You might also like
- Acid-Base and Electrolyte Handbook for Veterinary TechniciansFrom EverandAcid-Base and Electrolyte Handbook for Veterinary TechniciansAngela Randels-ThorpNo ratings yet
- Water Follows Sodium (Via OsmoticDocument3 pagesWater Follows Sodium (Via OsmoticMark Vincent SahagunNo ratings yet
- Electrolytes LecDocument4 pagesElectrolytes LecMichelle San Miguel FeguroNo ratings yet
- Wk8 - Electrolyte Imbalances & Acid-Base ImbalancesDocument65 pagesWk8 - Electrolyte Imbalances & Acid-Base ImbalancesPotato PceeNo ratings yet
- Clinical Chemistry 2 LAB MT305 Rlh3: ElectrolytesDocument2 pagesClinical Chemistry 2 LAB MT305 Rlh3: ElectrolytesEmiaj Francinne Mendoza100% (1)
- Perioperative Care Acid Base ElectrolytesDocument7 pagesPerioperative Care Acid Base ElectrolytesIlyas HarunNo ratings yet
- Electrolytes Water Balance PH Balance Trace MetalsDocument21 pagesElectrolytes Water Balance PH Balance Trace MetalsJohn Kevin Carl SaligumbaNo ratings yet
- ELECTROLYTES Clinica SignificanceDocument6 pagesELECTROLYTES Clinica SignificanceKim Mae ComendadorNo ratings yet
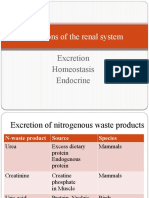
- Functions of The Renal SystemDocument30 pagesFunctions of The Renal SystemBlessing ChirwaNo ratings yet
- Hypokalemia 2Document32 pagesHypokalemia 2aqilasafikaNo ratings yet
- Electrolyte Imbalance Cause Signs and Symptoms Intervention ConnectionDocument6 pagesElectrolyte Imbalance Cause Signs and Symptoms Intervention ConnectionmkninnyNo ratings yet
- Week12 13 RENAL PhysiologyDocument41 pagesWeek12 13 RENAL Physiologyirwan kastellaNo ratings yet
- Hyponatremia: ElectrolytesDocument5 pagesHyponatremia: ElectrolytesCyreen Jill Aliling100% (1)
- WEEK 5 Management of Patients With Fluids and ElectrolytesDocument89 pagesWEEK 5 Management of Patients With Fluids and ElectrolytesErica P. ManlunasNo ratings yet
- Potassium Disorders: Syeda Shaheera ZaidiDocument60 pagesPotassium Disorders: Syeda Shaheera ZaidiMohammad AliNo ratings yet
- Composition of Fluid & ElectrolytesDocument33 pagesComposition of Fluid & ElectrolytesDwi SiregarNo ratings yet
- Kuliah Mineral 2015-2016Document20 pagesKuliah Mineral 2015-2016molenNo ratings yet
- Salty-Testing Skin, Chronic Respiratory Problems, Lung Infections, Poor Growth/weight Loss, Meconium IleusDocument8 pagesSalty-Testing Skin, Chronic Respiratory Problems, Lung Infections, Poor Growth/weight Loss, Meconium IleusOrhan AsdfghjklNo ratings yet
- Mark Billy L. Perpetua, Man RN: Fluids, Electrolytes andDocument96 pagesMark Billy L. Perpetua, Man RN: Fluids, Electrolytes andMaica LectanaNo ratings yet
- Diuretics MOA Notes Indications Side Effects DrugsDocument1 pageDiuretics MOA Notes Indications Side Effects Drugsmonica leeNo ratings yet
- Fluids and Renal DisorderDocument139 pagesFluids and Renal DisorderLhara MañoNo ratings yet
- Electrolyte: Sodium: Jai Anthony F. Cuevas, RMTDocument39 pagesElectrolyte: Sodium: Jai Anthony F. Cuevas, RMTBeaNo ratings yet
- Hypokalemia 180813073624Document26 pagesHypokalemia 180813073624korotkofNo ratings yet
- Fluids and Electrolytes (Concentration and Composition Changes)Document6 pagesFluids and Electrolytes (Concentration and Composition Changes)Kristin SaberonNo ratings yet
- Kid and 2 CatsDocument33 pagesKid and 2 Catsastrid shabrinaNo ratings yet
- ElectrolytesDocument60 pagesElectrolytesnmukila2No ratings yet
- Fe Finals NotesDocument23 pagesFe Finals NoteshanhananicasNo ratings yet
- Renal Physiology ReviewDocument7 pagesRenal Physiology ReviewHOD AnesthesiaNo ratings yet
