You might also like
- Basic Guitar Chords PDFDocument4 pagesBasic Guitar Chords PDFSamNo ratings yet
- Z Effect & Reverse Z Effect in PFNDocument7 pagesZ Effect & Reverse Z Effect in PFNNandan SurNo ratings yet
- Disaster P1examDocument9 pagesDisaster P1examJushua Opsima RuizNo ratings yet
- Homeopathic PracticeDocument313 pagesHomeopathic PracticeMarian Claudiu50% (2)
- Disorders of The Foot and Leg ConfDocument304 pagesDisorders of The Foot and Leg ConfhaminatrafNo ratings yet
- Pediatric OSCE A Guide For Medical StudentsDocument9 pagesPediatric OSCE A Guide For Medical Studentsjoey92leeNo ratings yet
- Breast Examination - ADocument30 pagesBreast Examination - AAkash VermaNo ratings yet
- Test 1 Science Form 3Document7 pagesTest 1 Science Form 3Zunaizah Yahaya100% (1)
- HypospadiaDocument21 pagesHypospadiaShi YunNo ratings yet
- Vanhove2014 PDFDocument5 pagesVanhove2014 PDFDavidBeatonComuladaNo ratings yet
- Osteomielitis PatelarDocument3 pagesOsteomielitis PatelarAlexander DanielNo ratings yet
- Rizqi Anang Anandito - P1337430118023 - Tugas Epidemiologi TM 8Document7 pagesRizqi Anang Anandito - P1337430118023 - Tugas Epidemiologi TM 8Par zivalNo ratings yet
- Patellar Tendon Avulsion With Tibial Tuberosity SLDocument4 pagesPatellar Tendon Avulsion With Tibial Tuberosity SLKirana ArinNo ratings yet
- A Case Report Treatment of A Medial Condylar Humeral Fracture in An Adult With Osteopetrosis - (Author Calvin Chien)Document3 pagesA Case Report Treatment of A Medial Condylar Humeral Fracture in An Adult With Osteopetrosis - (Author Calvin Chien)The Internet Medical JournalNo ratings yet
- Iatrogenic Vertebral Fracture During Intramedullary Nailing For Femoral FractureDocument8 pagesIatrogenic Vertebral Fracture During Intramedullary Nailing For Femoral FractureCristian ZepitaNo ratings yet
- Osteopathia Striata With Concomitant Fibroblastic Osteosarcoma of The Femur A Potential Malignant Risk 2472 016X 1000104Document4 pagesOsteopathia Striata With Concomitant Fibroblastic Osteosarcoma of The Femur A Potential Malignant Risk 2472 016X 1000104ritvikNo ratings yet
- Fulltext - Smjo v3 1059Document3 pagesFulltext - Smjo v3 1059Rachell AchellNo ratings yet
- Gorham's Disease of Spine: Sian Pine OurnalDocument6 pagesGorham's Disease of Spine: Sian Pine OurnalGermán PulidoNo ratings yet
- Total Knee Arthroplasty in Osteopetrosis Using Patient-Specific InstrumentationDocument4 pagesTotal Knee Arthroplasty in Osteopetrosis Using Patient-Specific InstrumentationDavidBeatonComuladaNo ratings yet
- FASJ - 2017 - Zwiers - Rare Causeof Lateral Ankle Pain - Symptomatic Talus Secundarius - Case ReportDocument5 pagesFASJ - 2017 - Zwiers - Rare Causeof Lateral Ankle Pain - Symptomatic Talus Secundarius - Case ReportJacob DoughertyNo ratings yet
- Bilateral Peroneal Tubercle Osteochondroma of The Calcaneus: CaseDocument3 pagesBilateral Peroneal Tubercle Osteochondroma of The Calcaneus: CaseAntony CevallosNo ratings yet
- 1982 4378 Rbort 54 06 0736Document3 pages1982 4378 Rbort 54 06 0736azevedoNo ratings yet
- Acutrak Fixation of Comminuted Distal Radial FracturesDocument4 pagesAcutrak Fixation of Comminuted Distal Radial Fracturessanjay chhawraNo ratings yet
- Case ReportDocument3 pagesCase Reportandrul556723No ratings yet
