You might also like
- An Introduction To Communication (Lynn H. Turner Richard West)Document676 pagesAn Introduction To Communication (Lynn H. Turner Richard West)abubakarsuleiman5206100% (1)
- Disruptive Mood Dysregulation Disorder: Case StudyDocument25 pagesDisruptive Mood Dysregulation Disorder: Case StudyMahnoor Shah100% (1)
- Psychological Assessment Report 1Document16 pagesPsychological Assessment Report 1Kiran Yaqoob MalhotrahNo ratings yet
- Major Depression Case 2Document14 pagesMajor Depression Case 2Mahnoor Malik100% (1)
- Case No 2 SchizoDocument8 pagesCase No 2 SchizoSarah Saqib AhmadNo ratings yet
- Clinical Interviews 2 Chap 4 Part 2Document47 pagesClinical Interviews 2 Chap 4 Part 2Ahmad Farooq100% (1)
- CaseDocument77 pagesCaseGrooming session with IqraNo ratings yet
- Psycho Diagnostic ReportDocument5 pagesPsycho Diagnostic ReportSmridhi Seth100% (1)
- Psychiatry Case Book: U.G.K.M.Udawelagedarda ME/2009/142 Group E Faculty of Medicine University of KelaniyaDocument37 pagesPsychiatry Case Book: U.G.K.M.Udawelagedarda ME/2009/142 Group E Faculty of Medicine University of KelaniyaTilanka WithanaNo ratings yet
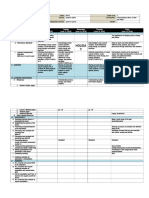
- Daily Lesson Log Ucsp RevisedDocument53 pagesDaily Lesson Log Ucsp RevisedAngelica Orbizo83% (6)
- Case Vignette Assignment 2Document3 pagesCase Vignette Assignment 2mysteryvan1981No ratings yet
- Knowledge Paper XDocument25 pagesKnowledge Paper Xparrot158100% (12)
- Australian Medical Council (Amc) Exam (Brief Overview)Document11 pagesAustralian Medical Council (Amc) Exam (Brief Overview)ahmerNo ratings yet
- A Case Study of A Patient Suffering From Major Depressive DisorderDocument5 pagesA Case Study of A Patient Suffering From Major Depressive Disorderdennis ndegeNo ratings yet
- Profession of The Clinical Psychologist Case 1Document4 pagesProfession of The Clinical Psychologist Case 1Joe SoulageNo ratings yet
- Institutional EconomicsDocument12 pagesInstitutional Economicsicha100% (1)
- Internship ReportDocument16 pagesInternship ReportRACHANA MURALIDHAR 1833279No ratings yet
- 1D Used To and WouldDocument2 pages1D Used To and Wouldlees10088No ratings yet
- English 10 - F2F 6Document5 pagesEnglish 10 - F2F 6Daniela DaculanNo ratings yet
- Chisholm - Problem of The Criterion in Reason and ResponsibilityDocument8 pagesChisholm - Problem of The Criterion in Reason and Responsibilityina823No ratings yet
- Web Quiz 1Document4 pagesWeb Quiz 1nephembaniNo ratings yet
- Hassan Case ReportDocument12 pagesHassan Case ReportkhadijaNo ratings yet
- Clinial Report of A PatientDocument14 pagesClinial Report of A PatientNamra QaisNo ratings yet
- Patient ReportDocument35 pagesPatient Reportshizaarshad125No ratings yet
- 1-History TakingDocument7 pages1-History TakingFUN FLARE SHADOWNo ratings yet
- 3493 Part ADocument7 pages3493 Part ABani Miza NamzaliNo ratings yet
- Lab 5 PsychDocument5 pagesLab 5 PsychMukarla DejavuNo ratings yet
- CounsellingDocument12 pagesCounsellingRida fatimaNo ratings yet
