You might also like
- Anatomy and Physiology - Dengue FeverDocument3 pagesAnatomy and Physiology - Dengue Feverhael yam62% (13)
- Arteriovenous Fistula Between Descending Aorta and Left Inferior Pulmonary VeinDocument2 pagesArteriovenous Fistula Between Descending Aorta and Left Inferior Pulmonary VeinDavin TakaryantoNo ratings yet
- Criss-Cross Heart With Double-Outlet Right VentricleDocument4 pagesCriss-Cross Heart With Double-Outlet Right Ventriclejuana lopezNo ratings yet
- BCR 2021 241644Document3 pagesBCR 2021 241644Davin TakaryantoNo ratings yet
- Jurnal Coronary Artery FistulaDocument3 pagesJurnal Coronary Artery FistulaRistinyaUnuyNo ratings yet
- 1229 6490 1 PB PDFDocument10 pages1229 6490 1 PB PDFSitti_HazrinaNo ratings yet
- Cavotricuspid Isthmus: Anatomy, Electrophysiology, and Long-Term OutcomeDocument5 pagesCavotricuspid Isthmus: Anatomy, Electrophysiology, and Long-Term Outcomeapi-26166949No ratings yet
- Caso Clinico Sp3Document4 pagesCaso Clinico Sp3eduardoNo ratings yet
- Intralobar Pulmonary Sequestration: Incidental Finding in An Asymptomatic PatientDocument4 pagesIntralobar Pulmonary Sequestration: Incidental Finding in An Asymptomatic PatienteduardoNo ratings yet
- A Case of Tracheal Tumor Masquerading As AsthmaDocument4 pagesA Case of Tracheal Tumor Masquerading As Asthmamastansk84No ratings yet
- USguidedprocedures EditedDocument7 pagesUSguidedprocedures EditedLex Alejandro Jr.No ratings yet
- Right Coronary Artery-Right Atrial Fistula in Right Atrial Myxoma A Rare CombinationDocument3 pagesRight Coronary Artery-Right Atrial Fistula in Right Atrial Myxoma A Rare CombinationAxel Hiram Hernandez PinedaNo ratings yet
- 1rabio (Oo'.: Proceedings MedicineDocument12 pages1rabio (Oo'.: Proceedings MedicineMadhumala KumariNo ratings yet
- Bronchial Artery Pseudoaneurysm and Mediast - 2021 - Archivos de BronconeumologDocument2 pagesBronchial Artery Pseudoaneurysm and Mediast - 2021 - Archivos de BronconeumologMomoh GaiusNo ratings yet
- Utility of Endoscopic Ultrasound in Symptomatic Cut Corners of A ClotDocument3 pagesUtility of Endoscopic Ultrasound in Symptomatic Cut Corners of A ClotDjabhi SpinzzNo ratings yet
- Acute Aortic Syndrome – More in The SpectruDocument5 pagesAcute Aortic Syndrome – More in The Spectrufabiola shoshajNo ratings yet
- Primary Ewing Sarcoma of The Adrenal Gland: A Rare Cause of Abdominal MassDocument6 pagesPrimary Ewing Sarcoma of The Adrenal Gland: A Rare Cause of Abdominal MassAndra KurniantoNo ratings yet
- 5 Arta Al EditorDocument3 pages5 Arta Al EditorJuan José CabezasNo ratings yet
- O-Water PET For Evaluation of Cardiopulmonary Perfusion in Complex Cyanotic Heart DiseaseDocument5 pagesO-Water PET For Evaluation of Cardiopulmonary Perfusion in Complex Cyanotic Heart Diseaseandreaslim2712No ratings yet
- Intercostal Artery Injury Manifested by A Sentinel Pleural ClotDocument2 pagesIntercostal Artery Injury Manifested by A Sentinel Pleural ClotGordana PuzovicNo ratings yet
- Radiology Case ReportsDocument5 pagesRadiology Case ReportsLaila Maria UlfahNo ratings yet
