You might also like
- Multiple Physical Injuries Secondary To Vehicular AccidentDocument31 pagesMultiple Physical Injuries Secondary To Vehicular AccidentXyrex Nicolas50% (12)
- Pcs Question 1Document21 pagesPcs Question 1Azra MuzafarNo ratings yet
- Excessive Gingival Display Etiology Diagnosis and Treatment Modalities NIR SILBERBERGDocument10 pagesExcessive Gingival Display Etiology Diagnosis and Treatment Modalities NIR SILBERBERGValentina100% (4)
- The Case of Radonda.... KeilaniDocument6 pagesThe Case of Radonda.... KeilaniTrabajos SOSNo ratings yet
- 76 Case StudyDocument7 pages76 Case StudyDon Fablo100% (1)
- AAO Network GlaucomaDocument59 pagesAAO Network Glaucomasafasayed100% (1)
- Ethical Legal Issue TPDocument6 pagesEthical Legal Issue TPapi-664556143No ratings yet
- Mendoza Ethics Paper Mar 19Document6 pagesMendoza Ethics Paper Mar 19api-340294934No ratings yet
- The Slim Book of Health Pearls: The Complete Medical ExaminationFrom EverandThe Slim Book of Health Pearls: The Complete Medical ExaminationNo ratings yet
- Roils Case StudyDocument4 pagesRoils Case Studyapi-530752813No ratings yet
- The COAT & Review Approach: How to recognise and manage unwell patientsFrom EverandThe COAT & Review Approach: How to recognise and manage unwell patientsRating: 5 out of 5 stars5/5 (1)
- Riddiford Ethics Paper Nov17Document6 pagesRiddiford Ethics Paper Nov17api-354529854No ratings yet
- Nurses Compliance With The Five Rights of Medication AdministrationDocument8 pagesNurses Compliance With The Five Rights of Medication AdministrationLuckyhansel CerezoNo ratings yet
- Gonzalez Paper 3 Rough DraftDocument9 pagesGonzalez Paper 3 Rough Draftapi-285287416No ratings yet
- Theory and Application in Transfusion Medicine at A Tertiary-Care InstitutionDocument6 pagesTheory and Application in Transfusion Medicine at A Tertiary-Care InstitutionfegariasNo ratings yet
- HIS-district LaboratoryDocument6 pagesHIS-district LaboratoryEricka GenoveNo ratings yet
- Compiled Osce - R&C IIDocument73 pagesCompiled Osce - R&C IIFaisal MakkiNo ratings yet
- HCE EsssayDocument3 pagesHCE EsssayAeivan Mae SombrioNo ratings yet
- Pre Op MNGMNTDocument22 pagesPre Op MNGMNTsandeepv08No ratings yet
- The Coming Healthcare Revolution: Take Control of Your HealthFrom EverandThe Coming Healthcare Revolution: Take Control of Your HealthNo ratings yet
- Medication ErrorsDocument7 pagesMedication Errorsapi-679663498No ratings yet
- 1 Preoperative Health Status EvaluationDocument21 pages1 Preoperative Health Status EvaluationNuno CoelhoNo ratings yet
- Negligence and MalpracticeDocument7 pagesNegligence and MalpracticejeyndelossantosNo ratings yet
- Establishing a Culture of Patient Safety: Improving Communication, Building Relationships, and Using Quality ToolsFrom EverandEstablishing a Culture of Patient Safety: Improving Communication, Building Relationships, and Using Quality ToolsNo ratings yet
- Ethical Legal Assign 3Document7 pagesEthical Legal Assign 3Armie CapinpinNo ratings yet
- First, Do Less Harm: Confronting the Inconvenient Problems of Patient SafetyFrom EverandFirst, Do Less Harm: Confronting the Inconvenient Problems of Patient SafetyNo ratings yet
- Viewcontent CgiDocument15 pagesViewcontent CgiasandiNo ratings yet
- 76 Case StudyDocument7 pages76 Case Studynavya sharmaNo ratings yet
