You might also like
- UE 1 Clavicle FracturesDocument46 pagesUE 1 Clavicle FracturesDavidBeatonComuladaNo ratings yet
- A Proposed Classification of Supracondylar FemurFractures Above Total Knee ArthroplastiesDocument4 pagesA Proposed Classification of Supracondylar FemurFractures Above Total Knee ArthroplastiesDavidBeatonComuladaNo ratings yet
- Matching Nail Angle and Native Neck-Shaft AngleDocument4 pagesMatching Nail Angle and Native Neck-Shaft AngleDavidBeatonComuladaNo ratings yet
- Synergy Hip System-SmallerDocument20 pagesSynergy Hip System-SmallerDavidBeatonComuladaNo ratings yet
- Does Femoral Notching During Total Knee Arthroplasty Influence Periprosthetic Fracture. A Prospective StudyDocument6 pagesDoes Femoral Notching During Total Knee Arthroplasty Influence Periprosthetic Fracture. A Prospective StudyDavidBeatonComuladaNo ratings yet
- Periprosthetic Fractures of The Proximal Femur Beyond The Vancouver ClassificationDocument8 pagesPeriprosthetic Fractures of The Proximal Femur Beyond The Vancouver ClassificationDavidBeatonComuladaNo ratings yet
- The Reliability and Validity of The Vancouver Classification of Femoral Fractures After Hip ReplacementDocument4 pagesThe Reliability and Validity of The Vancouver Classification of Femoral Fractures After Hip ReplacementDavidBeatonComuladaNo ratings yet
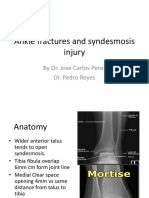
- Ankle fractures and syndesmosis injury treatment optionsDocument11 pagesAnkle fractures and syndesmosis injury treatment optionsDavidBeatonComuladaNo ratings yet
- Basic Guitar Chords PDFDocument4 pagesBasic Guitar Chords PDFSamNo ratings yet
- Total Knee Arthroplasty in Osteopetrosis Using Patient-Specific InstrumentationDocument4 pagesTotal Knee Arthroplasty in Osteopetrosis Using Patient-Specific InstrumentationDavidBeatonComuladaNo ratings yet
- Osteoarthritis and Osteopetrosis Treated by Knee ReplacementDocument6 pagesOsteoarthritis and Osteopetrosis Treated by Knee ReplacementDavidBeatonComuladaNo ratings yet
- Osteoarthritis Associated With Osteopetrosis.30Document6 pagesOsteoarthritis Associated With Osteopetrosis.30DavidBeatonComuladaNo ratings yet
- Vahedi2020 PDFDocument4 pagesVahedi2020 PDFDavidBeatonComuladaNo ratings yet
- Vahedi2020 PDFDocument4 pagesVahedi2020 PDFDavidBeatonComuladaNo ratings yet
- Intramedullary Nailing of Periarticular Fractures.2Document11 pagesIntramedullary Nailing of Periarticular Fractures.2DavidBeatonComuladaNo ratings yet
- Rheumatoid Hand and Wrist Surgery Soft Tissue.99323Document9 pagesRheumatoid Hand and Wrist Surgery Soft Tissue.99323DavidBeatonComuladaNo ratings yet
- Total Joint Arthroplasty in Patients With Osteopetrosis: A Report of 5 Cases and Review of The LiteratureDocument6 pagesTotal Joint Arthroplasty in Patients With Osteopetrosis: A Report of 5 Cases and Review of The LiteratureDavidBeatonComuladaNo ratings yet
- Intramedullary Nailing of Femoral Shaft Fractures .4Document10 pagesIntramedullary Nailing of Femoral Shaft Fractures .4DavidBeatonComuladaNo ratings yet
- Prosthetic Joint InfectionDocument21 pagesProsthetic Joint InfectionDavidBeatonComuladaNo ratings yet
- Hamilton 2014Document1 pageHamilton 2014DavidBeatonComuladaNo ratings yet
- Vanhove2014 PDFDocument5 pagesVanhove2014 PDFDavidBeatonComuladaNo ratings yet
- Vanhove2014 PDFDocument5 pagesVanhove2014 PDFDavidBeatonComuladaNo ratings yet
- Primary TKA TechniqueDocument23 pagesPrimary TKA TechniqueDavidBeatonComuladaNo ratings yet
- Vanhove2014 PDFDocument5 pagesVanhove2014 PDFDavidBeatonComuladaNo ratings yet