- Case ReportDocument17 pagesCase Reportmirha fatimaNo ratings yet
- Case Profile PsycologyDocument11 pagesCase Profile Psycologycrazy adwaithNo ratings yet
- Case No.7 SchizopherniaDocument18 pagesCase No.7 SchizopherniaAlyna QureshiNo ratings yet
- Psychological DisordersDocument7 pagesPsychological Disorderskuro hanabusaNo ratings yet
- Contentttttt AnalysisDocument10 pagesContentttttt Analysishadiqaasif01No ratings yet
- Case StudyDocument9 pagesCase Studyapsari.mhiNo ratings yet
- .Case 1 SAD - 1695819035000Document13 pages.Case 1 SAD - 1695819035000mabdu4775No ratings yet
- Case No 1:-Bio DataDocument8 pagesCase No 1:-Bio DataSarah Saqib Ahmad100% (1)
- Finl Case 2Document8 pagesFinl Case 2Kainat MumtazNo ratings yet
- Case Summary #1: DepressionDocument7 pagesCase Summary #1: DepressionSam Raven AndresNo ratings yet
- Case Summary #1: DepressionDocument7 pagesCase Summary #1: DepressionSam Raven AndresNo ratings yet
- Case Study 5Document10 pagesCase Study 5josmamani6789No ratings yet
- Ahmed ArshadDocument16 pagesAhmed ArshadBilal PervaizNo ratings yet
- Counsing Report Tasawar 1Document29 pagesCounsing Report Tasawar 1Momal AliNo ratings yet
- Family Medicine FinalDocument90 pagesFamily Medicine FinalPeter MichaelNo ratings yet
- Piyush Saurabh OCDDocument7 pagesPiyush Saurabh OCDhelalNo ratings yet
- Case Studies Ab Psych - BellenDocument20 pagesCase Studies Ab Psych - BellenHobi JungNo ratings yet
- Moolchand Case 01Document15 pagesMoolchand Case 01020Srishti MehtaNo ratings yet
- Case REPORT-2 Bio DataDocument5 pagesCase REPORT-2 Bio Datamariam khan100% (1)
- MRK - Fall 2023 - PSYI619 - 2 - Bc190406911Document11 pagesMRK - Fall 2023 - PSYI619 - 2 - Bc190406911Aniqa waheedNo ratings yet
- Final CaseDocument5 pagesFinal CaseSehar YasmeenNo ratings yet
- Case of Ben Case PreDocument3 pagesCase of Ben Case PreJahziel Anne Dela CruzNo ratings yet
- Abnormal Cases-1Document28 pagesAbnormal Cases-1rimsharajpoot838No ratings yet
- Fiza Case ReportDocument17 pagesFiza Case ReportkhadijaNo ratings yet
- Clinical Psychology R's Case RecordDocument22 pagesClinical Psychology R's Case RecordSwati Tiwari Life CoachNo ratings yet
- HCC Case 2 PresentationDocument25 pagesHCC Case 2 Presentationdamion clarkeNo ratings yet
- Running Head: Family Therapy Session Observation 1Document7 pagesRunning Head: Family Therapy Session Observation 1Hum NjorogeNo ratings yet
- Assignment 4Document5 pagesAssignment 4Mahek DoshiNo ratings yet
- Actual AssignmentDocument5 pagesActual AssignmentAshwin Hemant LawanghareNo ratings yet
- MDD PresentationDocument5 pagesMDD Presentationammaramaryam6463No ratings yet
- Case Summary 1Document75 pagesCase Summary 1Faryad HussainNo ratings yet
- BDI TestDocument5 pagesBDI TestIrsa ZaheerNo ratings yet
- Micah TootDocument2 pagesMicah TootMark Anthony IbayNo ratings yet
- Module 14 AssignmentDocument3 pagesModule 14 AssignmentNicole PoughNo ratings yet
- Social IssuesDocument37 pagesSocial IssuesAnanyaNo ratings yet
- APA Template GoogleDocument57 pagesAPA Template GoogleTanvi ManjrekarNo ratings yet
