You might also like
- Corynebacterium Diphtheriae: A Paradigm of The Toxigenic Infectious DiseasesDocument20 pagesCorynebacterium Diphtheriae: A Paradigm of The Toxigenic Infectious DiseasesRahma FatmawatiNo ratings yet
- Foundations in Microbiology: The Gram-Positive Bacilli of Medical Importance TalaroDocument70 pagesFoundations in Microbiology: The Gram-Positive Bacilli of Medical Importance TalaroAgathaNo ratings yet
- CORYNEBACTERIUMDocument22 pagesCORYNEBACTERIUMHamidreza RahmaniNo ratings yet
- CorynebacteriumDocument43 pagesCorynebacteriumIsak Isak Isak0% (1)
- Gram Positive RodsDocument74 pagesGram Positive RodsSophia E. BucarileNo ratings yet
- Airborne Bacterial Infection 6-10Document10 pagesAirborne Bacterial Infection 6-10Ashar AhmadNo ratings yet
- Corynebacterium DiphtheriaeDocument27 pagesCorynebacterium DiphtheriaeBarkavi 9620No ratings yet
- They Also Play The Role of Virulence Factors: Transmission Is Person To Person by Respiratory AerosolDocument5 pagesThey Also Play The Role of Virulence Factors: Transmission Is Person To Person by Respiratory Aerosolsm5315213No ratings yet
- Aerobes Chapter 12Document6 pagesAerobes Chapter 12Kristine BoholstNo ratings yet
- Reviewer in Micro para Lec FinalsDocument9 pagesReviewer in Micro para Lec FinalsJohn Carl CastilloNo ratings yet
- DiphtheriaDocument64 pagesDiphtheria2z5t98j7h9No ratings yet
- Lecture 9. Neisseria GonorrhoeaeDocument81 pagesLecture 9. Neisseria GonorrhoeaeHadiqa ArshadNo ratings yet
- Eukaryotic Diseases - 06Document33 pagesEukaryotic Diseases - 06Vien WhitlockNo ratings yet
- HandlerDocument32 pagesHandlerJessabel Taylan GalanoNo ratings yet
- Foundations in Microbiology: The Cocci of Medical Importance TalaroDocument71 pagesFoundations in Microbiology: The Cocci of Medical Importance TalaroOdurNo ratings yet
- Public Health Officers C1: TetanusDocument64 pagesPublic Health Officers C1: Tetanusmamaru bantieNo ratings yet
- 10 Anti InfectivesDocument29 pages10 Anti InfectivesFrançoise BNo ratings yet
- Corynebacterium Diphtheria: Zainab A. AldhaherDocument41 pagesCorynebacterium Diphtheria: Zainab A. Aldhaherمروه عماد عيسىNo ratings yet
- wk11 INFECTIOUS DISORDER PART TWODocument52 pageswk11 INFECTIOUS DISORDER PART TWOclaire yowsNo ratings yet
- 8 Clostridial InfectionsDocument39 pages8 Clostridial InfectionsHariharanNo ratings yet
- Chronic InfectionsDocument60 pagesChronic Infectionsnaveena reddyNo ratings yet
- It 38 Microbiology in Obgyn 24Document146 pagesIt 38 Microbiology in Obgyn 24dhjekwkwNo ratings yet
- Corynebacterium Diphteriae: 3 Year Pharmacy, Semester 2, 2021Document20 pagesCorynebacterium Diphteriae: 3 Year Pharmacy, Semester 2, 2021Xing YuNo ratings yet
- BDS - Corynebacterium (Autosaved)Document35 pagesBDS - Corynebacterium (Autosaved)Just a PersonNo ratings yet
- Cestodes: - Phylum Platyhelminthes (Flatworms)Document23 pagesCestodes: - Phylum Platyhelminthes (Flatworms)ruben6mNo ratings yet
- Aerobic Non-Spore Forming Gram-Positive BacilliDocument31 pagesAerobic Non-Spore Forming Gram-Positive BacilliCagar Irwin TaufanNo ratings yet
- NeisseriaDocument32 pagesNeisseriaKeshant SamarooNo ratings yet
- Bac NotesDocument22 pagesBac NotesK PrashasthaNo ratings yet
- Diphteria, ListeriaDocument20 pagesDiphteria, ListeriaLore LorenaNo ratings yet