- Main Strem BroncusDocument2 pagesMain Strem BroncusSri BayaniNo ratings yet
- Cardiac RadiologyDocument10 pagesCardiac RadiologyHaluk AlibazogluNo ratings yet
- Diagnosis and Minimally Invasive Treatment of Posterior Fossa Dural Arteriovenous Fistula Presenting Clinically As A Carotid Cavernous FistulaDocument5 pagesDiagnosis and Minimally Invasive Treatment of Posterior Fossa Dural Arteriovenous Fistula Presenting Clinically As A Carotid Cavernous FistulaAthenaeum Scientific PublishersNo ratings yet
- Best Management in Isolated Right Ventricular Hypoplasia With Septal Defects in AdultsDocument7 pagesBest Management in Isolated Right Ventricular Hypoplasia With Septal Defects in AdultsReinaldi octaNo ratings yet
- Uncommon Presentation of Coronary Sinus EndocarditisDocument4 pagesUncommon Presentation of Coronary Sinus EndocarditisAlex MarschallNo ratings yet
- Anatomic Correction of Transposition of The Great Arteries: A S A Result of Mustard's Report, The HemodynamicDocument5 pagesAnatomic Correction of Transposition of The Great Arteries: A S A Result of Mustard's Report, The HemodynamicFarida FaradillaNo ratings yet
- Skeik Et Al 2015 - CirculatoryDocument5 pagesSkeik Et Al 2015 - Circulatorymattlight07No ratings yet
- Ultrasound Imaging of The Arterial System: Prashant Gupta, Shannon Lyons, Sandeep HedgireDocument12 pagesUltrasound Imaging of The Arterial System: Prashant Gupta, Shannon Lyons, Sandeep HedgirePopyNo ratings yet
- Ultrasound of The Thorax (Noncardiac)Document13 pagesUltrasound of The Thorax (Noncardiac)ludiegues752No ratings yet
- Carotid Artery Stenosis ImagingDocument10 pagesCarotid Artery Stenosis ImagingCristhian RuizNo ratings yet
- CIRCULATIONDocument2 pagesCIRCULATIONRVDNo ratings yet
- OMJ Anomalous Systemic Artery To A Normal Lung - A Rare Cause of Hemoptysis in AdultsDocument4 pagesOMJ Anomalous Systemic Artery To A Normal Lung - A Rare Cause of Hemoptysis in AdultsradiologirsckNo ratings yet
- Massive Hemothorax Caused by Intercostal Artery Pseudoaneurysma Case ReportDocument5 pagesMassive Hemothorax Caused by Intercostal Artery Pseudoaneurysma Case ReportAndi Tri SutrisnoNo ratings yet
- Atypical Extralobar Sequestration - JCTDocument4 pagesAtypical Extralobar Sequestration - JCTRafaella AranhaNo ratings yet
- Bedside Lung Ultrasound Versus Chest X-Ray Use in The Emergency DepartmentDocument3 pagesBedside Lung Ultrasound Versus Chest X-Ray Use in The Emergency DepartmentharnellaNo ratings yet
- Journal Radiologi 3Document14 pagesJournal Radiologi 3WinayNayNo ratings yet
- JOURNALDocument4 pagesJOURNALChiara FajardoNo ratings yet
- Anatomical and Pathophysiological Classification of Congenital Heart DiseaseDocument16 pagesAnatomical and Pathophysiological Classification of Congenital Heart DiseasePietro PensoNo ratings yet
- Perivenous Artifact in Thoracic CT Angiography: Effectiveness of Lower Extremity InjectionDocument6 pagesPerivenous Artifact in Thoracic CT Angiography: Effectiveness of Lower Extremity InjectionGordana PuzovicNo ratings yet
- Blanco 2016Document10 pagesBlanco 2016Ananth BalakrishnanNo ratings yet