- Painful Knee 2024 International Journal of Surgery Case ReportsDocument6 pagesPainful Knee 2024 International Journal of Surgery Case ReportsRonald QuezadaNo ratings yet
- H Rotating-Hinge Total Knee Arthroplasty in A Patient With Genu Recurvatum After Osteomyelitis of The Distal FemurDocument4 pagesH Rotating-Hinge Total Knee Arthroplasty in A Patient With Genu Recurvatum After Osteomyelitis of The Distal FemurYuji AibNo ratings yet
- Fibrous Dysplasia of The Thoracic Spine: SciencedirectDocument5 pagesFibrous Dysplasia of The Thoracic Spine: SciencedirectRisang Nur WigunaNo ratings yet
- Percutaneous Femoral Derotational Osteotomy For Excessive Femoral TorsionDocument7 pagesPercutaneous Femoral Derotational Osteotomy For Excessive Femoral TorsionDouglas PrinaNo ratings yet
- Kelly 2003Document18 pagesKelly 2003leidy-riverosNo ratings yet
- The Ertl Osteomyoplastic Amputation: History, Philosophy, Misconceptions, MisapplicationsDocument8 pagesThe Ertl Osteomyoplastic Amputation: History, Philosophy, Misconceptions, MisapplicationsanujNo ratings yet
- Resección en síndrome de bertolottiDocument4 pagesResección en síndrome de bertolottiOscar Cayetano Herrera RodríguezNo ratings yet
- AAOS2001 ReconstructionDocument58 pagesAAOS2001 ReconstructionHéctor Pando SánchezNo ratings yet
- Bru10319 FM PDFDocument6 pagesBru10319 FM PDFR HariNo ratings yet
- Freibergs Infraction of The Second Metatarsal Head With Bioorthologic Repair Using The Nexa Osteocure Bone GraftDocument9 pagesFreibergs Infraction of The Second Metatarsal Head With Bioorthologic Repair Using The Nexa Osteocure Bone GraftWyka FaulaniNo ratings yet
- Intraosseous GanglionDocument10 pagesIntraosseous GanglionNasir MuzaffarNo ratings yet
- FRACTUREDocument5 pagesFRACTUREVirginbum Fatty downNo ratings yet
- Functional Outcomes of Nonunion Scaphoid Fracture Treated by PDFDocument6 pagesFunctional Outcomes of Nonunion Scaphoid Fracture Treated by PDFHazorthoNo ratings yet
- Anehosur Et Al 2020 Concepts and Challenges in The Surgical Management of Edentulous Mandible Fractures A Case SeriesDocument7 pagesAnehosur Et Al 2020 Concepts and Challenges in The Surgical Management of Edentulous Mandible Fractures A Case SeriesHenry Adhy SantosoNo ratings yet
- Dog Bone Lengthening Using Ilizarov MethodDocument3 pagesDog Bone Lengthening Using Ilizarov MethodAlejandra CárdenasNo ratings yet
- Journal of Orthopaedics: B.T. Pushpa, Siddharth N. Aiyer, Muhil Kannan, Anupama Maheswaran, S. RajasekaranDocument2 pagesJournal of Orthopaedics: B.T. Pushpa, Siddharth N. Aiyer, Muhil Kannan, Anupama Maheswaran, S. RajasekaranmohNo ratings yet
- Painful Pseudotendon Caused by Closed Rupture of TDocument6 pagesPainful Pseudotendon Caused by Closed Rupture of TCarlosNo ratings yet
- Journal 2Document3 pagesJournal 2wenny hildaNo ratings yet
- Osteoid Osteoma: A Diagnosis For Radicular Pain of ExtremitiesDocument7 pagesOsteoid Osteoma: A Diagnosis For Radicular Pain of ExtremitiesadeNo ratings yet
- J Orthop Trauma 2007 21 (5) 352Document3 pagesJ Orthop Trauma 2007 21 (5) 352Andrés KnubelNo ratings yet
- Angiographic Evaluation of Arterial Configuration After Acute Shortening 2013Document9 pagesAngiographic Evaluation of Arterial Configuration After Acute Shortening 2013aymanNo ratings yet