- Nursing Clinical Case Study AnalysisDocument5 pagesNursing Clinical Case Study Analysisapi-664257988No ratings yet
- Group 3B4 Ethics Case ReportDocument3 pagesGroup 3B4 Ethics Case ReportChris Jardine LiNo ratings yet
- NR Thesis1Document40 pagesNR Thesis1ceicai100% (1)
- Addressing Psychosocial Aspects of Care For Patients With Diabetes Undergoing Limb Salvage SurgeryDocument10 pagesAddressing Psychosocial Aspects of Care For Patients With Diabetes Undergoing Limb Salvage SurgeryAnonymous kdBDppigENo ratings yet
- Clinical Nursing Judgment 1Document5 pagesClinical Nursing Judgment 1api-601489653No ratings yet
- AssignmentDocument3 pagesAssignmentKim Rose SabuclalaoNo ratings yet
- Case Discussion - TruthfulnessDocument10 pagesCase Discussion - Truthfulnessshamsi saad shamsiNo ratings yet
- Week 3 PATIENTS RIGHTS AND RESPONSIBILITIES 19-20Document32 pagesWeek 3 PATIENTS RIGHTS AND RESPONSIBILITIES 19-20maha abdallahNo ratings yet
- Mock Covid Drive Thru ClinicalDocument4 pagesMock Covid Drive Thru Clinicalapi-663470553No ratings yet
- NEUK 1464 (Revised) 1 (Updated)Document21 pagesNEUK 1464 (Revised) 1 (Updated)Sameen ShafaatNo ratings yet
- Evaluacion Del Paciente UrologicoDocument14 pagesEvaluacion Del Paciente UrologicoJhonahanNo ratings yet
- Running Head: CASE STUDY 1Document7 pagesRunning Head: CASE STUDY 1Blessed ItalNo ratings yet
- FNP Module 3Document5 pagesFNP Module 3Jewel Berbano IINo ratings yet
- Professional Nursing Roles and ValuesDocument8 pagesProfessional Nursing Roles and Valuesjingle20No ratings yet
- Lecture 2Document9 pagesLecture 2omarelbihi8No ratings yet
- Medical Technology Grade 11Document3 pagesMedical Technology Grade 11Salma BazziNo ratings yet
- Ebp Final ProjectDocument11 pagesEbp Final Projectapi-577388355No ratings yet
- Bachelor of Nursing Science With HonoursDocument17 pagesBachelor of Nursing Science With Honoursiqmal irfamimiNo ratings yet
- Perioperative NursingDocument36 pagesPerioperative Nursinggrazelantonette.calubNo ratings yet
- The Slim Book of Health Pearls: The Prevention of Medical ErrorsFrom EverandThe Slim Book of Health Pearls: The Prevention of Medical ErrorsNo ratings yet
- Clinical MedicineDocument5 pagesClinical MedicineTimothyNo ratings yet
- Ethics MidtermDocument12 pagesEthics MidtermLoLiTraP KaiNo ratings yet
- Safety Issues: in Health Care SystemDocument31 pagesSafety Issues: in Health Care SystemHaifa Mohammadsali AndilingNo ratings yet
- Ethical Issues in NursingDocument6 pagesEthical Issues in Nursingkayzhel100% (1)
- Capstone Paper 1Document6 pagesCapstone Paper 1api-732900066No ratings yet
- Medical ErrorDocument11 pagesMedical ErrorLakshya BansalNo ratings yet
- How Bureaucracy Can Foster Burnout: Standardization FirstDocument7 pagesHow Bureaucracy Can Foster Burnout: Standardization FirstRakesh ChoudhuryNo ratings yet
- Annotated BibliographyDocument4 pagesAnnotated BibliographyKeii blackhoodNo ratings yet
- Medical Errors Prevention and SafetyDocument15 pagesMedical Errors Prevention and SafetyXavior Sebastian FernandezNo ratings yet
- Volman Ethics Paper March19Document6 pagesVolman Ethics Paper March19api-381505333No ratings yet
- 13McGillJLHealth73 1Document45 pages13McGillJLHealth73 1Jahlin HabbeiNo ratings yet
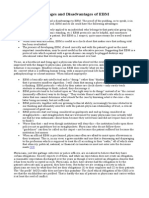