- Ojmi 2017101715394062Document7 pagesOjmi 2017101715394062Proimagem Santa InêsNo ratings yet
- Case Report: Transient Interruption of ContrastDocument3 pagesCase Report: Transient Interruption of ContrastGordana PuzovicNo ratings yet
- ArcuatoDocument7 pagesArcuatoDaniela PekeNo ratings yet
- Penetrating Gunshot Injury To The Chest With Unusual Intraluminal Passage of The BulletDocument4 pagesPenetrating Gunshot Injury To The Chest With Unusual Intraluminal Passage of The BulletSummaiyahWahabKhanNo ratings yet
- Articulo 20 de OctubreDocument6 pagesArticulo 20 de OctubreAlba PalaciosNo ratings yet
- Large Substernal Thyroid Goiter Associated With Saddle Pulmonary EmbolismDocument3 pagesLarge Substernal Thyroid Goiter Associated With Saddle Pulmonary Embolismsantri safiraNo ratings yet
- Journal Reading - CT of Thoracic Lymph Nodes. Part I Anatomy and DrainageDocument45 pagesJournal Reading - CT of Thoracic Lymph Nodes. Part I Anatomy and DrainageVincentius Henry SundahNo ratings yet
- Quadricuspid Aortic Valve and A Ventricular Septal Defect in A HorseDocument7 pagesQuadricuspid Aortic Valve and A Ventricular Septal Defect in A HorseJacob HaleNo ratings yet
- Adult Choroidal Vein of Galen MalformationDocument5 pagesAdult Choroidal Vein of Galen MalformationSonia Prima Arisa PutriNo ratings yet
- A Rare Case of Unexpected Cardiac Incidentaloma Causing SyncopeDocument4 pagesA Rare Case of Unexpected Cardiac Incidentaloma Causing Syncopeserena7205No ratings yet
- Fallot Tetralogy Imaging Findings With MDCT, Pre and Postoperative FindingsDocument25 pagesFallot Tetralogy Imaging Findings With MDCT, Pre and Postoperative FindingsMusaddad MudjahidNo ratings yet
- Particularities of Scimitar Syndrome in Adult PatientsDocument5 pagesParticularities of Scimitar Syndrome in Adult PatientsIJAR JOURNALNo ratings yet
- Insuffisance Mitrale Apport deDocument2 pagesInsuffisance Mitrale Apport deBrahim PharmNo ratings yet
- Images: Ventricular Septal Defects: Morphology of The Doubly Committed Juxtaarterial and Muscular VariantsDocument19 pagesImages: Ventricular Septal Defects: Morphology of The Doubly Committed Juxtaarterial and Muscular VariantsMarina RotaruNo ratings yet
- Jurnal 1Document4 pagesJurnal 1Ria AngganiNo ratings yet
- Computed Tomography Findings of Kommere - 2014 - Canadian Association of RadioloDocument6 pagesComputed Tomography Findings of Kommere - 2014 - Canadian Association of RadioloChilaka Priyanka1996No ratings yet
- Diag Imagem Shunt PDFDocument5 pagesDiag Imagem Shunt PDFIzabela RodriguesNo ratings yet
- Endovascular en Herida de BalaDocument3 pagesEndovascular en Herida de BalaVero CarpaniNo ratings yet
- CT Scan of The AxillaDocument28 pagesCT Scan of The AxillaObamaNo ratings yet
- Echocardiography English GifDocument77 pagesEchocardiography English GifAlexandra StancuNo ratings yet
- Heart BlockDocument20 pagesHeart BlockSumathi GopinathNo ratings yet
- Lymphatic System SummaryDocument2 pagesLymphatic System SummaryLizbeth Quinn BatangosoNo ratings yet
- Reading ExercisesDocument20 pagesReading Exercisesmuhammad dzikra azidanNo ratings yet
