You might also like
- current approaches in orthognathic surgeryDocument15 pagescurrent approaches in orthognathic surgerysrinivasanNo ratings yet
- We Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsDocument17 pagesWe Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistssafwanNo ratings yet
- Septoplasty Endoscopic and Open TechniquesDocument8 pagesSeptoplasty Endoscopic and Open TechniquesКонстантин БелоусNo ratings yet
- Surgical Approaches For Total Knee ArthroplastyDocument26 pagesSurgical Approaches For Total Knee ArthroplastyramilteimurovumsaNo ratings yet
- Building Up The Future of Colonscopy - A Synergy Between Clinicians and Computer ScientistsDocument35 pagesBuilding Up The Future of Colonscopy - A Synergy Between Clinicians and Computer ScientistsVân NguyễnNo ratings yet
- Arthroscopic Elbow Debridement Using Anterocentral Transbrachialis PortalDocument6 pagesArthroscopic Elbow Debridement Using Anterocentral Transbrachialis PortalMoustafa MohamedNo ratings yet
- Planning and Sizing With OsiriXHorosDocument23 pagesPlanning and Sizing With OsiriXHorosJanineNo ratings yet
- We Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsDocument19 pagesWe Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsFlaviu Ionuț FaurNo ratings yet
- Arthroscopy: A Guide to Knee ProceduresDocument9 pagesArthroscopy: A Guide to Knee ProceduresNyoman Gede BimantaraNo ratings yet
- 10 5772:intechopen 70363Document22 pages10 5772:intechopen 70363motohumeresNo ratings yet
- Serdev Sutures® in Upper Face Brow and Temporal Lift Glabella Muscle LigationDocument41 pagesSerdev Sutures® in Upper Face Brow and Temporal Lift Glabella Muscle LigationRamon Malheiros Barros100% (1)
- Achilles TendonDocument154 pagesAchilles Tendonalinutza_childNo ratings yet
- Endoscopic Procedures on the SpineFrom EverandEndoscopic Procedures on the SpineJin-Sung KimNo ratings yet
- Prosthetics_for_Lower_Limb_AmputationDocument22 pagesProsthetics_for_Lower_Limb_Amputationasmita chauhanNo ratings yet
- Applications of Upper Limb Biomechanical Models in Spinal Cord Injury PatientsDocument41 pagesApplications of Upper Limb Biomechanical Models in Spinal Cord Injury PatientsMarta Leal EscribanoNo ratings yet
- We Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsDocument16 pagesWe Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsrererNo ratings yet
- Capítulo 11 SerdevDocument19 pagesCapítulo 11 SerdevErik BrooksNo ratings yet
- Knee Arthroscopy_ an Up-To-Date Guide-Springer (2021)Document370 pagesKnee Arthroscopy_ an Up-To-Date Guide-Springer (2021)Hugo BustamanteNo ratings yet
- Upper ExtremityDocument22 pagesUpper ExtremityNiarti Ulan SariNo ratings yet
- Lifting SerdevDocument372 pagesLifting SerdevErik BrooksNo ratings yet
- Jin Goo Kim - Knee Arthroscopy - An Up-to-Date Guide-Springer (2021)Document370 pagesJin Goo Kim - Knee Arthroscopy - An Up-to-Date Guide-Springer (2021)Fernando FernandezNo ratings yet
- Basic and Advanced Operative Techniques in Orthognatic SurgeryDocument23 pagesBasic and Advanced Operative Techniques in Orthognatic SurgeryAndrea Cárdenas SandovalNo ratings yet
- Mechanical Design and Trajectory Planning of A Lower Limb Rehabilitation Robot With A Variable WorkspaceDocument13 pagesMechanical Design and Trajectory Planning of A Lower Limb Rehabilitation Robot With A Variable Workspacetanvir anwarNo ratings yet
