You might also like
- (CC) Malpresentation and DeliveryDocument6 pages(CC) Malpresentation and DeliveryDaryl Gay NanoNo ratings yet
- Operative Print3 Medad-NotesDocument46 pagesOperative Print3 Medad-NotesOliverYousryNo ratings yet
- Breech PDFDocument4 pagesBreech PDFMiguel Cuevas Dolot100% (1)
- Wa0010.Document18 pagesWa0010.deekshaNo ratings yet
- Cephalocaudal KemerutDocument10 pagesCephalocaudal KemerutKIANA LOUISE ROMANONo ratings yet
- OB Chap 22 - Normal LaborDocument4 pagesOB Chap 22 - Normal LaborChino Paolo SamsonNo ratings yet
- BREECH 2nijnjinijnuihiuhDocument7 pagesBREECH 2nijnjinijnuihiuhChethranNo ratings yet
- 19 - Vaginal DeliveryDocument16 pages19 - Vaginal DeliveryGen XNo ratings yet
- Patho OB - Breech DeliveryDocument7 pagesPatho OB - Breech DeliverySheryl Layne Lao-SebrioNo ratings yet
- NCM 107 Rle 2Document2 pagesNCM 107 Rle 2Patricia RamosNo ratings yet
- Essentials of Plastic SurgeryDocument12 pagesEssentials of Plastic SurgeryjoryadelmNo ratings yet
- Topic Outline: Rafael Babiano, PTRP/PT2115/November 03, 2021Document14 pagesTopic Outline: Rafael Babiano, PTRP/PT2115/November 03, 2021Charlize MarthaNo ratings yet
- Inguinal Region 1617Document23 pagesInguinal Region 1617Gx NavinNo ratings yet
- Final Ob1Document14 pagesFinal Ob1crix crixNo ratings yet
- Osce Py CompilationDocument47 pagesOsce Py CompilationBrandonRyanF.MosidinNo ratings yet
- Bilateral Direct HerniaDocument7 pagesBilateral Direct HerniaTeja Laksana NukanaNo ratings yet
- ENT 1.3 Lips and Oral CavityDocument15 pagesENT 1.3 Lips and Oral CavityZazaNo ratings yet
- Medical Appendix IDocument3 pagesMedical Appendix ITexchikaNo ratings yet
- Nursing Care Plan2 CVADocument4 pagesNursing Care Plan2 CVAhermesdave1No ratings yet
- 3 - Female PelvisDocument27 pages3 - Female PelvisKandula KasunNo ratings yet
- Problems of The PassengerDocument9 pagesProblems of The PassengerDanah Grace SanchezNo ratings yet
- ? DX Lie N Presentation: Abdominal Palpation VE Auscultation Fetal Heart Sonography /radiographyDocument2 pages? DX Lie N Presentation: Abdominal Palpation VE Auscultation Fetal Heart Sonography /radiographynmyza89No ratings yet
- Functional and Clinical Anatomy of Lower Limb LectureDocument7 pagesFunctional and Clinical Anatomy of Lower Limb Lectureteam.tell.0qNo ratings yet
- Breech DeliveryDocument5 pagesBreech DeliveryChristine Evan HoNo ratings yet
- Gravida - The Number of Pregnancies That o Progesterone Deprivation TheoryDocument27 pagesGravida - The Number of Pregnancies That o Progesterone Deprivation TheoryRoshin Tejero100% (1)
- M10-MED - Cleft Lip, Alveolus and Palate (CLAP) - Team02Document5 pagesM10-MED - Cleft Lip, Alveolus and Palate (CLAP) - Team02abeer alrofaeyNo ratings yet
- 15 Physio OB - Normal LaborDocument8 pages15 Physio OB - Normal LabormaqmmNo ratings yet
- Hernia - Surgery PrecisDocument1 pageHernia - Surgery PrecisSherif WagdyNo ratings yet
- Tipe Gait Cerebral PalsyDocument23 pagesTipe Gait Cerebral PalsyrenihardiyantiNo ratings yet
- Fetal Malposition UpdatedDocument3 pagesFetal Malposition UpdatedJozarine Chelsea LopezNo ratings yet
- Ao UcsDocument6 pagesAo Ucsdennis ferreraNo ratings yet
- Anatomy of PelvisDocument15 pagesAnatomy of PelvisJonnah Mae Belmonte100% (1)