- Case Report 1Document9 pagesCase Report 1sadiaNo ratings yet
- Rony-Case FinalDocument72 pagesRony-Case FinalTasnim AlomNo ratings yet
- Safeena Persistent DepressiveDocument14 pagesSafeena Persistent DepressiveAlyna QureshiNo ratings yet
- CaseDocument8 pagesCaseKenn Carlo DelaoNo ratings yet
- Taylor Syllabus 2018-2019Document2 pagesTaylor Syllabus 2018-2019api-293370184No ratings yet
- 1 OrCom 155 IntroductionDocument20 pages1 OrCom 155 IntroductionShayne LevisteNo ratings yet
- Philosophy Oct 14Document27 pagesPhilosophy Oct 14Hanna Joy AlaonNo ratings yet
- 91 106 CaslavovaDocument16 pages91 106 Caslavovadavid daviddNo ratings yet
- Rule, N. O., & Ambady, N. (2008) - Brief Exposures Male Sexual Orientation Is Accurately Perceived at 50ms.Document6 pagesRule, N. O., & Ambady, N. (2008) - Brief Exposures Male Sexual Orientation Is Accurately Perceived at 50ms.CharpapathNo ratings yet
- Brave New World Web QuestDocument3 pagesBrave New World Web QuestΑθηνουλα ΑθηναNo ratings yet
- Unit 1Document21 pagesUnit 1rammar147No ratings yet
- Professional/Business Ethics: LT Col (Retd) Khalid Hussain ChohanDocument17 pagesProfessional/Business Ethics: LT Col (Retd) Khalid Hussain ChohanAhmad FarooqNo ratings yet
- CEL2105 Class Material 9 SEM 2-2021-2022Document7 pagesCEL2105 Class Material 9 SEM 2-2021-2022NURUL FAIZAH BINTI ZULKIFLI / UPMNo ratings yet
- Business Communication Group Proposal Group 3: Aroma Resort: Handle The Scandal With Youtuber Khoa PugDocument8 pagesBusiness Communication Group Proposal Group 3: Aroma Resort: Handle The Scandal With Youtuber Khoa PugHằng ThuNo ratings yet
- SF2 LACT 3 Teacher NanDocument5 pagesSF2 LACT 3 Teacher NanLignerrac Anipal UtadNo ratings yet
- Wgu Obc1 Quizzes & Study Questions - Most RecentDocument34 pagesWgu Obc1 Quizzes & Study Questions - Most RecentsdwewNo ratings yet
- P3 Business Analysis 2015 PDFDocument7 pagesP3 Business Analysis 2015 PDFDaniel B Boy NkrumahNo ratings yet
- Critical Reading and ReasoningDocument34 pagesCritical Reading and Reasoningjollibee torresNo ratings yet
- Particularities of The Development of CreativenessDocument4 pagesParticularities of The Development of CreativenessParti BanNo ratings yet
- Mall Atmospherics Interaction EffectsDocument8 pagesMall Atmospherics Interaction EffectsLuis LancaNo ratings yet
- Philippine Studies Araling Pilipino PiliDocument70 pagesPhilippine Studies Araling Pilipino PiliSasha Quinto0% (1)
- Impacto de Influencers en La Decisiónde CompraDocument17 pagesImpacto de Influencers en La Decisiónde CompraYuleisi GonzalesNo ratings yet
- Untamed-Artistry Final JSR Rev2Document15 pagesUntamed-Artistry Final JSR Rev2badjem79No ratings yet
- A3 PPT TemplatesDocument3 pagesA3 PPT TemplatesappleappsNo ratings yet
- Chapter 1: Professional Communication in A Digital, Social, Mobile World 1. Multiple Choices QuestionsDocument4 pagesChapter 1: Professional Communication in A Digital, Social, Mobile World 1. Multiple Choices QuestionsNguyễn Hải BìnhNo ratings yet