- Case Report: A Rare Case of Bilateral Patellar Tendon Ruptures: A Case Report and Literature ReviewDocument4 pagesCase Report: A Rare Case of Bilateral Patellar Tendon Ruptures: A Case Report and Literature ReviewOBLIVION_29No ratings yet
- Osteophyte at SIJ Causing SciaticaDocument4 pagesOsteophyte at SIJ Causing SciaticaHayyu F RachmadhanNo ratings yet
- Catastrophic Talar Bone Loss From High Velocity Trauma Treated With Structural Tricorticate Fibula Autograft Compression Frame and Midfoot Distraction ArthroplastyDocument9 pagesCatastrophic Talar Bone Loss From High Velocity Trauma Treated With Structural Tricorticate Fibula Autograft Compression Frame and Midfoot Distraction ArthroplastyAthenaeum Scientific PublishersNo ratings yet
- Management of Elbow Osteoarthritis: Current Concepts ReviewDocument11 pagesManagement of Elbow Osteoarthritis: Current Concepts ReviewChristopher BermeoNo ratings yet
- Arthroscopic Debridement and Drilling of Osteochondral Lesions of The TalusDocument15 pagesArthroscopic Debridement and Drilling of Osteochondral Lesions of The TalusAnonymous kdBDppigENo ratings yet
- Medscape Knee OCDDocument16 pagesMedscape Knee OCDDita Ambarsari SyafruddinNo ratings yet
- A Case of Congenital Pseudoarthrosis Tibia Treated by Four in One Procedure and Review of LiteratureDocument5 pagesA Case of Congenital Pseudoarthrosis Tibia Treated by Four in One Procedure and Review of LiteratureArya NugrahaNo ratings yet
- Ankle Syndesmosis Injuries Diagnosis and TreatmentDocument11 pagesAnkle Syndesmosis Injuries Diagnosis and TreatmentRoger WatersNo ratings yet
- Femoral Head Osteonecrosis Why Choose FreeDocument6 pagesFemoral Head Osteonecrosis Why Choose FreeFreestanding identificationNo ratings yet
- Osteochondroma Fracture in Young Athlete Bfe9f44bDocument4 pagesOsteochondroma Fracture in Young Athlete Bfe9f44bViona Ananda putriNo ratings yet
- The Journal of Foot & Ankle SurgeryDocument5 pagesThe Journal of Foot & Ankle SurgeryDewidewidewi Madridista Part IINo ratings yet
- SEGMENTAL-CLAVICLE-FRACTU_2011_Revista-Brasileira-de-Ortopedia--English-EditDocument3 pagesSEGMENTAL-CLAVICLE-FRACTU_2011_Revista-Brasileira-de-Ortopedia--English-EditMladenNo ratings yet
- Case series OIDocument6 pagesCase series OIJulius JuliusNo ratings yet
- Radio Logical Assessment of OA FinalDocument60 pagesRadio Logical Assessment of OA FinaltarikeopsNo ratings yet
- Ilizarov 3 PDFDocument3 pagesIlizarov 3 PDFMuthu KumarNo ratings yet
- 1996-Subhepatic Migration of A Hip Prosthesis.Document2 pages1996-Subhepatic Migration of A Hip Prosthesis.Josep M Muñoz VivesNo ratings yet
- Azar 2003 Otsm Repair of Acute Distal Biceps Tendon RuptureDocument4 pagesAzar 2003 Otsm Repair of Acute Distal Biceps Tendon RuptureKuozram No MasNo ratings yet
- Total Hip Arthroplasty With Trochanteric Ostectomy For Patients With Angular Deformity of The Proximal FemurDocument8 pagesTotal Hip Arthroplasty With Trochanteric Ostectomy For Patients With Angular Deformity of The Proximal Femurdrbane123No ratings yet
- Osgood SlaterDocument5 pagesOsgood Slaterpruebaunodos123No ratings yet
- Arthroscopic findings of TMJ traumaDocument4 pagesArthroscopic findings of TMJ traumaThe Reading CrabNo ratings yet
- Nelson EWDocument6 pagesNelson EWDewidewidewi Madridista Part IINo ratings yet
