You might also like
- Metastatic Spine Disease: A Guide to Diagnosis and ManagementFrom EverandMetastatic Spine Disease: A Guide to Diagnosis and ManagementRex A. W. MarcoNo ratings yet
- Adult Traumatic Brachial PlexusDocument12 pagesAdult Traumatic Brachial PlexusMarjeane Cristina Jaques Hockmuller mhockmullerNo ratings yet
- Blood Loss Management in Spine Surgery.1Document10 pagesBlood Loss Management in Spine Surgery.1ngurahNo ratings yet
- Treatment of Common Congenital Hand Conditions.43Document13 pagesTreatment of Common Congenital Hand Conditions.43Ioana BarcariNo ratings yet
- Post2019 CS-1011Document1 pagePost2019 CS-1011Jaume SanahujaNo ratings yet
- Unraveling The Mechanisms of Manual Therapy: Modeling An ApproachDocument11 pagesUnraveling The Mechanisms of Manual Therapy: Modeling An ApproachMatheus BorgesNo ratings yet
- JAAOS Preoperative - Peripheral - Nerve - Blocks - in Trauma. (22088)Document7 pagesJAAOS Preoperative - Peripheral - Nerve - Blocks - in Trauma. (22088)Ben QuigleyNo ratings yet
- Role of Ligamentotaxis in Management of Comminuted Intra/ Juxta Articular FracturesDocument3 pagesRole of Ligamentotaxis in Management of Comminuted Intra/ Juxta Articular FracturesNidhish PatelNo ratings yet
- J Am Acad Orthop Surg 2018 OctoberDocument67 pagesJ Am Acad Orthop Surg 2018 Octoberyarimar hoyosNo ratings yet
- Principles of Metacarpal and Phalangeal Fracture Management: A Review of Rehabilitation ConceptsDocument19 pagesPrinciples of Metacarpal and Phalangeal Fracture Management: A Review of Rehabilitation ConceptsInas MellanisaNo ratings yet
- Anesthesia in Cosmetic Surgery.40Document2 pagesAnesthesia in Cosmetic Surgery.40Delladuasatu stellaNo ratings yet
- Extensor Tendon Injuries in The Hand JAAOSDocument8 pagesExtensor Tendon Injuries in The Hand JAAOSAzmi FarhadiNo ratings yet
- Adult Isthmic SpondylolisthesisDocument9 pagesAdult Isthmic SpondylolisthesisAlex CortesNo ratings yet
- Current Concepts in The Management of Dupuytren.3Document8 pagesCurrent Concepts in The Management of Dupuytren.3Shu Yang HuNo ratings yet
- Nonoperative Treatment of UCLDocument8 pagesNonoperative Treatment of UCLMarisé Llanos RoblesNo ratings yet
- How To Communicate Between Surgeon And.8Document7 pagesHow To Communicate Between Surgeon And.8FIA SlotNo ratings yet
- Nonsurgical Rhinoplasty: A Systematic Review of Technique, Outcomes, and ComplicationsDocument11 pagesNonsurgical Rhinoplasty: A Systematic Review of Technique, Outcomes, and ComplicationsSam CruzNo ratings yet
- Unraveling The Mechanisms of Manual Therapy: Modeling An ApproachDocument12 pagesUnraveling The Mechanisms of Manual Therapy: Modeling An ApproachCollin AndrusNo ratings yet
- Evaluation of The Painful Total Knee Arthroplasty.99377Document9 pagesEvaluation of The Painful Total Knee Arthroplasty.99377Filip starcevic100% (1)
- Basics and Best Practices of Multimodal Pain.34Document7 pagesBasics and Best Practices of Multimodal Pain.34QuangTiến ĐỗNo ratings yet
- Síndrome de Charcot-Marie-ToothDocument7 pagesSíndrome de Charcot-Marie-ToothXDbr xdNo ratings yet
- Case Report Stensrud2012Document13 pagesCase Report Stensrud2012marcus souzaNo ratings yet
- Safe Surgery Globally by 2030 The View From.3Document4 pagesSafe Surgery Globally by 2030 The View From.3erick jarandillaNo ratings yet
- Surgical Management of Patellofemoral Instability in The Skeletally Immature PatientDocument11 pagesSurgical Management of Patellofemoral Instability in The Skeletally Immature Patienttyoinfantil.hegcNo ratings yet
- 2019 - Humeral Shaft BraceDocument8 pages2019 - Humeral Shaft BraceSergio Navarrete VidalNo ratings yet