- OB1 3.2 Normal Labor and Delivery IIDocument10 pagesOB1 3.2 Normal Labor and Delivery IIManjula100% (1)
- 1.01 Esophagus and Diaphragmatic HerniaDocument10 pages1.01 Esophagus and Diaphragmatic HerniaZazaNo ratings yet
- Kaushik Banerjee OrthopaedicsDocument281 pagesKaushik Banerjee OrthopaedicsSwarnadeep Mani50% (4)
- Five Animals Qi Gong (五禽戲 Wu Qin Xi) : TigerDocument3 pagesFive Animals Qi Gong (五禽戲 Wu Qin Xi) : Tigereeklşeke kelekşlekNo ratings yet
- Hernia UmbilikalisDocument16 pagesHernia UmbilikalisWibhuti EmrikoNo ratings yet
- Speaker: Dr. Shafat A Mir Department of Anaesthesia and Critical Care SKIMS, Srinagar, J&k.indiaDocument74 pagesSpeaker: Dr. Shafat A Mir Department of Anaesthesia and Critical Care SKIMS, Srinagar, J&k.indiatutorial desatuNo ratings yet
- Gastrointestinal Examination - DR - Hammouri's Style: Rahaf Wardeh Internal Medicine 2016-2017Document5 pagesGastrointestinal Examination - DR - Hammouri's Style: Rahaf Wardeh Internal Medicine 2016-2017asdddNo ratings yet
- OSCE1Document5 pagesOSCE1Ahmed Mohammed omarNo ratings yet
- Fetal SkullDocument34 pagesFetal SkullNeelofur Ibran Ali85% (20)
- 10.3) Lower Extremity - Ankle & FootDocument9 pages10.3) Lower Extremity - Ankle & FootDION ANN SAYSONNo ratings yet
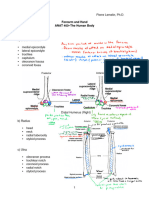
- Forearm and HandDocument8 pagesForearm and Handteam.tell.0qNo ratings yet
- 8.2 Inguinal Hernias, PUV, and VUR - March 14 - Dr. Gellido & Dr. LawenkoDocument8 pages8.2 Inguinal Hernias, PUV, and VUR - March 14 - Dr. Gellido & Dr. LawenkoJess PeltraNo ratings yet
- Anatomy Quiz 2 Review - Luke GriffinDocument6 pagesAnatomy Quiz 2 Review - Luke Griffinnategozdor58No ratings yet
- Cleft Lip, Cleft Palate, and Velopharyngeal.36Document19 pagesCleft Lip, Cleft Palate, and Velopharyngeal.36Jimmy Mejía Cirujano PlásticoNo ratings yet
- Esophageal Atresia and Tracheoesophageal Fistula MalformationsDocument23 pagesEsophageal Atresia and Tracheoesophageal Fistula MalformationsAnonymous Hx5eGBNNo ratings yet
- Elements of Globally Competent TeacherDocument3 pagesElements of Globally Competent Teacherjao jeonNo ratings yet
- Chinchilla SkullDocument12 pagesChinchilla Skullf.baobao28No ratings yet
- 2-3 BRAIN 4th YearDocument71 pages2-3 BRAIN 4th YearYosra —No ratings yet
- Marrow ErrataDocument268 pagesMarrow ErrataDr.Ebenesar DhasarathanNo ratings yet
- Pharynx: Upper Part: Widest - 3.5 CM, Non-Collapsible Middle Part: Narrow Lower End: Narrowest Part of GITDocument5 pagesPharynx: Upper Part: Widest - 3.5 CM, Non-Collapsible Middle Part: Narrow Lower End: Narrowest Part of GITdrpnnreddyNo ratings yet
- Club Foot CtevDocument82 pagesClub Foot Ctevtuyulgaul100% (1)
- Backup of LO 2 DD HERNIA - Id.en-2Document3 pagesBackup of LO 2 DD HERNIA - Id.en-2dianNo ratings yet
- Orthopedic FinalDocument858 pagesOrthopedic Finalhashmf180% (10)
- Cell Damage and DeathDocument1 pageCell Damage and DeathfgdhgfrhNo ratings yet
- Glasgow Coma ScaleDocument4 pagesGlasgow Coma ScalefgdhgfrhNo ratings yet
- MedicalBooks PDFDocument80 pagesMedicalBooks PDFfgdhgfrh50% (8)
- Embryology 10Document5 pagesEmbryology 10fgdhgfrhNo ratings yet
- Hysterectomy: Max Brinsmead MB Bs PHD June 2015Document19 pagesHysterectomy: Max Brinsmead MB Bs PHD June 2015DrChauhan0% (1)