- Cartilage Injury of the Knee: State-of-the-Art Treatment and ControversiesFrom EverandCartilage Injury of the Knee: State-of-the-Art Treatment and ControversiesAaron J. KrychNo ratings yet
- The Reliability and Validity of The Vancouver Classification of Femoral Fractures After Hip ReplacementDocument4 pagesThe Reliability and Validity of The Vancouver Classification of Femoral Fractures After Hip ReplacementDavidBeatonComuladaNo ratings yet
- A Proposed Classification of Supracondylar FemurFractures Above Total Knee ArthroplastiesDocument4 pagesA Proposed Classification of Supracondylar FemurFractures Above Total Knee ArthroplastiesDavidBeatonComuladaNo ratings yet
- Synergy Hip System-SmallerDocument20 pagesSynergy Hip System-SmallerDavidBeatonComuladaNo ratings yet
- UE 1 Clavicle FracturesDocument46 pagesUE 1 Clavicle FracturesDavidBeatonComuladaNo ratings yet
- Periprosthetic Fractures of The Proximal Femur Beyond The Vancouver ClassificationDocument8 pagesPeriprosthetic Fractures of The Proximal Femur Beyond The Vancouver ClassificationDavidBeatonComuladaNo ratings yet
- Matching Nail Angle and Native Neck-Shaft AngleDocument4 pagesMatching Nail Angle and Native Neck-Shaft AngleDavidBeatonComuladaNo ratings yet
- Osteoarthritis Associated With Osteopetrosis.30Document6 pagesOsteoarthritis Associated With Osteopetrosis.30DavidBeatonComuladaNo ratings yet
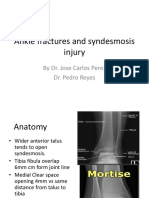
- Ankle fractures and syndesmosis injury treatment optionsDocument11 pagesAnkle fractures and syndesmosis injury treatment optionsDavidBeatonComuladaNo ratings yet
- Does Femoral Notching During Total Knee Arthroplasty Influence Periprosthetic Fracture. A Prospective StudyDocument6 pagesDoes Femoral Notching During Total Knee Arthroplasty Influence Periprosthetic Fracture. A Prospective StudyDavidBeatonComuladaNo ratings yet
- Vahedi2020 PDFDocument4 pagesVahedi2020 PDFDavidBeatonComuladaNo ratings yet
- Total Knee Arthroplasty in Osteopetrosis Using Patient-Specific InstrumentationDocument4 pagesTotal Knee Arthroplasty in Osteopetrosis Using Patient-Specific InstrumentationDavidBeatonComuladaNo ratings yet
- Vahedi2020 PDFDocument4 pagesVahedi2020 PDFDavidBeatonComuladaNo ratings yet
- Rheumatoid Hand and Wrist Surgery Soft Tissue.99323Document9 pagesRheumatoid Hand and Wrist Surgery Soft Tissue.99323DavidBeatonComuladaNo ratings yet
- Osteoarthritis and Osteopetrosis Treated by Knee ReplacementDocument6 pagesOsteoarthritis and Osteopetrosis Treated by Knee ReplacementDavidBeatonComuladaNo ratings yet
- Intramedullary Nailing of Periarticular Fractures.2Document11 pagesIntramedullary Nailing of Periarticular Fractures.2DavidBeatonComuladaNo ratings yet
- Tendon Transfers For Radial, Median, and Ulnar Nerve Palsy: Review ArticleDocument10 pagesTendon Transfers For Radial, Median, and Ulnar Nerve Palsy: Review ArticleDavidBeatonComuladaNo ratings yet
- Intramedullary Nailing of Femoral Shaft Fractures .4Document10 pagesIntramedullary Nailing of Femoral Shaft Fractures .4DavidBeatonComuladaNo ratings yet
- Hamilton 2014Document1 pageHamilton 2014DavidBeatonComuladaNo ratings yet
- Prosthetic Joint InfectionDocument21 pagesProsthetic Joint InfectionDavidBeatonComuladaNo ratings yet
