagesBasic Guitar Chords PDFSamNo ratings yet
- The Reliability and Validity of The Vancouver Classification of Femoral Fractures After Hip ReplacementDocument4 pagesThe Reliability and Validity of The Vancouver Classification of Femoral Fractures After Hip ReplacementDavidBeatonComuladaNo ratings yet
- Total Joint Arthroplasty in Patients With Osteopetrosis: A Report of 5 Cases and Review of The LiteratureDocument6 pagesTotal Joint Arthroplasty in Patients With Osteopetrosis: A Report of 5 Cases and Review of The LiteratureDavidBeatonComuladaNo ratings yet
- Vanhove2014 PDFDocument5 pagesVanhove2014 PDFDavidBeatonComuladaNo ratings yet
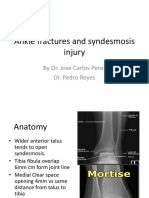
- Ankle fractures and syndesmosis injury treatment optionsDocument11 pagesAnkle fractures and syndesmosis injury treatment optionsDavidBeatonComuladaNo ratings yet
- Vahedi2020 PDFDocument4 pagesVahedi2020 PDFDavidBeatonComuladaNo ratings yet
- Hamilton 2014Document1 pageHamilton 2014DavidBeatonComuladaNo ratings yet
- Osteoarthritis and Osteopetrosis Treated by Knee ReplacementDocument6 pagesOsteoarthritis and Osteopetrosis Treated by Knee ReplacementDavidBeatonComuladaNo ratings yet
- Rheumatoid Hand and Wrist Surgery Soft Tissue.99323Document9 pagesRheumatoid Hand and Wrist Surgery Soft Tissue.99323DavidBeatonComuladaNo ratings yet
- Limb Length DiscrepancyDocument75 pagesLimb Length DiscrepancyDavidBeatonComuladaNo ratings yet
- Prosthetic Joint InfectionDocument21 pagesProsthetic Joint InfectionDavidBeatonComuladaNo ratings yet
- Intramedullary Nailing of Periarticular Fractures.2Document11 pagesIntramedullary Nailing of Periarticular Fractures.2DavidBeatonComuladaNo ratings yet
- Vanhove2014 PDFDocument5 pagesVanhove2014 PDFDavidBeatonComuladaNo ratings yet
- Primary TKA TechniqueDocument23 pagesPrimary TKA TechniqueDavidBeatonComuladaNo ratings yet
- Intramedullary Nailing of Femoral Shaft Fractures .4Document10 pagesIntramedullary Nailing of Femoral Shaft Fractures .4DavidBeatonComuladaNo ratings yet
- Vanhove2014 PDFDocument5 pagesVanhove2014 PDFDavidBeatonComuladaNo ratings yet
- Tendon Transfers For Radial, Median, and Ulnar Nerve Palsy: Review ArticleDocument10 pagesTendon Transfers For Radial, Median, and Ulnar Nerve Palsy: Review ArticleDavidBeatonComuladaNo ratings yet
- Vanhove2014 PDFDocument5 pagesVanhove2014 PDFDavidBeatonComuladaNo ratings yet
- Osteoarthritis Associated With Osteopetrosis.30Document6 pagesOsteoarthritis Associated With Osteopetrosis.30DavidBeatonComuladaNo ratings yet
- Skeletal System GuideDocument11 pagesSkeletal System GuideBryan JagroopNo ratings yet
- Knee Mechanics and Pathomechanics (1st Year)Document109 pagesKnee Mechanics and Pathomechanics (1st Year)MUGISHA GratienNo ratings yet
- 3 - Summary & MCQs PDFDocument6 pages3 - Summary & MCQs PDFSrinivas PingaliNo ratings yet
- SCLEROTHERAPYDocument439 pagesSCLEROTHERAPYVishal Gaikwad100% (2)
- Tashb CSDocument136 pagesTashb CSFaqRO100% (6)
- MANAGEMENT OF DISTAL RADIUS FRACTURESDocument98 pagesMANAGEMENT OF DISTAL RADIUS FRACTURESabhinavaiimsNo ratings yet
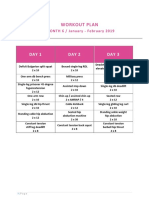