- ALLEGATO 03 Optimizing Recovery After Knee Meniscal or Cartilage InjuryDocument1 pageALLEGATO 03 Optimizing Recovery After Knee Meniscal or Cartilage Injuryale.zatti7No ratings yet
- Lesiones SindesmalesDocument9 pagesLesiones SindesmalesDaniel Cancino CallirgosNo ratings yet
- Flexor Tendon Repair, Rehabilitation, and Reconstruction: Preoperative AssessmentDocument11 pagesFlexor Tendon Repair, Rehabilitation, and Reconstruction: Preoperative AssessmentAdRiaNa JuLIetH LoZaDa PaTiÑoNo ratings yet
- Meals 2013Document11 pagesMeals 2013Harry CenNo ratings yet
- Ref 5Document8 pagesRef 5DahoviNo ratings yet
- Chiros ScientifDocument3 pagesChiros ScientifS Bascur V.No ratings yet
- Residual Limb Complications and Management StrategiesDocument9 pagesResidual Limb Complications and Management StrategiesTarushi TanwarNo ratings yet
- SJX 218Document11 pagesSJX 218Equipo AsoinmedNo ratings yet
- Orthopaedic Surgical Selection and Inpatient Paradigms During The Coronavirus (COVID-19) PandemicDocument15 pagesOrthopaedic Surgical Selection and Inpatient Paradigms During The Coronavirus (COVID-19) PandemicsitifathiyaNo ratings yet
- Functional Outcomes of Traumatic and Non-Traumatic Rotator Cuff Tears After Arthroscopic RepairDocument8 pagesFunctional Outcomes of Traumatic and Non-Traumatic Rotator Cuff Tears After Arthroscopic RepairAnonymous 7hLtYS1dkNo ratings yet
- Complicationsoffracturehealing AReviewDocument9 pagesComplicationsoffracturehealing AReviewMuhamad vero SyatiaNo ratings yet
- 10 1097@jsa 0000000000000275Document6 pages10 1097@jsa 0000000000000275Subarna PaudelNo ratings yet
- Polydactyly of The Foot A Review.92Document10 pagesPolydactyly of The Foot A Review.92mamyeu1801No ratings yet
- BMJ j1982 FullDocument8 pagesBMJ j1982 FullSamantha ColleNo ratings yet
- Module 2 PDFDocument23 pagesModule 2 PDFRui ViegasNo ratings yet
- Bracing After ACL Reconstruction: A Systematic ReviewDocument7 pagesBracing After ACL Reconstruction: A Systematic ReviewDanar AdhimuktiNo ratings yet
- Bialosky Et Al 2017 Unraveling The Mechanisms of Manual Therapy Modeling An ApproachDocument11 pagesBialosky Et Al 2017 Unraveling The Mechanisms of Manual Therapy Modeling An ApproachAlan KipperNo ratings yet
- Arm ContouringDocument11 pagesArm ContouringfumblefumbleNo ratings yet
- An Analysis of The Cost-Effectiveness of Spinal Versus General Anesthesia For Lumbar Spine Surgery in Various Hospital SettingsDocument7 pagesAn Analysis of The Cost-Effectiveness of Spinal Versus General Anesthesia For Lumbar Spine Surgery in Various Hospital SettingsGaetano De BiaseNo ratings yet
- Treatment Strategyfor Irreparable Rotator Cuff TearsDocument16 pagesTreatment Strategyfor Irreparable Rotator Cuff TearshawkjohnNo ratings yet
- Unraveling The Mechanisms of Manual Therapy Modeling An ApproachDocument11 pagesUnraveling The Mechanisms of Manual Therapy Modeling An Approachvicente leivaNo ratings yet
- ArthrocentesisDocument10 pagesArthrocentesisPranave PNo ratings yet
- Concepts in Foot Drop Management - Review of The CuDocument10 pagesConcepts in Foot Drop Management - Review of The CuIntanicNo ratings yet
- RTC Strengthening ArticleDocument14 pagesRTC Strengthening ArticleineedsheetzNo ratings yet
- RTC Strengthening Article PDFDocument14 pagesRTC Strengthening Article PDFineedsheetzNo ratings yet
- Five Operations That Give The Best Results After Brachial Plexus InjuryDocument12 pagesFive Operations That Give The Best Results After Brachial Plexus InjuryResurg ClinicNo ratings yet
- Exoskeleton Design For Upper Limb Rehabilitation of Post-Trauma PatientsDocument4 pagesExoskeleton Design For Upper Limb Rehabilitation of Post-Trauma PatientserpublicationNo ratings yet