- Fluid PDFDocument93 pagesFluid PDFSandeep VermaNo ratings yet
- Fluid & ElectrolyteDocument69 pagesFluid & ElectrolytePaul Ebenezer100% (1)
- Fluid and Electrolyte Balance in ICUDocument46 pagesFluid and Electrolyte Balance in ICUtapas_kbNo ratings yet
- Nursing 75 Fluid and Electrolyte Exam 2Document6 pagesNursing 75 Fluid and Electrolyte Exam 2chubbygunny_29776413No ratings yet
- K (Anion Gap 12) (Anion Gap 12) Acute Asthma Hypovolemia: - Vomit - Pyloric StenosisDocument4 pagesK (Anion Gap 12) (Anion Gap 12) Acute Asthma Hypovolemia: - Vomit - Pyloric StenosisAhmad Asyraf AzmanNo ratings yet
- Fluid & Electrolytes: DR Win Min OoDocument55 pagesFluid & Electrolytes: DR Win Min OoBiomedical Science MyanmarNo ratings yet
- RenalElectrolytecharts 220906 101323 2Document7 pagesRenalElectrolytecharts 220906 101323 2Saheed jaladeNo ratings yet
- W2 PHARMACOLOGY OF DIURETICS Short Notes 2017Document6 pagesW2 PHARMACOLOGY OF DIURETICS Short Notes 2017Syximsh FPNo ratings yet
- Aldosterone Regulation of Sodium: Atrial Natriuretic Peptide ANPDocument4 pagesAldosterone Regulation of Sodium: Atrial Natriuretic Peptide ANPHanoof GhaziNo ratings yet
- Felixcharlie Electrolyte Homeostasis Part 3Document3 pagesFelixcharlie Electrolyte Homeostasis Part 3Nur Fatima SanaaniNo ratings yet
- Electrolyte 1Document8 pagesElectrolyte 1Ylooner QuitsNo ratings yet
- Physiology 1 Fluid ElectrolyteDocument38 pagesPhysiology 1 Fluid ElectrolyteHaziq KamardinNo ratings yet
- ELECTROLYTES (Na & K)Document3 pagesELECTROLYTES (Na & K)Alondra SagarioNo ratings yet
- Water BalanceDocument9 pagesWater BalanceKim Mae ComendadorNo ratings yet
- Fluids and Electrolytes, Acid-Base ImbalancesDocument15 pagesFluids and Electrolytes, Acid-Base ImbalancesJherome FernandoNo ratings yet
- Renal Acute Kidney InjuryDocument41 pagesRenal Acute Kidney InjuryTim SilvaNo ratings yet
- Dr. Hendrata - CLINICAL POTASSIUM IMBALANCE (Slide PERNEFRI Jakarta (24-27 Nop 2011)Document45 pagesDr. Hendrata - CLINICAL POTASSIUM IMBALANCE (Slide PERNEFRI Jakarta (24-27 Nop 2011)Patricia WenNo ratings yet
- PATH ImmuneDocument7 pagesPATH ImmuneDavid DvoskineNo ratings yet
- Electrolytedisturbances 111102083753 Phpapp02Document137 pagesElectrolytedisturbances 111102083753 Phpapp02bobbyfildianNo ratings yet
- Chronic Renal Failure 2Document66 pagesChronic Renal Failure 2Octaviani ElparesiNo ratings yet
- Electrolytes PDFDocument5 pagesElectrolytes PDFFrances FranciscoNo ratings yet
- Electrolyte Imbalance - Handout PDFDocument23 pagesElectrolyte Imbalance - Handout PDFFaisal Ridho SaktiNo ratings yet
- PotassiumDocument2 pagesPotassiumtuffie85No ratings yet
- CC Lec Mod 3Document13 pagesCC Lec Mod 38wgmhh9ks9No ratings yet
- Hypokalemia CausesDocument12 pagesHypokalemia CausesEsther RefuncionNo ratings yet
- Assignment#1Document13 pagesAssignment#1Mark Jefferson LunaNo ratings yet
- Disturbances of Fluid and Electrolyte BalanceDocument3 pagesDisturbances of Fluid and Electrolyte BalanceJezel B. AnadonNo ratings yet
- 3.3 KidneyDocument54 pages3.3 KidneySurvin KandhariNo ratings yet
- Supplementary Information To Chapter 30: Overview of Electrolyte BalanceDocument11 pagesSupplementary Information To Chapter 30: Overview of Electrolyte BalanceAaron JoseNo ratings yet
- Serum Electrolytes-Part 1Document22 pagesSerum Electrolytes-Part 1Marwa 2002No ratings yet
- Lecture 22 - Fluid & Electrolyte Balance2 - 21 Oct 2006Document28 pagesLecture 22 - Fluid & Electrolyte Balance2 - 21 Oct 2006api-3703352No ratings yet
