You might also like
- Dopamine Vs EpinephrineDocument11 pagesDopamine Vs EpinephrineAyiek WicaksonoNo ratings yet
- Prednisona Vs ActhDocument7 pagesPrednisona Vs ActhElCanaldeSaadNo ratings yet
- A Novel Risk Analysis of Clinical Reference Dosimetry Based On Failure Modes and Effects AnalysisDocument7 pagesA Novel Risk Analysis of Clinical Reference Dosimetry Based On Failure Modes and Effects AnalysisMichelle LEINo ratings yet
- Efficacy and Safety of SildenafilDocument9 pagesEfficacy and Safety of SildenafilArif Nurhadi AtmokoNo ratings yet
- Nanorifampicin 2Document8 pagesNanorifampicin 2atulskoriNo ratings yet
- Journal 1Document6 pagesJournal 1Ahmad AbqariNo ratings yet
- Comparison of Dexmedetomidine With Propofol As SedativesDocument11 pagesComparison of Dexmedetomidine With Propofol As SedativesMarjorieLCalderónNo ratings yet
- Kran Ich 2014Document7 pagesKran Ich 2014windychyntiaNo ratings yet
- Afamelanotide With NBUVB in VitiligoDocument3 pagesAfamelanotide With NBUVB in VitiligoCHONG WEI SHENGNo ratings yet
- E000557 FullDocument13 pagesE000557 FullMS AKNo ratings yet
- Fphar 12 781084Document12 pagesFphar 12 781084Paulo LemeNo ratings yet
- Relapse Rates With Paliperidone Palmitate in AdultDocument11 pagesRelapse Rates With Paliperidone Palmitate in AdultdryaeonNo ratings yet
- Efficacy and Safety of Dapsone Gel For Acne: A Systematic Review and Meta-AnalysisDocument10 pagesEfficacy and Safety of Dapsone Gel For Acne: A Systematic Review and Meta-AnalysismonikaNo ratings yet
- American Journal of Emergency MedicineDocument12 pagesAmerican Journal of Emergency MedicineSandip MehtaNo ratings yet
- Original Research Article: Anurag Bijalwan, Pradeep Singhal, Syed AltamashDocument7 pagesOriginal Research Article: Anurag Bijalwan, Pradeep Singhal, Syed Altamashagus sukarnaNo ratings yet
- Propranolol em Queimados MetanaliseDocument9 pagesPropranolol em Queimados MetanaliseIsadora PereiraNo ratings yet
- A Systematic Review of The Pharmacokinetics of Antiepileptic Drugs in Neonates With Refractory SeizuresDocument14 pagesA Systematic Review of The Pharmacokinetics of Antiepileptic Drugs in Neonates With Refractory SeizuresAsri RachmawatiNo ratings yet
- Anti-Cancer Activity of Pegylated Liposomal Trans-Anethole On Breast Cancer Cell Lines MCF-7 and T47DDocument5 pagesAnti-Cancer Activity of Pegylated Liposomal Trans-Anethole On Breast Cancer Cell Lines MCF-7 and T47DBashar AliNo ratings yet
- 185852-Article Text-472571-1-10-20190423 PDFDocument9 pages185852-Article Text-472571-1-10-20190423 PDFPablo Segales BautistaNo ratings yet
- Medicine: Acupoint Herbal Patching During Sanfu Days On Reducing Frequency of Acute Asthma Attack in ChildrenDocument7 pagesMedicine: Acupoint Herbal Patching During Sanfu Days On Reducing Frequency of Acute Asthma Attack in ChildrennoviaNo ratings yet
- The Effect of Propanolol and Metformin On Clinical Outcomes in Bu 2023 BurnsDocument9 pagesThe Effect of Propanolol and Metformin On Clinical Outcomes in Bu 2023 BurnsAdrian MoralesNo ratings yet
- Li 2021Document8 pagesLi 2021Intan Adevia RosnaritaNo ratings yet
- PIIS2213260017304745Document10 pagesPIIS2213260017304745Juan Pablo CasanovaNo ratings yet
- Prenatal Exposure To Phthalates and Phenols and Infant en 2018 Environment IDocument12 pagesPrenatal Exposure To Phthalates and Phenols and Infant en 2018 Environment Isiti masita chairuddinNo ratings yet
- Paper SeminarioDocument8 pagesPaper SeminarioKarla Labbe RodriguezNo ratings yet
- 81635793Document13 pages81635793Brock TernovNo ratings yet
