You might also like
- Atropine Refractoriness in OP and Carbamate PoisoningDocument18 pagesAtropine Refractoriness in OP and Carbamate PoisoningDouglas SantosNo ratings yet
- Less Is More: Catecholamine-Sparing Strategies in Septic ShockDocument3 pagesLess Is More: Catecholamine-Sparing Strategies in Septic Shockmariano villavicencioNo ratings yet
- 949-Texto Del Artículo-7086-1-10-20231207Document8 pages949-Texto Del Artículo-7086-1-10-20231207mplp2721No ratings yet
- ACTH Treatment For Management of Nephrotic SyndromeDocument16 pagesACTH Treatment For Management of Nephrotic SyndromeCalvin Tanuwijaya Stick BolaNo ratings yet
- Intoxicacion Por Betabloqueadores ToxicologyDocument42 pagesIntoxicacion Por Betabloqueadores ToxicologyIza ÁlvarezNo ratings yet
- Articles: Spironolactone Management of Resistant HypertensionDocument8 pagesArticles: Spironolactone Management of Resistant HypertensionKatherine America Camac DelgadoNo ratings yet
- Corticosteroid After Etomidate in Critically IllDocument41 pagesCorticosteroid After Etomidate in Critically IllanaeshklNo ratings yet
- CaptoprilDocument5 pagesCaptoprilmooncake sanchezNo ratings yet
- Antiepileptic Drugs Montherapy and Hematolgic, Japin 2019Document13 pagesAntiepileptic Drugs Montherapy and Hematolgic, Japin 2019Mohammed Abdullah AlqaadNo ratings yet
- Besok HuluqDocument7 pagesBesok Huluqagustiawan28No ratings yet
- Comparative Bioavailability Study of Phenytoin inDocument4 pagesComparative Bioavailability Study of Phenytoin inHuydiNo ratings yet
- Treatment of Adults With Idiopathic Recurrent Pericarditis Novel Use of ImmunotherapyDocument15 pagesTreatment of Adults With Idiopathic Recurrent Pericarditis Novel Use of Immunotherapytere serranoNo ratings yet
- Testing For Primary Hyperaldosteronism and MRA TX Annals 2020Document10 pagesTesting For Primary Hyperaldosteronism and MRA TX Annals 2020Miri PravdaNo ratings yet
- Goz 043Document8 pagesGoz 043nNo ratings yet
- Journal Club CompleteDocument2 pagesJournal Club Completeapi-534233456No ratings yet
- Patisiran Pharmacokinetics, Pharmacodynamics, and Exposure-Response Analyses in the Phase 3 APOLLO Trial in Patients With Hereditary Transthyretin-Mediated (hATTR) AmyloidosisDocument13 pagesPatisiran Pharmacokinetics, Pharmacodynamics, and Exposure-Response Analyses in the Phase 3 APOLLO Trial in Patients With Hereditary Transthyretin-Mediated (hATTR) AmyloidosisMihaela BerindeieNo ratings yet
- Articulo 6 FarmacoDocument8 pagesArticulo 6 FarmacoLiz Espinoza ZambranoNo ratings yet
- Profile of Aluminum Phosphide Poisoning in A Tertiary Care Institute in The Sub-Himalayan RegionDocument6 pagesProfile of Aluminum Phosphide Poisoning in A Tertiary Care Institute in The Sub-Himalayan RegionAccio JournalNo ratings yet
- Bivalirudin Anticoagulant1Document6 pagesBivalirudin Anticoagulant1walid hassanNo ratings yet
- 1 s2.0 S0168827820304700 MainDocument11 pages1 s2.0 S0168827820304700 MainHadi KuriryNo ratings yet
- Individualized Pharmacokinetic Monitoring Reduces Aminoglycoside-Associated Nephrotoxicity and CostsDocument9 pagesIndividualized Pharmacokinetic Monitoring Reduces Aminoglycoside-Associated Nephrotoxicity and CostsDaniela HernandezNo ratings yet
- Assessment of Synthetic Glucocorticoids in Asthmatic SputumDocument3 pagesAssessment of Synthetic Glucocorticoids in Asthmatic SputumDewiRahmatikaNo ratings yet
- Amlodipine AtenololDocument7 pagesAmlodipine AtenololBidhur Chakma 1935371673No ratings yet
- Ritscher 2019Document10 pagesRitscher 2019maxsmaxNo ratings yet
- Carditone Herb Clinical StudyDocument8 pagesCarditone Herb Clinical StudyDr Sreedhar TirunagariNo ratings yet
- 12 - 2015 - LT Safety and Efficacy of Imatinib in PAH - IMPRES (10) 70Document10 pages12 - 2015 - LT Safety and Efficacy of Imatinib in PAH - IMPRES (10) 70edward the iiiNo ratings yet