- Summary: Advantages and Disadvantages of EBMDocument3 pagesSummary: Advantages and Disadvantages of EBMAnonymous DA8iQzNo ratings yet
- Lesson 5 Appraising Diagnostic Research StudiesDocument23 pagesLesson 5 Appraising Diagnostic Research StudiesProject MedbooksNo ratings yet
- 19 CR 8411 IngDocument1 page19 CR 8411 IngJorge OrtegaNo ratings yet
- 28b - EMRCOG SUMMARY - STROKE IN PREGNANCY - TOG 2020Document8 pages28b - EMRCOG SUMMARY - STROKE IN PREGNANCY - TOG 2020saeed hasan saeedNo ratings yet
- CURIS® 4 MHZ Radiofrequency Generator - ENT and Head-and-Neck Surgery Solutions - EN - 1339Document11 pagesCURIS® 4 MHZ Radiofrequency Generator - ENT and Head-and-Neck Surgery Solutions - EN - 1339diana mistraNo ratings yet
- Mayfield: Product DescriptionDocument2 pagesMayfield: Product DescriptionGiapril DoniNo ratings yet
- Blunt Chest InjuryDocument61 pagesBlunt Chest InjuryISFAHAN MASULOTNo ratings yet
- Brosur TrilogyDocument7 pagesBrosur TrilogyHendra SetiawanNo ratings yet
- 99.11.26-病歷實作及修改 方川尹醫師Document36 pages99.11.26-病歷實作及修改 方川尹醫師陳瑋毅No ratings yet
- LADocument93 pagesLAkaedeamira_113974100% (2)
- OSCE Checklist ABG SamplingDocument2 pagesOSCE Checklist ABG SamplingPiyali SahaNo ratings yet
- Bronchoscopy and EsophagoscopyA Manual of Peroral Endoscopy and Laryngeal Surgery by Jackson, Chevalier, 1865-1958Document153 pagesBronchoscopy and EsophagoscopyA Manual of Peroral Endoscopy and Laryngeal Surgery by Jackson, Chevalier, 1865-1958Gutenberg.org100% (1)
- Histopathology and Pathogenesis of VascularDocument62 pagesHistopathology and Pathogenesis of VascularSamah AlshamiNo ratings yet
- Coronary ArteriesDocument28 pagesCoronary ArteriesFirst LuckNo ratings yet
- Prevention of Surgical Site Infections: Pola Brenner, Patricio NercellesDocument10 pagesPrevention of Surgical Site Infections: Pola Brenner, Patricio NercellesAmeng GosimNo ratings yet
- C1 Lab 4 - 55654Document23 pagesC1 Lab 4 - 55654anaNo ratings yet
- ECG - ACLS 2020 ModuleDocument68 pagesECG - ACLS 2020 ModuleRasheedAladdinNGuiomala100% (1)
- Hospital Furniture NO Nama Produk Keterangan Price (RP) : Bed PasienDocument14 pagesHospital Furniture NO Nama Produk Keterangan Price (RP) : Bed PasienMonalisa ArmaniNo ratings yet
- Wa Pedi MaleDocument5 pagesWa Pedi MaleMithun ChowdhuryNo ratings yet
- Ojanes 2019121113522570 PDFDocument6 pagesOjanes 2019121113522570 PDFArifudin Cipto HusodoNo ratings yet
- SNACC Cognitive Aids For Neuroanesthetic Emergencies - 9 - 25 - 2020Document13 pagesSNACC Cognitive Aids For Neuroanesthetic Emergencies - 9 - 25 - 2020hkdawnwongNo ratings yet
- Endodontic Clinic Manual 2015 - 1Document134 pagesEndodontic Clinic Manual 2015 - 1Adina Popa100% (2)
- Cap. 10 - RatsDocument17 pagesCap. 10 - RatsNailson JúniorNo ratings yet
- KKKKDocument22 pagesKKKKMARY CLAIRE SUMILHIGNo ratings yet
- Antireflux Surgery Lich-GregoirDocument16 pagesAntireflux Surgery Lich-GregoircristiangelsNo ratings yet
- Matrix RibDocument80 pagesMatrix RibTamara PricilaNo ratings yet
- Infection Control During IV AsesesDocument20 pagesInfection Control During IV AsesesVineeth venuNo ratings yet
- Mary Rose Tolentino Macalinao, RN: Career ObjectiveDocument7 pagesMary Rose Tolentino Macalinao, RN: Career ObjectiveAina De LeonNo ratings yet
- Basic PrincipleDocument92 pagesBasic PrincipleAde SinagaNo ratings yet