- We Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsDocument27 pagesWe Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For Scientistsfebyan yohanesNo ratings yet
- Basic Knee Arthroscopy: Surface Anatomy and Portal PlacementDocument2 pagesBasic Knee Arthroscopy: Surface Anatomy and Portal PlacementΗΛΙΑΣ ΠΑΛΑΙΟΧΩΡΛΙΔΗΣNo ratings yet
- Basic Knee Arthroscopy Part 2Document2 pagesBasic Knee Arthroscopy Part 2Diego BellingNo ratings yet
- We Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsDocument31 pagesWe Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsmustafasacarNo ratings yet
- Advanced Techniques of Endoscopic Lumbar Spine SurgeryFrom EverandAdvanced Techniques of Endoscopic Lumbar Spine SurgeryHyeun Sung KimNo ratings yet
- Ankle Joint Arthroscopy: A Step-by-Step GuideFrom EverandAnkle Joint Arthroscopy: A Step-by-Step GuideFrancesco AllegraNo ratings yet
- Part 1 Introduction 1Document17 pagesPart 1 Introduction 1Mahmoud AlnaserNo ratings yet
- Subtalar Arthrodesis Van Dijck 2012Document7 pagesSubtalar Arthrodesis Van Dijck 2012liviu tomoiagaNo ratings yet
- Capítulo 15Document19 pagesCapítulo 15Erik BrooksNo ratings yet
- Endoscopy of the Hip and Knee: Principle and PracticeFrom EverandEndoscopy of the Hip and Knee: Principle and PracticeTun Hing LuiNo ratings yet
- 1 s2.0 S2212628721002589 MainDocument6 pages1 s2.0 S2212628721002589 MainEvans JohnNo ratings yet
- We Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsDocument13 pagesWe Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsSd HelNo ratings yet
- Prosthetic Upper LimbDocument5 pagesProsthetic Upper LimbNimesh Gunasekera100% (1)
- We Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsDocument25 pagesWe Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsKanchit SuwanswadNo ratings yet
- Yau Et Al 2022 Swelling Assessment After Total Knee ArthroplastyDocument10 pagesYau Et Al 2022 Swelling Assessment After Total Knee ArthroplastyCláudia SilvaNo ratings yet
- World's Largest Science, Technology & Medicine Open Access Book PublisherDocument15 pagesWorld's Largest Science, Technology & Medicine Open Access Book PublisherOrhan RamazanNo ratings yet
- Arthroscopic Treatment of Anterosuperior Rotator CDocument8 pagesArthroscopic Treatment of Anterosuperior Rotator CGabriel RojasNo ratings yet
- 1 s2.0 S2212628721000864 MainDocument5 pages1 s2.0 S2212628721000864 MainLuthfi LazuardiNo ratings yet
- Prosthetic Hand Research PaperDocument5 pagesProsthetic Hand Research Papergpxmlevkg100% (1)
- Medi 101 E31809Document3 pagesMedi 101 E31809supachoke NivesNo ratings yet
- Double-Pedicle Propeller Flap For Reconstruction of The Foot and Ankle: Anatomical Study and Clinical ApplicationsDocument12 pagesDouble-Pedicle Propeller Flap For Reconstruction of The Foot and Ankle: Anatomical Study and Clinical ApplicationsWulan PurnamiNo ratings yet
- Robotic Colon Surgery: The Peoria ExperienceDocument16 pagesRobotic Colon Surgery: The Peoria ExperiencepingusNo ratings yet
- Arthroscopic Synovectomy of The Hip Joint: The Regional Surgical TechniqueDocument7 pagesArthroscopic Synovectomy of The Hip Joint: The Regional Surgical TechniqueMoustafa MohamedNo ratings yet
- UCLA Upper Extremity Amputations Manual - Sholder ProsthesisDocument39 pagesUCLA Upper Extremity Amputations Manual - Sholder ProsthesisAlaa SalamNo ratings yet
- Elbow Arthroscopy (2013, Springer-Verlag Berlin Heidelberg)Document131 pagesElbow Arthroscopy (2013, Springer-Verlag Berlin Heidelberg)Joaquin Villagra Jara100% (2)