- Vanhove2014 PDFDocument5 pagesVanhove2014 PDFDavidBeatonComuladaNo ratings yet
- Limb Length DiscrepancyDocument75 pagesLimb Length DiscrepancyDavidBeatonComuladaNo ratings yet
- Osteoarthritis Associated With Osteopetrosis.30Document6 pagesOsteoarthritis Associated With Osteopetrosis.30DavidBeatonComuladaNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Lalpath Shruti ThrroidDocument2 pagesLalpath Shruti ThrroidSatish SrivastavaNo ratings yet
- Assignment 2Document2 pagesAssignment 2Rashida ParveenNo ratings yet
- Vasavi Diagnostic Laboratory: Church Road, Chitradurga - 577501Document2 pagesVasavi Diagnostic Laboratory: Church Road, Chitradurga - 577501Vidya kiranNo ratings yet
- Canvas Lab Exercise 12 Cardiovascular SystemDocument3 pagesCanvas Lab Exercise 12 Cardiovascular SystemJamesanne DemetriaNo ratings yet
- ANATOMY AND BIOMECHANICS OF WRIST JOINT FinalDocument43 pagesANATOMY AND BIOMECHANICS OF WRIST JOINT Finalinas ismailNo ratings yet
- HugeDocument36 pagesHugePupoko100% (2)
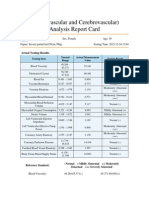
- Cardiovascular and CerebrovascularDocument6 pagesCardiovascular and CerebrovascularJoshelle B. Bancilo0% (1)
- Neuro 2 AnsDocument14 pagesNeuro 2 AnsSantiago AldayNo ratings yet
- How Animals SurviveDocument35 pagesHow Animals SurvivedhonaNo ratings yet
- Copy+of+AM+ +Frog+Dissection+ (Remote)Document21 pagesCopy+of+AM+ +Frog+Dissection+ (Remote)Khosraw HalimiNo ratings yet
- 10th Grade Fitness Assignment Sheet #3 PDFDocument6 pages10th Grade Fitness Assignment Sheet #3 PDFJohn JonesNo ratings yet
- 10 Simple Yoga Poses Height GainDocument11 pages10 Simple Yoga Poses Height GainRajesh GandikotaNo ratings yet
- Planes Systems OrganizationDocument36 pagesPlanes Systems OrganizationR. EssoNo ratings yet
- Activity 1Document3 pagesActivity 1Clarin Perez OrdinarioNo ratings yet
- Spontaneous Regression of Sequestrated Lumbar Disc Herniations - 2014Document6 pagesSpontaneous Regression of Sequestrated Lumbar Disc Herniations - 2014SNNo ratings yet
- Unit 2 Grandrounds Ot ListDocument2 pagesUnit 2 Grandrounds Ot ListBhavvNo ratings yet
- Making Occlusion 2Document7 pagesMaking Occlusion 2Ali QawasNo ratings yet
- Curs 10 MG AN I SEM IDocument34 pagesCurs 10 MG AN I SEM IRusu CristianaNo ratings yet
- Cranial Nerves TableDocument1 pageCranial Nerves TablePIOZRNo ratings yet
- The Slump Test: Examining Spinal Pain and Range of MotionDocument5 pagesThe Slump Test: Examining Spinal Pain and Range of MotionNahu SteinmannNo ratings yet
- Stanford DR Dake MRI MRV Protocol 1.5 TeslaDocument18 pagesStanford DR Dake MRI MRV Protocol 1.5 Teslamarky777100% (1)
- Gait Cycle - Foot & Ankle - OrthobulletsDocument6 pagesGait Cycle - Foot & Ankle - OrthobulletsBOOCOMETRUENo ratings yet
- Neurological Exam of Cats Made SimpleDocument6 pagesNeurological Exam of Cats Made SimplevetthamilNo ratings yet
- MakhaarijDocument18 pagesMakhaarijSalia SoumareNo ratings yet
- 1 The General Plan of PatientDocument7 pages1 The General Plan of PatientcorsairmdNo ratings yet
- Lecture 1 - Development of Respiratory SystemDocument27 pagesLecture 1 - Development of Respiratory SystemRachmad MusyaffaNo ratings yet
- Respiratory System ExplainedDocument6 pagesRespiratory System ExplainedPaulus Villanueva100% (1)
- Head and NeckDocument11 pagesHead and NeckdrsamnNo ratings yet
- Arm Diagram Left - Google Search PDFDocument1 pageArm Diagram Left - Google Search PDFjordanNo ratings yet
- DLL November 21, 2017 - Endocrine GlandsDocument4 pagesDLL November 21, 2017 - Endocrine GlandsHelen Grace Llemos Cabalag100% (2)