You might also like
- UrolithiasisDocument135 pagesUrolithiasisHaziq HussainiNo ratings yet
- MNT Penyakit GinjalDocument41 pagesMNT Penyakit GinjalNurfitriana DwiNo ratings yet
- Hepatology Case PresentationDocument48 pagesHepatology Case PresentationHajar HossamNo ratings yet
- 1 - GueDocument24 pages1 - GueQasmNo ratings yet
- Multiple Choice Questions (20 Points)Document8 pagesMultiple Choice Questions (20 Points)ODESSEY SERQUI�ANo ratings yet
- Metabolic DisordersDocument59 pagesMetabolic DisordersKeannu Havana100% (1)
- The Diseases of The Liver: Department of Pediatric Allergy, Gastroenterology and NutritionDocument125 pagesThe Diseases of The Liver: Department of Pediatric Allergy, Gastroenterology and NutritionlindaNo ratings yet
- NCM 118 - CCN - THEORY - MidtermsDocument19 pagesNCM 118 - CCN - THEORY - MidtermsSTEFFANIE VALE BORJANo ratings yet
- Urine AnalysisDocument42 pagesUrine AnalysisajaysomNo ratings yet
- Biochemical Investigation of Renal FunctionDocument34 pagesBiochemical Investigation of Renal FunctionUhuebor DavidNo ratings yet
- Drugs For GoutDocument29 pagesDrugs For GoutSsempijja Joshua BuyinzaNo ratings yet
- Renal SystemDocument20 pagesRenal SystemRahul DasNo ratings yet
- Acute Renal Failure Case Presentation GRP 3Document60 pagesAcute Renal Failure Case Presentation GRP 3varish100% (1)
- Chemical Examination of UrineDocument46 pagesChemical Examination of UrineH GondaliyaNo ratings yet
- Inborn Errors of MetabolismDocument2 pagesInborn Errors of MetabolismLode DeocadesNo ratings yet
- Renal Tubules Modify Glomerular Filtrate: Reabsorption of High Threshold SubstancesDocument44 pagesRenal Tubules Modify Glomerular Filtrate: Reabsorption of High Threshold SubstancesajaysomNo ratings yet
- Abnormal Constituents of Urine Interpretation PracticalDocument42 pagesAbnormal Constituents of Urine Interpretation PracticalTEJASWI ModiNo ratings yet
- Chronic KidneyDocument40 pagesChronic KidneyAni Budiati Sehat SejahteraNo ratings yet
- Urine AnalysisDocument41 pagesUrine AnalysisAjay SomeshwarNo ratings yet
- Formation of Urine: NephronDocument44 pagesFormation of Urine: NephronajaysomNo ratings yet
- Urine AnalysisDocument31 pagesUrine AnalysisajaysomNo ratings yet
- Chronic Kidney Disease (CKD) : Diabetes High Blood Pressure Responsible For Up To Two-Thirds GlomerulonephritisDocument6 pagesChronic Kidney Disease (CKD) : Diabetes High Blood Pressure Responsible For Up To Two-Thirds GlomerulonephritisKyle Ü D. CunanersNo ratings yet
- Rta Final Year 23.2.23Document36 pagesRta Final Year 23.2.23S.ayesh HasanNo ratings yet
- URINALYSISDocument80 pagesURINALYSISredr7131No ratings yet
- Obstructive Jaundice: DR Nanteza SumayiyaDocument26 pagesObstructive Jaundice: DR Nanteza SumayiyaNinaNo ratings yet
- Clinical Approach To Jaundice (GSH)Document19 pagesClinical Approach To Jaundice (GSH)handikaNo ratings yet
- Diseases of The GallbladderDocument5 pagesDiseases of The GallbladdertristineNo ratings yet
- Urine AnalysisDocument33 pagesUrine AnalysisajaysomNo ratings yet
- Gout 131015051453 Phpapp01 PDFDocument26 pagesGout 131015051453 Phpapp01 PDFReny Rony BersaudaraNo ratings yet
- 2 5463111801086427966Document13 pages2 5463111801086427966haidernadhem57No ratings yet