- Cost Effectiveness of Dapagliflozinmetformin VersuDocument2 pagesCost Effectiveness of Dapagliflozinmetformin VersuENY RUSMIYATINo ratings yet
- 2018 Wastewater-Based Tracing of Doping Use by The General Population and Amateur AthletesDocument11 pages2018 Wastewater-Based Tracing of Doping Use by The General Population and Amateur Athleteskryylmz.tNo ratings yet
- Cyp2c19, Ugt2b7, Ugt1a8Document8 pagesCyp2c19, Ugt2b7, Ugt1a8Nandit BanawalikarNo ratings yet
- Comparative Study The Effect of Induction of General Anesthesia With Propofol Versus Thiopentone in Pediatric Age Group On Cardiovascular SystemDocument8 pagesComparative Study The Effect of Induction of General Anesthesia With Propofol Versus Thiopentone in Pediatric Age Group On Cardiovascular SystemCentral Asian StudiesNo ratings yet
- English - Daniel Yoseph Pardomuan - Botulinum Toxin-A Therapy Effectivity Compared With Placebo in Overactive Bladder Syndrome Patients Meta-AnalysisDocument7 pagesEnglish - Daniel Yoseph Pardomuan - Botulinum Toxin-A Therapy Effectivity Compared With Placebo in Overactive Bladder Syndrome Patients Meta-AnalysisDaniel YprNo ratings yet
- Advocating For Demonstration of Disease Modification - Have We Been Approaching Clinical Trials in Early Alzheimer Disease Incorrectly?Document2 pagesAdvocating For Demonstration of Disease Modification - Have We Been Approaching Clinical Trials in Early Alzheimer Disease Incorrectly?Lorrane NevesNo ratings yet
- RARE & Orphan Diseases - Epidemiology & Public HealthDocument1 pageRARE & Orphan Diseases - Epidemiology & Public HealthMichael John AguilarNo ratings yet
- P0581 548 Risk Factors of Severity of Dengue.639Document1 pageP0581 548 Risk Factors of Severity of Dengue.639Hendri HariyantoNo ratings yet
- International Journal of Scientific ResearchDocument2 pagesInternational Journal of Scientific ResearchAfnita LestaryNo ratings yet
- Pediatric Acute Asthma Scoring Systems: A Systematic Review and Survey of UK PracticeDocument9 pagesPediatric Acute Asthma Scoring Systems: A Systematic Review and Survey of UK PracticeM Tevfik ÇeviriciNo ratings yet
- Memorandum: Reference ID: 3059531Document4 pagesMemorandum: Reference ID: 3059531joelrequenaNo ratings yet
- 10 1177@0300060519889442Document13 pages10 1177@0300060519889442Glabela Christiana PandangoNo ratings yet
- Immature Platelet Fraction Predicts Early Marrow Recovery in Febrile NeutropeniaDocument13 pagesImmature Platelet Fraction Predicts Early Marrow Recovery in Febrile NeutropeniasulvitaNo ratings yet
- Toxic Effects of Paracetamol On Male Reproductive System of Adult RabbitsDocument16 pagesToxic Effects of Paracetamol On Male Reproductive System of Adult RabbitsEka SupardinataNo ratings yet
- Malaria PK/PD and The Role Pharmacometrics Can Play in The Global Health Arena: Malaria Treatment Regimens For Vulnerable PopulationsDocument15 pagesMalaria PK/PD and The Role Pharmacometrics Can Play in The Global Health Arena: Malaria Treatment Regimens For Vulnerable PopulationsAli DuchuNo ratings yet
- Caldwell Etal 2014 Chemo SphereDocument9 pagesCaldwell Etal 2014 Chemo SphereAiniiSumichelzNo ratings yet
- A Meta-Analysis of Andexanet Alfa and ProthrombinDocument14 pagesA Meta-Analysis of Andexanet Alfa and ProthrombinLuan FerreiraNo ratings yet
- Ijms 40958-2Document8 pagesIjms 40958-2Manolin KinNo ratings yet
- Lidocain and BuvipacainDocument6 pagesLidocain and BuvipacaintinahermantoNo ratings yet
- Impact of Estrogen Type On Cardiovascular Safety of Combined OralDocument12 pagesImpact of Estrogen Type On Cardiovascular Safety of Combined OralMary SuescaNo ratings yet