- Foundations in Microbiology: TalaroDocument65 pagesFoundations in Microbiology: Talaromertx013No ratings yet
- Diphtheria: Sabah Mohsin Al-Maamuri MDDocument3 pagesDiphtheria: Sabah Mohsin Al-Maamuri MDAmmar AlnajjarNo ratings yet
- Non Spore Forming, Nonbranching Catalase Positive BacilliDocument5 pagesNon Spore Forming, Nonbranching Catalase Positive BacilliFaithNo ratings yet
- Agents of Respiratory DiseaseDocument25 pagesAgents of Respiratory DiseaseAbid AliNo ratings yet
- Monkey Pox-FinalDocument23 pagesMonkey Pox-FinalnirmalaspandagaleNo ratings yet
- Ectoparasites and Parasites On Human's Skin/body Surface Parasitology DepartmentDocument35 pagesEctoparasites and Parasites On Human's Skin/body Surface Parasitology DepartmentLydia KosasihNo ratings yet
- Dm-Lecture 4-11-23Document28 pagesDm-Lecture 4-11-23s.zainabtanweerNo ratings yet
- Mikrobiologi Dasar (DR - Latre)Document50 pagesMikrobiologi Dasar (DR - Latre)wawanNo ratings yet
- RabiesDocument4 pagesRabiesJamie FabianiaNo ratings yet
- Non Spore Forming AnerobDocument75 pagesNon Spore Forming AnerobMahendra SatriaNo ratings yet
- Exotoxic Model Corynebacterium DiphteriaeDocument37 pagesExotoxic Model Corynebacterium Diphteriaekohinoor815256100% (1)
- Diphtheria NUN NOV 2023Document61 pagesDiphtheria NUN NOV 2023NUBWA MEDUGUNo ratings yet
- Pathogenic Gram Negative CocciiDocument31 pagesPathogenic Gram Negative Cocciitemesgensemahegn55No ratings yet
- This Child Has Had A Sore Throat and Fever For 3 Days. The Appearance of The Throat Is Shown. What Do You See?Document62 pagesThis Child Has Had A Sore Throat and Fever For 3 Days. The Appearance of The Throat Is Shown. What Do You See?Ivan KurniawanNo ratings yet
- Microbial Diseases of The Nervous System: DR Sonnie P. Talavera 08162009 OlfuDocument162 pagesMicrobial Diseases of The Nervous System: DR Sonnie P. Talavera 08162009 Olfuone_nd_onlyu0% (1)
- Communicable DiseaseDocument32 pagesCommunicable Diseasekimberly shayneNo ratings yet
- Rabies 2Document51 pagesRabies 2Vanlal RemruatiNo ratings yet
- DiphtheriaDocument3 pagesDiphtheriakpkr603No ratings yet
- Lecturer 3: Warning!!!! This Should Not Replace Your Note or Textbook in AnyformDocument13 pagesLecturer 3: Warning!!!! This Should Not Replace Your Note or Textbook in AnyformHabibNo ratings yet
- ACFrOgAegfbheMg8rqEJ3FF6QO358DrkR G4HUGyi5cjuvj3A15Db9TAgMHCztpPGbxKvqdfItxDDpVELqrY-glc7neG334huie5vHY911yGvh6kn DzxjMIyT7 RpfUdjFVZk1xf1N5v5izuboiDocument33 pagesACFrOgAegfbheMg8rqEJ3FF6QO358DrkR G4HUGyi5cjuvj3A15Db9TAgMHCztpPGbxKvqdfItxDDpVELqrY-glc7neG334huie5vHY911yGvh6kn DzxjMIyT7 RpfUdjFVZk1xf1N5v5izuboiansam hirbaweNo ratings yet
- Diseases of The External EarDocument20 pagesDiseases of The External EarFabian LitetaNo ratings yet
- Canine Distemper: Hard Pad Disease, Canine InfluenzaDocument11 pagesCanine Distemper: Hard Pad Disease, Canine InfluenzaDr-Hassan SaeedNo ratings yet
- Family NeisseriaDocument38 pagesFamily NeisseriakavyaNo ratings yet
- LeprosyDocument22 pagesLeprosyDaniel OkakaNo ratings yet
- Fungi & VirusDocument3 pagesFungi & VirusJazz On WattpadNo ratings yet
- Subcutaneous MycosesDocument34 pagesSubcutaneous MycosesNUBWA MEDUGUNo ratings yet
- Foundations in Microbiology: TalaroDocument71 pagesFoundations in Microbiology: Talaromertx013No ratings yet
- Common Infections BDS4124Document25 pagesCommon Infections BDS4124NouraHabiba28No ratings yet