- Stoolexamination DR 160521051722Document86 pagesStoolexamination DR 160521051722kathrynNo ratings yet
- Acute Renal FailureDocument45 pagesAcute Renal FailureRubinNo ratings yet
- Normal Liver Physiology: Substancesthese Substances Have Entered The Blood Supply Either Through Production byDocument8 pagesNormal Liver Physiology: Substancesthese Substances Have Entered The Blood Supply Either Through Production byad-adNo ratings yet
- Renal Function TestsDocument34 pagesRenal Function TestsMandavi HindNo ratings yet
- Urinalysis (Part-2) Constituents of Urine: AbnormalDocument49 pagesUrinalysis (Part-2) Constituents of Urine: AbnormalArnab GhoshNo ratings yet
- Analysis of Abnormal Urine NotesDocument6 pagesAnalysis of Abnormal Urine Notesahteshammirji575No ratings yet
- 4 BodyDocument35 pages4 Bodysinte beyuNo ratings yet
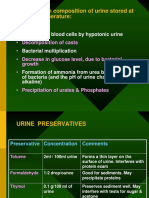
- Changes in Composition of Urine Stored at Room TemperatureDocument39 pagesChanges in Composition of Urine Stored at Room TemperatureAjay SomeshwarNo ratings yet
- Glycosuria: I. Diabetic: II. Non-DiabeticDocument21 pagesGlycosuria: I. Diabetic: II. Non-DiabeticajaysomNo ratings yet
- Chronic Kidney DiseaseDocument14 pagesChronic Kidney DiseaseGabrielle Frances FernandezNo ratings yet
- Potassium ImbalancesDocument82 pagesPotassium ImbalancesManmeet SNo ratings yet
- What Is: Acute Renal Failure Acute Kidney InjuryDocument32 pagesWhat Is: Acute Renal Failure Acute Kidney InjuryCiedelle Honey Lou DimaligNo ratings yet
- 3.acute Liver Failure Without AudioDocument42 pages3.acute Liver Failure Without AudioMohamed ElkadyNo ratings yet
- MS AddsDocument4 pagesMS Addsapi-3731294No ratings yet
- URINALYSISDocument63 pagesURINALYSISMedah Naserian100% (2)
- Renal Pathophysiology PDFDocument52 pagesRenal Pathophysiology PDFzoher al naeemeNo ratings yet
- Renal Failure March 2020Document46 pagesRenal Failure March 2020dicksonsamboNo ratings yet
- SPH Surgery Didactics Gallblader To PancreasDocument170 pagesSPH Surgery Didactics Gallblader To PancreasAbegail IbañezNo ratings yet
- RENAL FUNCTION TESTS (Lecture)Document8 pagesRENAL FUNCTION TESTS (Lecture)mulengaemmanuel350No ratings yet
- Analysis of Abnormal UrineDocument12 pagesAnalysis of Abnormal Urinesingonstrings365No ratings yet
- UrinaryDocument3 pagesUrinaryIYA LABAO100% (1)
- Differential Diagnosis of JaundiceDocument4 pagesDifferential Diagnosis of JaundiceVirag PatilNo ratings yet
- ChemistryDocument103 pagesChemistryadis alemNo ratings yet
- Urinalysis 1Document27 pagesUrinalysis 1ullifannuriNo ratings yet
- Glomerular Filtrate: - Water - Crystalloids - Uric Acid - Proteins With Low Mol. Wt. E.G. HB, Myohb, BJ ProteinsDocument42 pagesGlomerular Filtrate: - Water - Crystalloids - Uric Acid - Proteins With Low Mol. Wt. E.G. HB, Myohb, BJ ProteinsajaysomNo ratings yet
- Gagal Ginjal Kronik: Jainuri Erik Pratama, M.Farm - Klin., AptDocument30 pagesGagal Ginjal Kronik: Jainuri Erik Pratama, M.Farm - Klin., ApthudayanaNo ratings yet
- Urine Analysis FinalDocument112 pagesUrine Analysis FinalNischita JayarajNo ratings yet
- Urine AnalysisDocument69 pagesUrine Analysisvinay0717100% (3)
- Liver Cirrhosis, A Simple Guide To The Condition, Treatment And Related DiseasesFrom EverandLiver Cirrhosis, A Simple Guide To The Condition, Treatment And Related DiseasesNo ratings yet