- Snyder Mackler2012Document9 pagesSnyder Mackler2012josefinaNo ratings yet
- Multilevel ReplantationDocument11 pagesMultilevel ReplantationShaneNo ratings yet
- Management of Segmental Bone DefectDocument11 pagesManagement of Segmental Bone DefectZin HtutNo ratings yet
- Leg-Length Discrepancy, Functional Scoliosis, and Low Back PainDocument8 pagesLeg-Length Discrepancy, Functional Scoliosis, and Low Back PainRez QNo ratings yet
- 10 1016@j JHT 2020 03 024Document10 pages10 1016@j JHT 2020 03 024eduar yecid duarte gomezNo ratings yet
- Pathomechanics and Management of Secondary ComplicDocument10 pagesPathomechanics and Management of Secondary ComplicnabeelNo ratings yet
- NB - Systematic Approach To The Management of Post-Traumatic Segmental Diaphyseal Long Bone Defect - NandoDocument12 pagesNB - Systematic Approach To The Management of Post-Traumatic Segmental Diaphyseal Long Bone Defect - NandoSerenna DehalooNo ratings yet
- A Systematic Review of Electromyography Studies in Normal Shoulders To Inform Postoperative Rehabilitation Following Rotator Cuff RepairDocument14 pagesA Systematic Review of Electromyography Studies in Normal Shoulders To Inform Postoperative Rehabilitation Following Rotator Cuff Repairshsh ShshsshNo ratings yet
- UE 1 Clavicle FracturesDocument46 pagesUE 1 Clavicle FracturesDavidBeatonComuladaNo ratings yet
- Does Femoral Notching During Total Knee Arthroplasty Influence Periprosthetic Fracture. A Prospective StudyDocument6 pagesDoes Femoral Notching During Total Knee Arthroplasty Influence Periprosthetic Fracture. A Prospective StudyDavidBeatonComuladaNo ratings yet
- Synergy Hip System-SmallerDocument20 pagesSynergy Hip System-SmallerDavidBeatonComuladaNo ratings yet
- Matching Nail Angle and Native Neck-Shaft AngleDocument4 pagesMatching Nail Angle and Native Neck-Shaft AngleDavidBeatonComuladaNo ratings yet
- Periprosthetic Fractures of The Proximal Femur Beyond The Vancouver ClassificationDocument8 pagesPeriprosthetic Fractures of The Proximal Femur Beyond The Vancouver ClassificationDavidBeatonComuladaNo ratings yet
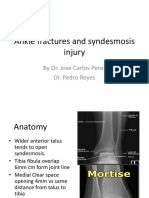
- Ankle Fractures and Syndesmosis Injury: by Dr. Jose Carlos Perez Dr. Pedro ReyesDocument11 pagesAnkle Fractures and Syndesmosis Injury: by Dr. Jose Carlos Perez Dr. Pedro ReyesDavidBeatonComuladaNo ratings yet
- Vahedi2020 PDFDocument4 pagesVahedi2020 PDFDavidBeatonComuladaNo ratings yet
- Osteoarthritis Associated With Osteopetrosis.30Document6 pagesOsteoarthritis Associated With Osteopetrosis.30DavidBeatonComuladaNo ratings yet
- Total Joint Arthroplasty in Patients With Osteopetrosis: A Report of 5 Cases and Review of The LiteratureDocument6 pagesTotal Joint Arthroplasty in Patients With Osteopetrosis: A Report of 5 Cases and Review of The LiteratureDavidBeatonComuladaNo ratings yet
- Total Knee Arthroplasty in Osteopetrosis Using Patient-Specific InstrumentationDocument4 pagesTotal Knee Arthroplasty in Osteopetrosis Using Patient-Specific InstrumentationDavidBeatonComuladaNo ratings yet
- Hamilton 2014Document1 pageHamilton 2014DavidBeatonComuladaNo ratings yet
- Intramedullary Nailing of Femoral Shaft Fractures .4Document10 pagesIntramedullary Nailing of Femoral Shaft Fractures .4DavidBeatonComuladaNo ratings yet
- Osteoarthritis Associated With Osteopetrosis.30Document6 pagesOsteoarthritis Associated With Osteopetrosis.30DavidBeatonComuladaNo ratings yet
- Vanhove2014 PDFDocument5 pagesVanhove2014 PDFDavidBeatonComuladaNo ratings yet
- Temporal Bone AnatomyDocument27 pagesTemporal Bone AnatomyChangho Lee100% (5)
- Manual Therapy: Jeremy LewisDocument12 pagesManual Therapy: Jeremy LewisMariano OsorioNo ratings yet