- RARE & Orphan Diseases - Clinical OutcomesDocument2 pagesRARE & Orphan Diseases - Clinical OutcomesMichael John AguilarNo ratings yet
- Gómez-García 2016Document10 pagesGómez-García 2016Rafaela Queiroz MascarenhasNo ratings yet
- A Meta-Analysis On Intravenous Magnesium Sulphate For Treating Acute AsthmaDocument5 pagesA Meta-Analysis On Intravenous Magnesium Sulphate For Treating Acute AsthmayunitadwiherwatiNo ratings yet
- Friedman 2015Document7 pagesFriedman 2015yunNo ratings yet
- 09 InglesDocument8 pages09 InglesJulissa BarciaNo ratings yet
- CATIENNTEditorialRegardingCITROME KERWIN IntJClinPract2006Document2 pagesCATIENNTEditorialRegardingCITROME KERWIN IntJClinPract2006Leslie CitromeNo ratings yet
- SANAD II ValproateDocument12 pagesSANAD II ValproateveerrajuNo ratings yet
- PSY21 COST EFFECTIVENESS ANALYSIS OF EMICIZUMAB FOR THE TREATME - 2019 - Value IDocument1 pagePSY21 COST EFFECTIVENESS ANALYSIS OF EMICIZUMAB FOR THE TREATME - 2019 - Value IMichael John AguilarNo ratings yet
- Comparative Study Between Propofol and Propofol With Ketamine in Ambulatory AnaesthesiaDocument9 pagesComparative Study Between Propofol and Propofol With Ketamine in Ambulatory AnaesthesiaInternational Organization of Scientific Research (IOSR)No ratings yet
- Research Doc DelDocument7 pagesResearch Doc DelrohankishorlandeNo ratings yet
- 12 s2.0 S0048969723019228 MainDocument9 pages12 s2.0 S0048969723019228 MainDarlianaMelloSouzaNo ratings yet
- Comparison of Isotonic and Hypotonic Intravenous Maintenance Fluids A Randomized Clinical TrialDocument8 pagesComparison of Isotonic and Hypotonic Intravenous Maintenance Fluids A Randomized Clinical TrialyunNo ratings yet
- Comparative Efficacy of Anti-Epileptic Drugs For Neonatal Seizures: A Network Meta - AnalysisDocument8 pagesComparative Efficacy of Anti-Epileptic Drugs For Neonatal Seizures: A Network Meta - AnalysisSultan Rahmat SeptianNo ratings yet
- Sepsis and The Systemic Inflammatory Response SyndromeDocument9 pagesSepsis and The Systemic Inflammatory Response SyndromeHandi Tri EffendiNo ratings yet
- Surgery Trans 1 - Systemic Response To InjuryDocument29 pagesSurgery Trans 1 - Systemic Response To InjuryJoan Caacbay De GuzmanNo ratings yet
- TM 15Document8 pagesTM 15Alfi LafitNo ratings yet
- CACCN Study Guide, Final Questions, Answers Oct 2010Document63 pagesCACCN Study Guide, Final Questions, Answers Oct 2010Chris Zantira100% (2)
- Bheesam KumarDocument4 pagesBheesam KumardileepNo ratings yet
- Surgery Crashcourse PDFDocument545 pagesSurgery Crashcourse PDFjlhotaru100% (1)
- Bilirubin Crystals in Neutrophils: A Rare Occurance: January 2018Document5 pagesBilirubin Crystals in Neutrophils: A Rare Occurance: January 2018Djdjjd SiisusNo ratings yet
- MNT For Metabolic StressDocument107 pagesMNT For Metabolic StressBobby SwadharmaNo ratings yet
- University of Santo Tomas: The Graduate SchoolDocument19 pagesUniversity of Santo Tomas: The Graduate SchoolJohn Henry ValenciaNo ratings yet
- QR Management of Neonatal Jaundice (Second Edition)Document8 pagesQR Management of Neonatal Jaundice (Second Edition)نور حسليندا اسحاقNo ratings yet
- Fluido Therapy - Sepsis Jama Zampieri 2023 RV 230010 1686240954.61353Document14 pagesFluido Therapy - Sepsis Jama Zampieri 2023 RV 230010 1686240954.61353VictorMéndezNo ratings yet
- DR Anuj Raj BijukchheDocument95 pagesDR Anuj Raj BijukchheMUHAMMAD JAWAD HASSANNo ratings yet
- Neonatal Sepsis OverviewDocument26 pagesNeonatal Sepsis OverviewDr C JayakumarNo ratings yet
- Pathophysiology: EndometritisDocument8 pagesPathophysiology: EndometritisBrett StevensonNo ratings yet
