You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5814)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- 2Document36 pages2PYNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- H2 Maths Detailed SummaryDocument82 pagesH2 Maths Detailed SummarythatsparklexNo ratings yet
- Assignment #3 (Forecasting)Document10 pagesAssignment #3 (Forecasting)Mark Roger Huberit IINo ratings yet
- SPAN CSP Volume 2Document176 pagesSPAN CSP Volume 2samer alrawashdeh50% (2)
- PIIS0031395514001801Document2 pagesPIIS0031395514001801DavidBeatonComuladaNo ratings yet
- Synergy Hip System-SmallerDocument20 pagesSynergy Hip System-SmallerDavidBeatonComuladaNo ratings yet
- Periprosthetic Fractures of The Proximal Femur Beyond The Vancouver ClassificationDocument8 pagesPeriprosthetic Fractures of The Proximal Femur Beyond The Vancouver ClassificationDavidBeatonComuladaNo ratings yet
- UE 1 Clavicle FracturesDocument46 pagesUE 1 Clavicle FracturesDavidBeatonComuladaNo ratings yet
- Matching Nail Angle and Native Neck-Shaft AngleDocument4 pagesMatching Nail Angle and Native Neck-Shaft AngleDavidBeatonComuladaNo ratings yet
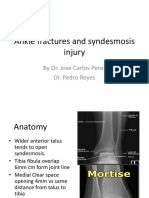
- Ankle Fractures and Syndesmosis Injury: by Dr. Jose Carlos Perez Dr. Pedro ReyesDocument11 pagesAnkle Fractures and Syndesmosis Injury: by Dr. Jose Carlos Perez Dr. Pedro ReyesDavidBeatonComuladaNo ratings yet
- Does Femoral Notching During Total Knee Arthroplasty Influence Periprosthetic Fracture. A Prospective StudyDocument6 pagesDoes Femoral Notching During Total Knee Arthroplasty Influence Periprosthetic Fracture. A Prospective StudyDavidBeatonComuladaNo ratings yet
- Total Knee Arthroplasty in Osteopetrosis Using Patient-Specific InstrumentationDocument4 pagesTotal Knee Arthroplasty in Osteopetrosis Using Patient-Specific InstrumentationDavidBeatonComuladaNo ratings yet
- Vahedi2020 PDFDocument4 pagesVahedi2020 PDFDavidBeatonComuladaNo ratings yet
- Total Joint Arthroplasty in Patients With Osteopetrosis: A Report of 5 Cases and Review of The LiteratureDocument6 pagesTotal Joint Arthroplasty in Patients With Osteopetrosis: A Report of 5 Cases and Review of The LiteratureDavidBeatonComuladaNo ratings yet
- Osteoarthritis Associated With Osteopetrosis.30Document6 pagesOsteoarthritis Associated With Osteopetrosis.30DavidBeatonComuladaNo ratings yet
- Hamilton 2014Document1 pageHamilton 2014DavidBeatonComuladaNo ratings yet
- Intramedullary Nailing of Femoral Shaft Fractures .4Document10 pagesIntramedullary Nailing of Femoral Shaft Fractures .4DavidBeatonComuladaNo ratings yet
- Rheumatoid Hand and Wrist Surgery Soft Tissue.99323Document9 pagesRheumatoid Hand and Wrist Surgery Soft Tissue.99323DavidBeatonComuladaNo ratings yet
- Vanhove2014 PDFDocument5 pagesVanhove2014 PDFDavidBeatonComuladaNo ratings yet
- Osteoarthritis Associated With Osteopetrosis.30Document6 pagesOsteoarthritis Associated With Osteopetrosis.30DavidBeatonComuladaNo ratings yet
- Emailing BHU Syllabus M.Sc.Document25 pagesEmailing BHU Syllabus M.Sc.Prateek NaikNo ratings yet
- A Novel Sample Design For Determining Color Compatibility Between Layered Resin Composite and Vita Shade GuidesDocument9 pagesA Novel Sample Design For Determining Color Compatibility Between Layered Resin Composite and Vita Shade GuidesNaoki MezarinaNo ratings yet
- 51940bos41633 p3qDocument16 pages51940bos41633 p3qJagpreet SinghNo ratings yet
- Resistance ManualDocument71 pagesResistance ManualDaniel Balan LangatNo ratings yet
- Global Vaccine Market Report: Executive SummaryDocument14 pagesGlobal Vaccine Market Report: Executive SummaryAntonio MoncayoNo ratings yet
- Language Motivation PDFDocument15 pagesLanguage Motivation PDFMa. Cassandra EspirituNo ratings yet
- HYSYS - Course EA1000 Advanced Process ModelingDocument210 pagesHYSYS - Course EA1000 Advanced Process Modelingnagymate0% (1)
- Calculating Correlation With ExcelDocument5 pagesCalculating Correlation With ExcelAadhar GilhotraNo ratings yet
- XtxtnbregDocument13 pagesXtxtnbregalicorpanaoNo ratings yet
- Project CharterDocument35 pagesProject CharterAndi AlibetoNo ratings yet
- 3b Features PDFDocument40 pages3b Features PDFjithuNo ratings yet
- A Study On Financial Literacy of Malaysian Degree Students PDFDocument9 pagesA Study On Financial Literacy of Malaysian Degree Students PDFbilalrafiqgaganNo ratings yet
- Fourth EditionDocument623 pagesFourth EditionPrince DeepNo ratings yet
- Hackston Dan Milne (1996) - Some - DeterminantsDocument32 pagesHackston Dan Milne (1996) - Some - DeterminantsRia BarusNo ratings yet
- Production, Modeling, and Education Egg Geometry Calculation Using The Measurements of Length and BreadthDocument3 pagesProduction, Modeling, and Education Egg Geometry Calculation Using The Measurements of Length and BreadthpriyaNo ratings yet
- PPRF Complete Research Report PDFDocument53 pagesPPRF Complete Research Report PDFGuillermo Bautista FuerteNo ratings yet
- Finkel 1Document24 pagesFinkel 1Manuel Ruiz-Huidobro VeraNo ratings yet
- Manual DS701MS 737MS 748 Eng OmDocument2 pagesManual DS701MS 737MS 748 Eng Om18847No ratings yet
- MBA Syllabus III SemesterDocument59 pagesMBA Syllabus III SemesterSharmilaNo ratings yet
- What Is The Difference Between Linear Regression and Multiple RegressionDocument4 pagesWhat Is The Difference Between Linear Regression and Multiple RegressionNaveed Ahmad100% (1)
- Effect of Profitability & Financial Leverage On Capital Structure A Case of Pakistan's Automobile IndustryDocument9 pagesEffect of Profitability & Financial Leverage On Capital Structure A Case of Pakistan's Automobile IndustryAhmed SiddNo ratings yet
- Phi-Coefficient: Conceptual ExplanationDocument130 pagesPhi-Coefficient: Conceptual ExplanationAj RosalNo ratings yet
- BSL 3 - 7 TutorialDocument41 pagesBSL 3 - 7 TutorialIndrė LapeikaitėNo ratings yet
- Amul WelfareDocument13 pagesAmul WelfareivaibhavworldNo ratings yet
- MultipotentialityDocument12 pagesMultipotentialityDeasElenaNicoletaNo ratings yet
- CorrelationDocument19 pagesCorrelationMarcus MedinaNo ratings yet