- Mental Health DirectoryDocument88 pagesMental Health DirectoryAbhijit DasNo ratings yet
- Cl2 Material Safety Data SheetDocument11 pagesCl2 Material Safety Data SheetChristian CoboNo ratings yet
- 2020 11 07 XII Economics 1Document17 pages2020 11 07 XII Economics 1Sjft6hd FfNo ratings yet
- My Own Life. Oliver SacksDocument3 pagesMy Own Life. Oliver Sacksajjm100% (4)
- GHH Horoscope PDFDocument46 pagesGHH Horoscope PDFRakesh Kumar BeheraNo ratings yet
- Post Graduate ClinicsDocument113 pagesPost Graduate ClinicsSnehal PatilNo ratings yet
- Healing PowersDocument9 pagesHealing PowersJack Key Chan AntigNo ratings yet
- Self-Injection Classes: Empowering Patients and Decreasing Nursing WorkloadDocument5 pagesSelf-Injection Classes: Empowering Patients and Decreasing Nursing WorkloadIlvita MayasariNo ratings yet
- Penyakit MeniereDocument25 pagesPenyakit MeniereMuhammad Budiman Irpan BachtiarNo ratings yet
- Origin and Importance of GeneticsDocument12 pagesOrigin and Importance of Geneticshuyenthanh1807100% (1)
- Street Corner Secrets by Svati ShahDocument71 pagesStreet Corner Secrets by Svati ShahDuke University Press100% (2)
- PrepositionsDocument10 pagesPrepositionsZahoor Ul HaqNo ratings yet
- Ahmed Proposal2Document34 pagesAhmed Proposal2ahmedabdikerimNo ratings yet
- Atopic Dermatitis: A Guide For Your Family A Guide For Your FamilyDocument20 pagesAtopic Dermatitis: A Guide For Your Family A Guide For Your Familyputri anggunNo ratings yet
- SunCoBe ShampooDocument24 pagesSunCoBe ShampooDong YulNo ratings yet
- Drug StudyDocument14 pagesDrug StudyCj LowryNo ratings yet
- HypothesisDocument4 pagesHypothesisSunny Boy Ng SinadjanNo ratings yet
- Meal Plan Medyo FinalDocument14 pagesMeal Plan Medyo FinalJasha MaeNo ratings yet
- 2022 Field Research Book DAD - 1190 - 28250Document262 pages2022 Field Research Book DAD - 1190 - 28250Diego PalhariniNo ratings yet
- Fitness Calculator Python ProjectDocument12 pagesFitness Calculator Python ProjectNishitha NeelamNo ratings yet
- The Sovereign Remedy: Touch-Pieces and The King's Evil. (Pt. I) / Noel WoolfDocument30 pagesThe Sovereign Remedy: Touch-Pieces and The King's Evil. (Pt. I) / Noel WoolfDigital Library Numis (DLN)No ratings yet
- Ok Sa Deped Divmemo169 s.2018Document19 pagesOk Sa Deped Divmemo169 s.2018Bella MelendresNo ratings yet
- 2 Upper Airway Disorders PDFDocument33 pages2 Upper Airway Disorders PDFMonica BorjaNo ratings yet
- 02 - Recalibrating Gavi 5.0 in Light of COVID-19 and Successful Replenis..Document19 pages02 - Recalibrating Gavi 5.0 in Light of COVID-19 and Successful Replenis..aman_sasanNo ratings yet
- Ferric Carboxymaltose (Hemojet) : Md. Arafat Hossain Brand Executive, SBMD, 01713354512Document5 pagesFerric Carboxymaltose (Hemojet) : Md. Arafat Hossain Brand Executive, SBMD, 01713354512Heranmoy Kumar Bijon100% (1)
- 2020 Article 773Document10 pages2020 Article 773bagas umam alwiNo ratings yet
- Amla As A Health FoodDocument14 pagesAmla As A Health FoodKUNAL MITTALNo ratings yet
- Jpog August 2013 IdDocument51 pagesJpog August 2013 IdHasyim PurwadiNo ratings yet
- IP Group 10 Making Soap Out of Guava LeavesDocument5 pagesIP Group 10 Making Soap Out of Guava LeavesYuriko CaballeroNo ratings yet
- Answers Part 2Document64 pagesAnswers Part 2Rynjeff Lui-Pio100% (1)