- Chapter 15: ElectrolytesDocument6 pagesChapter 15: ElectrolytesTelle AngNo ratings yet
- The Brain Adapts To Dishonesty: Neil Garrett, Stephanie C Lazzaro, Dan Ariely & Tali SharotDocument9 pagesThe Brain Adapts To Dishonesty: Neil Garrett, Stephanie C Lazzaro, Dan Ariely & Tali SharotVissente TapiaNo ratings yet
- DR Lal Pathlabs: LPL - Lpl-Rohini (National Reference Lab) Sector - 18, Block - E Rohini Delhi 110085Document1 pageDR Lal Pathlabs: LPL - Lpl-Rohini (National Reference Lab) Sector - 18, Block - E Rohini Delhi 110085Sandeep ArelaNo ratings yet
- Ornamental Breeding ConceptsDocument83 pagesOrnamental Breeding ConceptsjoshigautaNo ratings yet
- Oscar PDFDocument1 pageOscar PDFAkaYumi GNo ratings yet
- Use of Dinitrosalicylic Acid Reagent For Determination of Reducing SugarDocument7 pagesUse of Dinitrosalicylic Acid Reagent For Determination of Reducing SugarLANANo ratings yet
- Kajtez NatCommun 2016Document11 pagesKajtez NatCommun 2016Luka JandricNo ratings yet
- LettersDocument5 pagesLettersCarolina Rodriguez GuarinNo ratings yet
- 17 3Document30 pages17 3Lim ZjianNo ratings yet
- Neuro Informo1Document8 pagesNeuro Informo1Dr. Kaushal Kishor SharmaNo ratings yet
- Introduction To Environmental EngineeringDocument11 pagesIntroduction To Environmental EngineeringJeric WaldoNo ratings yet
- GDR - Poc Update (01.07.21)Document2 pagesGDR - Poc Update (01.07.21)Dr ThietNo ratings yet
- Jurnal EvolusiDocument19 pagesJurnal EvolusiAdicahyoo SentosaNo ratings yet
- Shimelis WondimuDocument95 pagesShimelis WondimuMelaku MamayeNo ratings yet
- Blood Physiology 2022Document116 pagesBlood Physiology 2022Gurmessa FekaduNo ratings yet
- Cosmetics PresentationDocument7 pagesCosmetics PresentationOkafor AugustineNo ratings yet
- Detailed Lesson Plan in ScienceDocument8 pagesDetailed Lesson Plan in ScienceRegine MalanaNo ratings yet
- Anexo Norma HolandesaDocument13 pagesAnexo Norma HolandesaThePomboNo ratings yet
- Magnotti Et Al 2016 Cryopreservation and Vitrificaction of Fish SemenDocument11 pagesMagnotti Et Al 2016 Cryopreservation and Vitrificaction of Fish SemenssotomNo ratings yet
- 12 Biology Notes Ch11 Biotechnology Principles and ProcessesDocument9 pages12 Biology Notes Ch11 Biotechnology Principles and ProcessesAnkit YadavNo ratings yet
- Unit 5, Novel Drug Delivery Systems, B Pharmacy 7th Sem, Carewell PharmaDocument30 pagesUnit 5, Novel Drug Delivery Systems, B Pharmacy 7th Sem, Carewell Pharma47 DevendraNo ratings yet
- Physiology Notes 1Document193 pagesPhysiology Notes 1Sivaranjini BhalaNo ratings yet
- Inheritance 14.2Document6 pagesInheritance 14.2YashodhaNo ratings yet
- Top 50 Biotech CompaniesDocument3 pagesTop 50 Biotech CompaniesVidya SagarNo ratings yet
- Field Trip ReportDocument28 pagesField Trip ReportTootsie100% (1)
- Chapter 44 Activity and ExerciseDocument7 pagesChapter 44 Activity and ExerciseKathleen FrugalidadNo ratings yet
- Banana Expert System - Crop ProtectionDocument38 pagesBanana Expert System - Crop ProtectionbhushanNo ratings yet
- 2016 Black Soldier Fly WartazoaDocument11 pages2016 Black Soldier Fly WartazoaghotamaNo ratings yet
- Current Concepts On How To Optimise Skin Needling 2020 2Document6 pagesCurrent Concepts On How To Optimise Skin Needling 2020 2maat1No ratings yet
- Investigatory Project in Science ViDocument21 pagesInvestigatory Project in Science Vijasperrheyhuera100% (2)
- CloveDocument53 pagesCloveDharun RanganathanNo ratings yet