- Primary TKA TechniqueDocument23 pagesPrimary TKA TechniqueDavidBeatonComuladaNo ratings yet
- Osteoarthritis Associated With Osteopetrosis.30Document6 pagesOsteoarthritis Associated With Osteopetrosis.30DavidBeatonComuladaNo ratings yet
- Limb Length DiscrepancyDocument75 pagesLimb Length DiscrepancyDavidBeatonComuladaNo ratings yet
- Pembimbing: Dr. Hildebrand Hannoch Victor Watupongoh, SP - PD Disusun Oleh: Advenny Elisabeth 1161050151Document24 pagesPembimbing: Dr. Hildebrand Hannoch Victor Watupongoh, SP - PD Disusun Oleh: Advenny Elisabeth 1161050151Advenny ElisabethNo ratings yet
- (Osborn) Chapter 60: Learning Outcome 1 Learning Outcome 2 Learning Outcome 3Document14 pages(Osborn) Chapter 60: Learning Outcome 1 Learning Outcome 2 Learning Outcome 3KittiesNo ratings yet
- Health Declaration Form D02Document1 pageHealth Declaration Form D02Hizwani ZainalNo ratings yet
- Histiocytic SarcomaDocument8 pagesHistiocytic SarcomadanishNo ratings yet
- Compare Bisoprolol Vs AtenololDocument4 pagesCompare Bisoprolol Vs AtenololMohammed shamiul ShahidNo ratings yet
- Interview With Paul Cheney ImmunocolDocument7 pagesInterview With Paul Cheney Immunocolapi-3714923No ratings yet
- Disaster Associated Health IssuesDocument29 pagesDisaster Associated Health Issuesmeshack mbalaNo ratings yet
- CUTANEOUS ALLERGY MECHANISMS AND TESTINGDocument26 pagesCUTANEOUS ALLERGY MECHANISMS AND TESTINGThiti JessadaromNo ratings yet
- Aun Herbal CatalogDocument29 pagesAun Herbal Catalogaunherbalremedies2009No ratings yet
- Labor and ComplicationsDocument51 pagesLabor and ComplicationsTrisha Mae MarquezNo ratings yet
- 5-Troubles de La Motricité - Les ParalysiesDocument6 pages5-Troubles de La Motricité - Les Paralysiesanon_391445722100% (2)
- Liu036 Brain Disorders PDFDocument2 pagesLiu036 Brain Disorders PDFAyeshaNo ratings yet
- Calawag National High School MAPEH AssessmentDocument2 pagesCalawag National High School MAPEH AssessmentMarbert GarganzaNo ratings yet
- Case StudyDocument4 pagesCase StudyMargarita Limon BalunesNo ratings yet
- Focal InfectionDocument2 pagesFocal InfectionRoza NafilahNo ratings yet
- BakteriDocument8 pagesBakteriAgus SugiartoNo ratings yet
- Pill CameraDocument21 pagesPill CameraAnil DsouzaNo ratings yet
- Test Report: Patient ID 0100007634 Sid NoDocument2 pagesTest Report: Patient ID 0100007634 Sid NoBalamurugan ArumugamNo ratings yet
- After TURP: What to expectDocument2 pagesAfter TURP: What to expectvilla88No ratings yet
- Assesment Post Op Ratna GCT Radius - Preop Sekar MegaprothesisDocument32 pagesAssesment Post Op Ratna GCT Radius - Preop Sekar MegaprothesisReza Devianto HambaliNo ratings yet
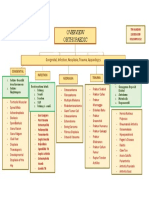
- Orthopaedic: Congenital, Infection, Neoplasia, Trauma, AppandegesDocument1 pageOrthopaedic: Congenital, Infection, Neoplasia, Trauma, AppandegesdinsNo ratings yet
- Approach to the lymph node: A concise guide to evaluation and diagnosisDocument75 pagesApproach to the lymph node: A concise guide to evaluation and diagnosisJose SirittNo ratings yet
- Causes and Treatment of SplenomegalyDocument4 pagesCauses and Treatment of SplenomegalydoctorimrankabirNo ratings yet
- OptoPrep Part1 StudyCalendar 3-MonthDocument4 pagesOptoPrep Part1 StudyCalendar 3-MonthmelanieNo ratings yet