- Early Outcome After The Use of The Triceps Fascia Flap in Interposition Elbow Arthroplasty A Novel Method in The Treatment of Post-Traumatic Elbow StiffnessDocument6 pagesEarly Outcome After The Use of The Triceps Fascia Flap in Interposition Elbow Arthroplasty A Novel Method in The Treatment of Post-Traumatic Elbow StiffnessJohannes CordeNo ratings yet
- Capítulo 16Document15 pagesCapítulo 16Erik BrooksNo ratings yet
- Bionic Limb ReconstructionFrom EverandBionic Limb ReconstructionOskar C. AszmannNo ratings yet
- Long Head Biceps Tendondnatural Patch For Massive Irreparable Rotator Cuff TearsDocument6 pagesLong Head Biceps Tendondnatural Patch For Massive Irreparable Rotator Cuff TearsDita Putri DamayantiNo ratings yet
- Troncossi-et-al_GEF-2012_v1_UMDocument11 pagesTroncossi-et-al_GEF-2012_v1_UMAnh HuyNo ratings yet
- Unit 1: Rehabilitation EngineeringDocument12 pagesUnit 1: Rehabilitation EngineeringPrasidha PrabhuNo ratings yet
- Chapterpdf Download635476105037 4Document20 pagesChapterpdf Download635476105037 4Abhishek JhaNo ratings yet
- A Removable Class III Traction Appliance For Early Class III TreatmentDocument11 pagesA Removable Class III Traction Appliance For Early Class III TreatmentcdentistacesarmNo ratings yet
- World's Largest Science, Technology & Medicine Open Access Book PublisherDocument38 pagesWorld's Largest Science, Technology & Medicine Open Access Book PublisherAyuAnatrieraNo ratings yet
- Prosthetic DevicesDocument40 pagesProsthetic DevicesRania ANo ratings yet
- Tendon Transfer Surgery: Analysis and Simulation With Opensim 3.3 SoftwareDocument2 pagesTendon Transfer Surgery: Analysis and Simulation With Opensim 3.3 SoftwareJeffllanoNo ratings yet
- 2135-Article Text-12201-1-10-20230403Document9 pages2135-Article Text-12201-1-10-20230403LeiNo ratings yet
- Material Assignment in Finite Element Modeling Heterogeneous Properties of The Mandibular BoneDocument6 pagesMaterial Assignment in Finite Element Modeling Heterogeneous Properties of The Mandibular BoneLeiNo ratings yet
- 髋关节置换的三维有限元分析Document4 pages髋关节置换的三维有限元分析LeiNo ratings yet
- AcetabularCupPositioningduringTotalHipReplacementinOsteoarthritisSecondarytoDevelopmentalDysplasiaoftheHip aReviewoftheLiteratureDocument8 pagesAcetabularCupPositioningduringTotalHipReplacementinOsteoarthritisSecondarytoDevelopmentalDysplasiaoftheHip aReviewoftheLiteratureLeiNo ratings yet
- Journal of Orthopaedic Translation: Lin Xu, Hao Qin, Jia Tan, Zhilin Cheng, Xiang Luo, Haitao Tan, Wenhua HuangDocument7 pagesJournal of Orthopaedic Translation: Lin Xu, Hao Qin, Jia Tan, Zhilin Cheng, Xiang Luo, Haitao Tan, Wenhua HuangLeiNo ratings yet
- Midterm Exam Reviewer: Surgical Handwashing QuizDocument9 pagesMidterm Exam Reviewer: Surgical Handwashing QuizOfficially RandomNo ratings yet
- Hyperfunctional Voice DisordersDocument11 pagesHyperfunctional Voice DisordersJam PNo ratings yet
- Wrap Book A4Document27 pagesWrap Book A4doscribe100% (1)
- Tapping Volcanic Energy for Human UseDocument9 pagesTapping Volcanic Energy for Human UseThartson Oliveros MagdadaroNo ratings yet
- Ventilation System Comparison - Constant Air Volume (CAV) and Variable Air Volume (VAV)Document15 pagesVentilation System Comparison - Constant Air Volume (CAV) and Variable Air Volume (VAV)ankurNo ratings yet