- Blood Supply of BrainDocument49 pagesBlood Supply of BrainDarling Sevenfoldism SynysterNo ratings yet
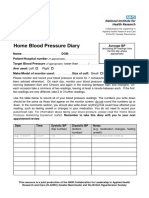
- Home Blood Pressure DiaryDocument2 pagesHome Blood Pressure DiaryCherieNo ratings yet
- Krisis HipertensiDocument29 pagesKrisis HipertensiMuarifNo ratings yet
- Ascending Aortic Elongation and The Risk of DissecDocument8 pagesAscending Aortic Elongation and The Risk of DissecJonathan MarkNo ratings yet
- Chapter 48B - Critical Care of Cerebrovascular DiseaseDocument26 pagesChapter 48B - Critical Care of Cerebrovascular DiseaseDragutin PetrićNo ratings yet
- Part 1 Cva CasesDocument7 pagesPart 1 Cva CasesMicole NatividadNo ratings yet
- Ischemic Heart Disease (IHD)Document35 pagesIschemic Heart Disease (IHD)Ali Akand AsifNo ratings yet
- Reticulo Endothelial SystemDocument15 pagesReticulo Endothelial Systemssdb14No ratings yet
- Prioritization of ProblemsDocument3 pagesPrioritization of ProblemsBLABLEBLIBLOBLUUUNo ratings yet
- Chapter 13 The Heart Lesson Plan For Caroline 1Document3 pagesChapter 13 The Heart Lesson Plan For Caroline 1api-546738847No ratings yet
- A. Cardio: Anatomy & Physiology - A. AnatomyDocument43 pagesA. Cardio: Anatomy & Physiology - A. AnatomyGloryJaneNo ratings yet
- (O. Nelson) Small Animal CardiologyDocument208 pages(O. Nelson) Small Animal CardiologyLoredana Gutu100% (1)
- Vein of Galen MalformationDocument69 pagesVein of Galen MalformationBhupendra GuptaNo ratings yet
- 2019 ESC/EAS Guidelines For The Management of Dyslipidaemias: Lipid Modification To Reduce Cardiovascular Risk: Supplementary DataDocument18 pages2019 ESC/EAS Guidelines For The Management of Dyslipidaemias: Lipid Modification To Reduce Cardiovascular Risk: Supplementary DataElena CosminaNo ratings yet
- Inguinal Lymphnode DissectionDocument35 pagesInguinal Lymphnode Dissectionpravin narkhede100% (3)
- Heart Failure Pelatihan Dokter KeluargaDocument55 pagesHeart Failure Pelatihan Dokter KeluargaDelia NingrumNo ratings yet
- RCSI Clinical Examinations in Medicine 2018-19Document189 pagesRCSI Clinical Examinations in Medicine 2018-19Rebecca MarshallNo ratings yet
- Second Cot Science SixDocument5 pagesSecond Cot Science Sixmaricel isletaNo ratings yet
- Pulse Rate BioDocument3 pagesPulse Rate Biosanique peterkinNo ratings yet
- Thrombolysis For Acute Myocardial Infarction: Clinical Cardiology: New FrontiersDocument15 pagesThrombolysis For Acute Myocardial Infarction: Clinical Cardiology: New FrontiersBinod KumarNo ratings yet
- RCAT WindowDocument2 pagesRCAT WindowEric Jake LimNo ratings yet
- ICU One Pager Fluid Responsiveness v1 2Document1 pageICU One Pager Fluid Responsiveness v1 2liz mNo ratings yet
- 10,11-Arterial Blood Pressure & Its Regulation Team441Document51 pages10,11-Arterial Blood Pressure & Its Regulation Team441saran kNo ratings yet
- 2014 @nucproflib Helen Ryder, GiorgioDocument128 pages2014 @nucproflib Helen Ryder, Giorgioe'Rfan k'AguyaNo ratings yet
- Ficha 12 - Pulse RateDocument2 pagesFicha 12 - Pulse Ratejorgitoperu2014100% (1)