- Which Parameters Are Relevant in Sagittal Balance Analysis of The Cervical Spine? A Literature ReviewDocument8 pagesWhich Parameters Are Relevant in Sagittal Balance Analysis of The Cervical Spine? A Literature ReviewMohsen AzarNo ratings yet
- Types of ExcerciseDocument13 pagesTypes of ExcerciseTefera LeteboNo ratings yet
- Biology ProjectDocument8 pagesBiology ProjectSANJAYNo ratings yet
- Week 4 Yoga and PilatesDocument36 pagesWeek 4 Yoga and PilatesSkarlon BalagtasNo ratings yet
- Pelzer Et Al., 2017 - Periodization Effects During Short-Term Resistance Training With Equated Exercise Variables in FemalesDocument14 pagesPelzer Et Al., 2017 - Periodization Effects During Short-Term Resistance Training With Equated Exercise Variables in FemalesRicardo Pereira NevesNo ratings yet
- The Fabulous 15 Exercises For A Better Vertical PDFDocument5 pagesThe Fabulous 15 Exercises For A Better Vertical PDFKeijoNo ratings yet
- 3431-Article Text-12963-2-10-20220828Document13 pages3431-Article Text-12963-2-10-20220828Marsyah CharuzzikriaNo ratings yet
- Promedics Therapy Catalogue 2015Document148 pagesPromedics Therapy Catalogue 2015Nicole Maldonado MenesesNo ratings yet
- Reconstruction of MaxillaDocument58 pagesReconstruction of MaxillaAnjum IqbalNo ratings yet
- The Role of Proprioception and Neuromuscular Stability in Carpal InstabilitiesDocument8 pagesThe Role of Proprioception and Neuromuscular Stability in Carpal Instabilities杨钦杰No ratings yet
- The Complete Guide To Yoga PDFDocument356 pagesThe Complete Guide To Yoga PDFagustinNo ratings yet
- PhysioEx Exercise 2 Activity 6Document8 pagesPhysioEx Exercise 2 Activity 6scasandra192No ratings yet
- 1998 Knee Injury and Osteoarthritis Outcome Score (KOOS) - Development of A Self-Administered Outcome MeasureDocument9 pages1998 Knee Injury and Osteoarthritis Outcome Score (KOOS) - Development of A Self-Administered Outcome MeasureCastro WeithNo ratings yet
- Anatomy Lab Syllabus Fall 2015 WebCTDocument18 pagesAnatomy Lab Syllabus Fall 2015 WebCTkarijaniNo ratings yet
- Osteology BonesDocument48 pagesOsteology BonesÂhmęd ĐoolaNo ratings yet
- Presented by - Rutuja Suryawanshi Roll No.:-34 Batch: - Summer 2020-21 Date of Presentation: - 1/5/2021Document41 pagesPresented by - Rutuja Suryawanshi Roll No.:-34 Batch: - Summer 2020-21 Date of Presentation: - 1/5/2021Anurag SuryawanshiNo ratings yet
- Lower Extremity DisordersDocument14 pagesLower Extremity DisordersJameson87No ratings yet
- Surgery of The Hip Joint 1984Document435 pagesSurgery of The Hip Joint 1984Igor IvanesNo ratings yet
- Imaging of Diffuse Idiopathic Skeletal Hyperostosis (DISH) : Original ResearchDocument8 pagesImaging of Diffuse Idiopathic Skeletal Hyperostosis (DISH) : Original ResearchLorenc OrtopediNo ratings yet
- MFM42Support - Answers of End Module MSK1Document8 pagesMFM42Support - Answers of End Module MSK1Mohammed HashemNo ratings yet
- Final ArthridesDocument22 pagesFinal ArthrideskizpirinNo ratings yet
- DR Tans Balance Method PDFDocument18 pagesDR Tans Balance Method PDFJoy Arguelles GoolNo ratings yet
- Laporan Physioex Modul MusketDocument65 pagesLaporan Physioex Modul MusketAfifah Marwah Al-Qadrie100% (1)
- Muscular System DisordersDocument36 pagesMuscular System DisordersShawn Henry CepedaNo ratings yet
- Proximal Femur FracturesDocument191 pagesProximal Femur FracturesGreenIron9No ratings yet
- Topic: Mechanics of PositionDocument17 pagesTopic: Mechanics of Positionbakhtawar safdarNo ratings yet
- Beef CutsDocument50 pagesBeef Cutsoptimeatvaleria100% (3)
- Surgery For LBP - DR ManaekDocument44 pagesSurgery For LBP - DR ManaekArsyad MustaminNo ratings yet