- BKTK-2010, Failure in Material ConstructionsDocument17 pagesBKTK-2010, Failure in Material ConstructionsSorulay Way-neyNo ratings yet
- Wörterbuch Der Humanbiologie - Dictionary of Human Biology - Deutsch - Englisch - Englisch - Deutsch. English - German - German - English (PDFDrive)Document1,002 pagesWörterbuch Der Humanbiologie - Dictionary of Human Biology - Deutsch - Englisch - Englisch - Deutsch. English - German - German - English (PDFDrive)MilaNo ratings yet
- RR No. 6-2015 PDFDocument5 pagesRR No. 6-2015 PDFErlene CompraNo ratings yet
- Candidate 1 (Reservoir Engineering Panel) : ONGC SAMPLE INTERVIEW QUESTIONS (Based Upon Memory of Appeared Candidates)Document3 pagesCandidate 1 (Reservoir Engineering Panel) : ONGC SAMPLE INTERVIEW QUESTIONS (Based Upon Memory of Appeared Candidates)Neha AhiraoNo ratings yet
- Supplying Ready Mix in Southeast Asia - Adapting Concrete Mix Design for Hot, Tropical WeatherDocument2 pagesSupplying Ready Mix in Southeast Asia - Adapting Concrete Mix Design for Hot, Tropical Weathermixtoes7647No ratings yet
- Neonatal Ventilation, Step by StepDocument99 pagesNeonatal Ventilation, Step by StepMarely Ovando Castillo93% (14)
- Stanley - Your Voice (1957) PDFDocument396 pagesStanley - Your Voice (1957) PDFŠašavi Sam MajmunNo ratings yet
- Dupont Heir Sexually Abuses DaughterDocument3 pagesDupont Heir Sexually Abuses DaughterJuandelaCruzNo ratings yet
- The Federal Environmental Protection Authority: May 2004 Addis Ababa EthiopiaDocument44 pagesThe Federal Environmental Protection Authority: May 2004 Addis Ababa Ethiopiayared0% (1)
- Silver Rain Svetlana Perevalova PDFDocument9 pagesSilver Rain Svetlana Perevalova PDFAndrea Koumarian100% (1)
- Grade 5. Unit 15Document6 pagesGrade 5. Unit 15Đình ThuậnNo ratings yet
- Detox 101Document31 pagesDetox 101Botoşanu Diana-LarisaNo ratings yet
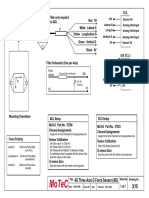
- Filter and wiring schematic for 3-axis ADL G-force sensorDocument1 pageFilter and wiring schematic for 3-axis ADL G-force sensorJuan Ramón Pérez LorenzoNo ratings yet
- Low Noise Pseudomorphic HEMT Technical DataDocument4 pagesLow Noise Pseudomorphic HEMT Technical Datahendpraz88No ratings yet
- 20090716FoxReiki PDFDocument40 pages20090716FoxReiki PDFAgustina RomeroNo ratings yet
- Simplex 4100ES 5 Days Customer TrainingDocument1 pageSimplex 4100ES 5 Days Customer TrainingBrahmantyo HadiprasetyoNo ratings yet
- Concrete Pump Hose TDSDocument2 pagesConcrete Pump Hose TDSAlaa Abu KhurjNo ratings yet
- Group 3Document11 pagesGroup 3Sharp MIER TVNo ratings yet
- Discover the training secrets of legendary bodybuildersDocument129 pagesDiscover the training secrets of legendary bodybuildersfatmir100% (7)
- Chapter 5 Integumentary Study GuideDocument3 pagesChapter 5 Integumentary Study GuideSuperjunior8No ratings yet
- Cost Control ReviewerDocument13 pagesCost Control ReviewerMatthew Ivan HerreraNo ratings yet
- EMBRYOLOGYDocument4 pagesEMBRYOLOGYbhagavan prasadNo ratings yet
- FORM HSE MATRIX TRAINING (Contoh)Document1 pageFORM HSE MATRIX TRAINING (Contoh)Hifni GhazaliNo ratings yet
- Facilitating Civic Engagement Through Consultation: Learning From Local Communities Through The NHI-Accountability Project in South AfricaDocument64 pagesFacilitating Civic Engagement Through Consultation: Learning From Local Communities Through The NHI-Accountability Project in South AfricaOxfamNo ratings yet
- Codex CRD26Document9 pagesCodex CRD26arely svetlana gaspar badilloNo ratings yet