- Serum Electrolyte Levels and Outcomes in Patients Hospitalized With Hepatic EncephalopathyDocument7 pagesSerum Electrolyte Levels and Outcomes in Patients Hospitalized With Hepatic EncephalopathyhimayatullahNo ratings yet
- Zawierucha Et Al-2019-Frontiers in EndocrinologyDocument8 pagesZawierucha Et Al-2019-Frontiers in Endocrinologygodato SynclaneNo ratings yet
- 10 1097MD 0000000000000587Document3 pages10 1097MD 0000000000000587abbasamiri135103No ratings yet
- 1 PBDocument12 pages1 PBwinda kiranaNo ratings yet
- 1 PBDocument11 pages1 PBrahmat khairulNo ratings yet
- Outcome of Treatment of OPC Poisoning Patients With Atropine or Atropine Plus PralidoximeDocument5 pagesOutcome of Treatment of OPC Poisoning Patients With Atropine or Atropine Plus Pralidoximeshaker al baharNo ratings yet
- PGI Score A Simplified Three-Point Prognostic Score ForDocument4 pagesPGI Score A Simplified Three-Point Prognostic Score ForWalaa YousefNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 8: UrologyFrom EverandComplementary and Alternative Medical Lab Testing Part 8: UrologyRating: 3 out of 5 stars3/5 (1)
- B6 For AkathisiaDocument6 pagesB6 For AkathisiaPsikiatri 76 UndipNo ratings yet
- Aldosterone To Renin Ratio As Screening Tool in Primary AldosteronismDocument9 pagesAldosterone To Renin Ratio As Screening Tool in Primary AldosteronismghfkhgfjhfgNo ratings yet
- Inappropriate Usage of Intravenous Proton Pump Inhibitors and Associated Factors in a High Complexity Hospital in BrazilDocument7 pagesInappropriate Usage of Intravenous Proton Pump Inhibitors and Associated Factors in a High Complexity Hospital in BrazilJosivaneMarquesNo ratings yet
- E2 Journal of Hypertension Vol 35, E-Supplement 3, November 2017Document1 pageE2 Journal of Hypertension Vol 35, E-Supplement 3, November 2017Sadam_fasterNo ratings yet
- 52 Iajps52042018 PDFDocument11 pages52 Iajps52042018 PDFBaru Chandrasekhar RaoNo ratings yet
- Impact of A Novel Strategy For Critical ValuesDocument9 pagesImpact of A Novel Strategy For Critical ValuesMD LarasatiNo ratings yet
- Elaxim ResearchDocument6 pagesElaxim ResearchMayukh BanerjeeNo ratings yet
- Uji Klinis 5Document10 pagesUji Klinis 5Verliatesya TugasNo ratings yet
- Standardized Laboratory Monitoring With Use of Isotretinoin in Acne - Hansen2016Document6 pagesStandardized Laboratory Monitoring With Use of Isotretinoin in Acne - Hansen2016Blu Punto ArtNo ratings yet
- X 1504300210Document7 pagesX 1504300210OleOhhNo ratings yet
- Mannitol Vs Hypertonic SalineDocument8 pagesMannitol Vs Hypertonic SalineaizenfazerNo ratings yet
- Op 2b 05 Effect of Health Education Intervention.48Document1 pageOp 2b 05 Effect of Health Education Intervention.48omingNo ratings yet
- Metoprolol vs. Diltiazem in The Acute Management of Atrial Fibrillation in Patients With Heart Failure With Reduced Ejection FractionDocument5 pagesMetoprolol vs. Diltiazem in The Acute Management of Atrial Fibrillation in Patients With Heart Failure With Reduced Ejection FractionGenevieve LawrenceNo ratings yet
- Perspectives in Clinical Hepatology Current and Novel Immunosuppressive Therapy For Autoimmune HepatitisDocument7 pagesPerspectives in Clinical Hepatology Current and Novel Immunosuppressive Therapy For Autoimmune HepatitisPathrecia Natalia SiagianNo ratings yet
- 9Document12 pages9gpatwallahNo ratings yet
- Adverse Drug Reaction Monitoring With Angiotensin Converting Enzyme Inhibitors: A Prospective, Randomized, Open-Label, Comparative StudyDocument6 pagesAdverse Drug Reaction Monitoring With Angiotensin Converting Enzyme Inhibitors: A Prospective, Randomized, Open-Label, Comparative Studybbaam99No ratings yet
- HindawiDocument6 pagesHindawiTaufiqo Nugraha SjachrilNo ratings yet
- Arp2018 1486261Document5 pagesArp2018 1486261Sheren ElinNo ratings yet
- Jurnal Terapi ACE Inhibitors in Anthracycline Induced CardiotoxicityDocument6 pagesJurnal Terapi ACE Inhibitors in Anthracycline Induced CardiotoxicityalerohmadNo ratings yet