- د يزن ابو غربية نسائيةDocument55 pagesد يزن ابو غربية نسائيةobadaNo ratings yet
- Sistem Pengurusan Kualiti: Jadual Pengajaran TerperinciDocument3 pagesSistem Pengurusan Kualiti: Jadual Pengajaran TerperinciNurul IrhamnaNo ratings yet
- 4 1 36 151Document4 pages4 1 36 151Shelly GargNo ratings yet
- ObsDocument5 pagesObsAemiro TsegayeNo ratings yet
- Expectant Mother'S and Baby Information Sheet: Given Name: Middle Name: Last NameDocument3 pagesExpectant Mother'S and Baby Information Sheet: Given Name: Middle Name: Last NameLeslie D. Aton60% (5)
- Abruptio PlacentaDocument13 pagesAbruptio Placentamiss RN92% (12)
- Acog Committee Opinion: Cesarean Delivery On Maternal RequestDocument5 pagesAcog Committee Opinion: Cesarean Delivery On Maternal RequestfbihansipNo ratings yet
- Maternal Health ProgramDocument5 pagesMaternal Health ProgramMark Kevin Velasco PanchoNo ratings yet
- Placenta PreviaDocument4 pagesPlacenta PreviaJeizel IgnacioNo ratings yet
- Assisting in Insertion of Intrauterine Contraceptive Device (Copper-T)Document4 pagesAssisting in Insertion of Intrauterine Contraceptive Device (Copper-T)manju100% (1)
- In Vitro FertilizationDocument44 pagesIn Vitro FertilizationGing-ging Acdal100% (1)
- PQCNC AIM RPC Spinning BabiesDocument71 pagesPQCNC AIM RPC Spinning Babieskcochran50% (2)
- Dilation and Curettage Janelle ReforDocument4 pagesDilation and Curettage Janelle ReforCjay HernandezNo ratings yet
- NCM 109 (Prelims) - Lesson 1Document5 pagesNCM 109 (Prelims) - Lesson 1nianNo ratings yet
- Fdocuments - in Mother Child Protection Card Telugu Hetvorg Mother Child Protection CardDocument16 pagesFdocuments - in Mother Child Protection Card Telugu Hetvorg Mother Child Protection CardRAJENDRA PRASADNo ratings yet
- Preskas Mioma Geburt DafpusDocument2 pagesPreskas Mioma Geburt DafpusNadira DanataNo ratings yet
- Pregnancy TestDocument2 pagesPregnancy TestGianna SablanNo ratings yet
- (Mar) Bedsite Teaching Gin Maret 2022Document5 pages(Mar) Bedsite Teaching Gin Maret 2022Yudistira YunusNo ratings yet
- 20hr Maternity Staff Course-Ses 3Document36 pages20hr Maternity Staff Course-Ses 3Norhanie Dida-agun AlimodenNo ratings yet
- Orca Share Media1496246332671Document5 pagesOrca Share Media1496246332671HCX dghhqNo ratings yet
- Midwifery in BelgiumDocument2 pagesMidwifery in Belgiummbok diyirNo ratings yet
- Mrs. A, 35 Years Old, MR 01 13 45 74, Severity Level IIIDocument18 pagesMrs. A, 35 Years Old, MR 01 13 45 74, Severity Level IIIprimaindra27No ratings yet
- Journal 1Document4 pagesJournal 1Kristoff CamposNo ratings yet
- Soal Usulan UnHas Juli 2019Document25 pagesSoal Usulan UnHas Juli 2019Ibnu SinaNo ratings yet
- Submitted To: Submitted By:: Paladi FeedingDocument3 pagesSubmitted To: Submitted By:: Paladi FeedingManisa ParidaNo ratings yet
- Level 2 Skills Lab PresentationDocument24 pagesLevel 2 Skills Lab PresentationJamie HaravataNo ratings yet
- Taking History in MedicineDocument20 pagesTaking History in Medicineprincemasr6No ratings yet
- Chapter 19 - Nutritional Needs of A NewbornDocument8 pagesChapter 19 - Nutritional Needs of A NewbornMerenisa LiminNo ratings yet
- Chapter 5 - Displacement of UterusDocument25 pagesChapter 5 - Displacement of Uterusاسامة محمد السيد رمضانNo ratings yet