- Sexually Transmitted Infections 19-21Document4 pagesSexually Transmitted Infections 19-21Ashar AhmadNo ratings yet
- DIPHTHERIADocument12 pagesDIPHTHERIANununNo ratings yet
- BSRM Ultima BrochureDocument2 pagesBSRM Ultima BrochuresaifuzzamanNo ratings yet
- 9701 Nos Ps 23Document5 pages9701 Nos Ps 23Hubbak KhanNo ratings yet
- Fortnite Task Courier Pack 1500 V Bucks - BuscarDocument1 pageFortnite Task Courier Pack 1500 V Bucks - Buscariancard321No ratings yet
- Bill of Quantities 16FI0009Document1 pageBill of Quantities 16FI0009AJothamChristianNo ratings yet
- Final - Anarchy One-Sheet Sell SheetDocument2 pagesFinal - Anarchy One-Sheet Sell SheetMaddanie WijayaNo ratings yet
- Eng Notes2Document10 pagesEng Notes2Arti KapurNo ratings yet
- Peanut AllergyDocument4 pagesPeanut AllergyLNICCOLAIONo ratings yet
- Worked Solution Paper5 A LevelDocument8 pagesWorked Solution Paper5 A LevelBhoosan AncharazNo ratings yet
- Guidelines For Doing Business in Grenada & OECSDocument14 pagesGuidelines For Doing Business in Grenada & OECSCharcoals Caribbean GrillNo ratings yet
- Diagnosis ListDocument1 pageDiagnosis ListSenyorita KHayeNo ratings yet
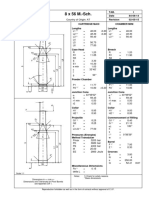
- 8 X 56 M.-SCH.: Country of Origin: ATDocument1 page8 X 56 M.-SCH.: Country of Origin: ATMohammed SirelkhatimNo ratings yet
- FluteDocument13 pagesFlutefisher3910% (1)
- BSNL BillDocument3 pagesBSNL BillKaushik GurunathanNo ratings yet
- 02 CT311 Site WorksDocument26 pages02 CT311 Site Worksshaweeeng 101No ratings yet
- Eje Delantero Fxl14 (1) .6Document2 pagesEje Delantero Fxl14 (1) .6Lenny VirgoNo ratings yet
- Springs: All India Distributer of NienhuisDocument35 pagesSprings: All India Distributer of NienhuisIrina DroliaNo ratings yet
- 16 - Ocean Currents & Salinity Interactive NotebookDocument23 pages16 - Ocean Currents & Salinity Interactive NotebookRaven BraymanNo ratings yet
- HangersSupportsReferenceDataGuide PDFDocument57 pagesHangersSupportsReferenceDataGuide PDFIndra RosadiNo ratings yet
- Lecture 19 Code Standards and ReviewDocument27 pagesLecture 19 Code Standards and ReviewAdhil Ashik vNo ratings yet
- Emerging Technology SyllabusDocument6 pagesEmerging Technology Syllabussw dr100% (4)
- Chemical & Ionic Equilibrium Question PaperDocument7 pagesChemical & Ionic Equilibrium Question PapermisostudyNo ratings yet
- Fce Use of English 1 Teacher S Book PDFDocument2 pagesFce Use of English 1 Teacher S Book PDFOrestis GkaloNo ratings yet
- Payment of Wages 1936Document4 pagesPayment of Wages 1936Anand ReddyNo ratings yet
- Operating Instructions: Rotary Lobe PumpDocument77 pagesOperating Instructions: Rotary Lobe PumpRuslan SlusarNo ratings yet
- Kiraan Supply Mesin AutomotifDocument6 pagesKiraan Supply Mesin Automotifjamali sadatNo ratings yet
- Vq40de Service ManualDocument257 pagesVq40de Service Manualjaumegus100% (4)
- Communication Skill - Time ManagementDocument18 pagesCommunication Skill - Time ManagementChấn NguyễnNo ratings yet
- Index: © Christopher Pitt 2018 C. Pitt, The Definitive Guide To AdonisjsDocument5 pagesIndex: © Christopher Pitt 2018 C. Pitt, The Definitive Guide To AdonisjsZidi BoyNo ratings yet
- Equilibrium of A Rigid BodyDocument30 pagesEquilibrium of A Rigid BodyChristine Torrepenida RasimoNo ratings yet
- APJ Abdul Kalam Success StoryDocument1 pageAPJ Abdul Kalam Success StorySanjaiNo ratings yet