- Shock SIRS & MODS - Lewis Flashcards - QuizletDocument17 pagesShock SIRS & MODS - Lewis Flashcards - QuizletNursyNurseNo ratings yet
- Sepsis Fact SheetDocument4 pagesSepsis Fact SheetJoana MoreiraNo ratings yet
- CAse Study SEptic ShockDocument29 pagesCAse Study SEptic ShockRyan Inapan67% (3)
- Efficacy and Safety of A Paired Sedation and Ventilator Weaning Prtocol For Mechanically Ventilated Patients in Intesive Care ABC)Document16 pagesEfficacy and Safety of A Paired Sedation and Ventilator Weaning Prtocol For Mechanically Ventilated Patients in Intesive Care ABC)Miguel CachonNo ratings yet
- ISC Workshop - Surgical Nutrition and Fluid and Electrolytes - 2010Document58 pagesISC Workshop - Surgical Nutrition and Fluid and Electrolytes - 2010fiansisNo ratings yet
- Antibiotic Guidelines (2020) - 0Document55 pagesAntibiotic Guidelines (2020) - 0yudhit bessieNo ratings yet
- Neonatal Sepsis: Progress Towards Improved Outcomes: Andi L. Shane, Barbara J. StollDocument9 pagesNeonatal Sepsis: Progress Towards Improved Outcomes: Andi L. Shane, Barbara J. StollMarco Antonio Mendoza OjedaNo ratings yet
- NCLEX: From UworldDocument26 pagesNCLEX: From UworldOlgaKNo ratings yet
- Urosepsis 1Document7 pagesUrosepsis 1Anonymous Xajh4w100% (1)
- PostoperativeDocument21 pagesPostoperativeCitra AyuMerilasariNo ratings yet
- Pathology Solved Papers 2015Document35 pagesPathology Solved Papers 2015Lakshmi Venkataraman100% (3)
- Deep Fungal InfectionDocument39 pagesDeep Fungal InfectionFahmi Nur AL-HidayatNo ratings yet
- Shock and Its Management: Presented byDocument72 pagesShock and Its Management: Presented bysheme171150% (2)
- Thesis Topics For MD Respiratory MedicineDocument7 pagesThesis Topics For MD Respiratory Medicinelindseyriverakansascity100% (2)
- JRRMMC Section of Colon and Rectal Surgery Colorectal Patient's Expectations FormDocument4 pagesJRRMMC Section of Colon and Rectal Surgery Colorectal Patient's Expectations FormJaysonGarabilesEspejoNo ratings yet
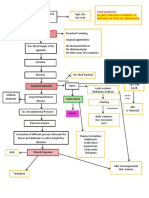
- CPC - Appendicitis (Flowchart)Document1 pageCPC - Appendicitis (Flowchart)Milet NacionalesNo ratings yet
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (23)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (80)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 4 out of 5 stars4/5 (5)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- Sleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningFrom EverandSleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningRating: 4 out of 5 stars4/5 (3)
- Gut: the new and revised Sunday Times bestsellerFrom EverandGut: the new and revised Sunday Times bestsellerRating: 4 out of 5 stars4/5 (392)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDFrom EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDRating: 5 out of 5 stars5/5 (1)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisFrom EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisRating: 3.5 out of 5 stars3.5/5 (2)
- An Autobiography of Trauma: A Healing JourneyFrom EverandAn Autobiography of Trauma: A Healing JourneyRating: 5 out of 5 stars5/5 (2)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Summary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisFrom EverandSummary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (9)
- 12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosFrom Everand12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosRating: 4.5 out of 5 stars4.5/5 (207)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)