- Aptt 1Document21 pagesAptt 1Diantari PrawertiNo ratings yet
- Astronaut 2013Document11 pagesAstronaut 2013Guilherme CarelliNo ratings yet
- Hypoalbuminemia 2018Document6 pagesHypoalbuminemia 2018Tayyaba RahatNo ratings yet
- Methylprednisolone in West SyndromeDocument5 pagesMethylprednisolone in West SyndromeBandya SahooNo ratings yet
- Toxics: Pattern of Paracetamol Poisoning: Influence On Outcome and ComplicationsDocument11 pagesToxics: Pattern of Paracetamol Poisoning: Influence On Outcome and Complicationsinfinity ooNo ratings yet
- Use of Very-High-Dose Olanzapine in Treatment-Resistant SchizophreniaDocument4 pagesUse of Very-High-Dose Olanzapine in Treatment-Resistant SchizophreniaPutu Agus GrantikaNo ratings yet
- Farmacology Del Paro CardiacoDocument14 pagesFarmacology Del Paro CardiacoNicoSwtifNo ratings yet
- 2iccas2005 Paper 377Document5 pages2iccas2005 Paper 377Cristian BandilaNo ratings yet
- Sunera Best Practices For Remediating SoDsDocument7 pagesSunera Best Practices For Remediating SoDssura anil reddyNo ratings yet
- 0520 Int OTG P4 MSDocument12 pages0520 Int OTG P4 MSTrévina JosephNo ratings yet
- AlternatorDocument3 pagesAlternatorVatsal PatelNo ratings yet
- Tiresocks CatalogDocument19 pagesTiresocks CatalogAshBossNo ratings yet
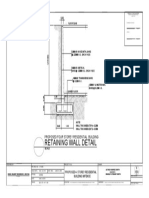
- Retaining Wall DetailsDocument1 pageRetaining Wall DetailsWilbert ReuyanNo ratings yet
- Manual PDFDocument9 pagesManual PDFRuth ResuelloNo ratings yet
- Red Lion Edict-97 - Manual PDFDocument282 pagesRed Lion Edict-97 - Manual PDFnaminalatrukNo ratings yet
- Atlas Ci30002Tier-PropanDocument3 pagesAtlas Ci30002Tier-PropanMarkus JeremiaNo ratings yet
- 4) April 2023 Current AffairsDocument24 pages4) April 2023 Current AffairsPicturesque vibrant shadesNo ratings yet
- Forecast Time Series-NotesDocument138 pagesForecast Time Series-NotesflorinNo ratings yet
- Xt600e 3tb-3uw 90-95Document46 pagesXt600e 3tb-3uw 90-95Kenneth SynnesNo ratings yet
- Olt CliDocument2 pagesOlt CliMohammad SaeedNo ratings yet
- An Introduction To Log ShootingDocument10 pagesAn Introduction To Log ShootingSorin GociuNo ratings yet
- bk978 1 6817 4068 3ch1Document28 pagesbk978 1 6817 4068 3ch1fysmaNo ratings yet
- Heather Bianco 2016 Resume Revised PDFDocument3 pagesHeather Bianco 2016 Resume Revised PDFapi-316610725No ratings yet
- Nelson Climate Change Plan UpdateDocument37 pagesNelson Climate Change Plan UpdateBillMetcalfeNo ratings yet
- Construction Materials and Testing: "WOOD"Document31 pagesConstruction Materials and Testing: "WOOD"Aira Joy AnyayahanNo ratings yet
- A Primer On Financial Time Series AnalysisDocument93 pagesA Primer On Financial Time Series AnalysisKM AgritechNo ratings yet
- DWDM Route Planning A4 WPDocument3 pagesDWDM Route Planning A4 WPChavara MatekweNo ratings yet
- CAFA Open House HighlightsDocument1 pageCAFA Open House HighlightsDaniel LaiNo ratings yet
- Design and Analysis of Buck ConverterDocument18 pagesDesign and Analysis of Buck Converterk rajendraNo ratings yet
- Fisher - Techincal Monograph 42 - Understanding DecibelsDocument8 pagesFisher - Techincal Monograph 42 - Understanding Decibelsleslie.lp2003No ratings yet
- Is Iso 2692-1992Document24 pagesIs Iso 2692-1992mwasicNo ratings yet
- Natural GasDocument86 pagesNatural GasNikhil TiwariNo ratings yet
- Science MELCsDocument42 pagesScience MELCsRanjell Allain TorresNo ratings yet
- HNM Announcement Flyer enDocument2 pagesHNM Announcement Flyer enJali SahiminNo ratings yet
- Tugas Bahasa Inggris Analytical Exposition Text: Disusun Oleh: Nama:Hansel Hendrawan Effendy Kelas:XI IPA 1Document4 pagesTugas Bahasa Inggris Analytical Exposition Text: Disusun Oleh: Nama:Hansel Hendrawan Effendy Kelas:XI IPA 1Hansel HendrawanNo ratings yet
- 2 Integrated MarketingDocument13 pages2 Integrated MarketingPaula Marin CrespoNo ratings yet
- Coffee TestDocument6 pagesCoffee TestAmit Satyen RaviNo ratings yet