- BBB Month 6 Workout PlanDocument7 pagesBBB Month 6 Workout Planolle3870No ratings yet
- Shoulder Girdle Stretch StrengthenDocument4 pagesShoulder Girdle Stretch Strengthenapi-532952163No ratings yet
- Ukite 2010Document79 pagesUkite 2010pikacu196100% (2)
- Disorder of The Neuromuscular Junction: Courtesy . DR - Syeda Afsheen Hasnain DPT/MSPT NeuroloicalDocument16 pagesDisorder of The Neuromuscular Junction: Courtesy . DR - Syeda Afsheen Hasnain DPT/MSPT NeuroloicalCHANGEZ KHAN SARDAR100% (1)
- Artemis Hospital GurgaonDocument3 pagesArtemis Hospital GurgaonRashmi AgrawalNo ratings yet
- Test Bank For Bontragers Handbook of Radiographic Positioning and Techniques 9th Edition by LampignanoDocument24 pagesTest Bank For Bontragers Handbook of Radiographic Positioning and Techniques 9th Edition by LampignanoRebeccaLarsonqxsd100% (40)
- HyperarchFasciaTrainingGuide2022Document42 pagesHyperarchFasciaTrainingGuide2022tatuajev3No ratings yet
- Epidural NeuroplastyDocument13 pagesEpidural NeuroplastyadityakurniantoNo ratings yet
- 123 SIMM TutorialDocument2 pages123 SIMM Tutorialthanhr2411No ratings yet
- Assignment #1 Have An Advance Reading and Define The FollowingDocument6 pagesAssignment #1 Have An Advance Reading and Define The FollowingChan LeeNo ratings yet
- Master your upper/lower body split with Dr. Swole's summer programDocument2 pagesMaster your upper/lower body split with Dr. Swole's summer programMusadiq Ahmed100% (1)
- Nordic Musculoskeletal Questionnaire Form PDFDocument1 pageNordic Musculoskeletal Questionnaire Form PDFkhaista bacha100% (3)
- Trust Board: Board of Direction:: 9 No. 2 April - June 2015 Published Every 3 Month ISSN 1978 - 3744Document12 pagesTrust Board: Board of Direction:: 9 No. 2 April - June 2015 Published Every 3 Month ISSN 1978 - 3744febrian rahmatNo ratings yet
- Mri of Cervical Spine: Location: COLTONDocument3 pagesMri of Cervical Spine: Location: COLTONSusana FranklinNo ratings yet
- Swiss Ball Pike Ab WorkoutDocument9 pagesSwiss Ball Pike Ab WorkoutOana MozaNo ratings yet
- SpondylolisthesisDocument22 pagesSpondylolisthesisgonsteadtruth100% (3)
- Stew Smith - 6 Week Running PlanDocument15 pagesStew Smith - 6 Week Running PlanLuke Baumgartner100% (4)
- Diffuse Idiopathic Skeletal Hyperostosis (DISH) - StatPearls - NCBI BookshelfDocument7 pagesDiffuse Idiopathic Skeletal Hyperostosis (DISH) - StatPearls - NCBI BookshelfDavid Ithu AgkhuNo ratings yet
- Everything You Need to Know About GoniometryDocument57 pagesEverything You Need to Know About GoniometryNaveen Kumar100% (1)
- Spine Trauma - Dr. Didik Librianto, SpOT (K)Document65 pagesSpine Trauma - Dr. Didik Librianto, SpOT (K)Verty SalleNo ratings yet
- Organ Systems in the Human BodyDocument6 pagesOrgan Systems in the Human Bodycarmina duldulaoNo ratings yet
- PNF Techniques in The Upper ExtremityDocument27 pagesPNF Techniques in The Upper ExtremitysanalcrazyNo ratings yet
- Sacral Fractures: The Forgotten BoneDocument32 pagesSacral Fractures: The Forgotten BoneAkimuMagezaNo ratings yet
- White, M ( back)Document3 pagesWhite, M ( back)mnwhite1949No ratings yet