You might also like
- LeukemiaDocument29 pagesLeukemiaMichelle TeodoroNo ratings yet
- Malaria Microscopy WHO PDFDocument140 pagesMalaria Microscopy WHO PDFsarasNo ratings yet
- PitocinDocument5 pagesPitocinWilliam BrownNo ratings yet
- Burlinson-2018-Sepsis in Pregnancy and The Puerperium PDFDocument12 pagesBurlinson-2018-Sepsis in Pregnancy and The Puerperium PDFntnquynhproNo ratings yet
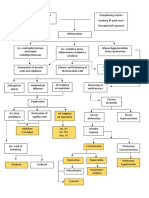
- Copd PathoDocument1 pageCopd PathoRey AngeloNo ratings yet
- Maternal Sepsis and Sepsis ShockDocument17 pagesMaternal Sepsis and Sepsis ShockAlvaro Andres Flores JimenezNo ratings yet
- BJAEd - Hemorragia Obstetrica 2022Document7 pagesBJAEd - Hemorragia Obstetrica 2022Dragos IonixNo ratings yet
- Nejmra 1513247Document11 pagesNejmra 1513247Jose BoderoNo ratings yet
- Medical and Obstetric Outcomes Among Preg Wpman With Cpngenital Hart DseeeDocument9 pagesMedical and Obstetric Outcomes Among Preg Wpman With Cpngenital Hart DseeeZahed UllahNo ratings yet
- Medicina 59 01151Document9 pagesMedicina 59 01151Lissaberti AmaliahNo ratings yet
- JCM 12 06175Document10 pagesJCM 12 06175Taulant MukaNo ratings yet
- Nejmra 1513247Document11 pagesNejmra 1513247Franz Huber QueiroloNo ratings yet
- Postpartum HemorrhageDocument22 pagesPostpartum HemorrhageReynaldiReikyHadiwijayaNo ratings yet
- Interrelation of Liver & Kidney Parameter Changes Association With Hematological Changes of Patients With Dengue FeverDocument6 pagesInterrelation of Liver & Kidney Parameter Changes Association With Hematological Changes of Patients With Dengue FeverSALT Journal of Scientific Research in HealthcareNo ratings yet
- Risk Factor For Sever Postpartum Hemorrhage A Case Control StudyDocument9 pagesRisk Factor For Sever Postpartum Hemorrhage A Case Control StudyAhmad SyaukatNo ratings yet
- HPP 2022Document25 pagesHPP 2022rafael martinezNo ratings yet
- Hemorragia y EmbrazoDocument6 pagesHemorragia y Embrazoana catalinaNo ratings yet
- Hipertension in PregnancyDocument8 pagesHipertension in PregnancyblaeagNo ratings yet
- Abruptio PlacentaeDocument5 pagesAbruptio PlacentaeindahNo ratings yet
- Management of HypertensionDocument6 pagesManagement of HypertensionRioNo ratings yet
- Hemorrgia Obstetrica 2020Document20 pagesHemorrgia Obstetrica 2020Carolina VargasNo ratings yet
- Critically Ill Obstetric Patients and Feto-Maternal Outcome: EditorialDocument3 pagesCritically Ill Obstetric Patients and Feto-Maternal Outcome: EditorialMahtosurup GodavarthyNo ratings yet
- Severe Postpartum Hemorrhage From Uterine AtonyDocument6 pagesSevere Postpartum Hemorrhage From Uterine AtonyYuang Anaya VargasNo ratings yet
- Clinical Study: Severe Postpartum Hemorrhage From Uterine Atony: A Multicentric StudyDocument7 pagesClinical Study: Severe Postpartum Hemorrhage From Uterine Atony: A Multicentric StudymelisaberlianNo ratings yet
- Strokeinpregnancy: An UpdateDocument18 pagesStrokeinpregnancy: An UpdateFerina Mega SilviaNo ratings yet
- Effect of Maternal Body Mass Index On Postpartum HemorrhageDocument10 pagesEffect of Maternal Body Mass Index On Postpartum Hemorrhagegopal trustNo ratings yet
- Postpartum Hemorrhage: New Insights For Definition and DiagnosisDocument8 pagesPostpartum Hemorrhage: New Insights For Definition and DiagnosisMarkoNo ratings yet
- The Role of Fibrinogen in Postpartu - 2022 - Best Practice - Research Clinical ADocument12 pagesThe Role of Fibrinogen in Postpartu - 2022 - Best Practice - Research Clinical APaulHerreraNo ratings yet
- Medip, IJRCOG-7407 ODocument6 pagesMedip, IJRCOG-7407 OKomalNo ratings yet
- Acute Pyelonephritis in Pregnancy: An 18-Year Retrospective AnalysisDocument6 pagesAcute Pyelonephritis in Pregnancy: An 18-Year Retrospective AnalysisIntan Wahyu CahyaniNo ratings yet
- Postpartum Hemorrhage: New Insights For Definition and DiagnosisDocument7 pagesPostpartum Hemorrhage: New Insights For Definition and DiagnosisRabbi'ahNo ratings yet
- Vanderpol 2016Document6 pagesVanderpol 2016Andy esNo ratings yet
- Postpartum Hemorrhage, Update 2016Document31 pagesPostpartum Hemorrhage, Update 2016Marthin Fernandes PasaribuNo ratings yet
- Management of Severe Hypertension in PregnancyDocument7 pagesManagement of Severe Hypertension in PregnancyAnastasia RiuneszveNo ratings yet
- VHRM 19 469 - 114322Document16 pagesVHRM 19 469 - 114322Hayfa LayebNo ratings yet
- Ner Enberg 2017Document7 pagesNer Enberg 2017Ruben Dario Choque CutipaNo ratings yet
- PPH Introduction 1Document95 pagesPPH Introduction 1regine maeNo ratings yet
- Famacion - Journal Article (Red Alert II An Update On Postpartum Hemorrhage)Document6 pagesFamacion - Journal Article (Red Alert II An Update On Postpartum Hemorrhage)Kyra Bianca R. FamacionNo ratings yet
- Meconium-Stained Amniotic Fluid: A Risk Factor For Postpartum HemorrhageDocument5 pagesMeconium-Stained Amniotic Fluid: A Risk Factor For Postpartum HemorrhagelaniNo ratings yet
- BR J Haematol - 2014 - Oteng Ntim - Pregnancy Outcome in Patients With Sickle Cell Disease in The UK A National CohortDocument9 pagesBR J Haematol - 2014 - Oteng Ntim - Pregnancy Outcome in Patients With Sickle Cell Disease in The UK A National CohortJustine ObedNo ratings yet
- Risk Factors For Severe Postpartum Haemorrhage During Caesarean Section For Placenta PraeviaDocument7 pagesRisk Factors For Severe Postpartum Haemorrhage During Caesarean Section For Placenta PraeviaCorina PavalacheNo ratings yet
- Criterios de HPPDocument7 pagesCriterios de HPPLisseth Becerra VargasNo ratings yet
- Endoscopic Intervention and Cholecystectomy in Pregnant Women With Acute Biliary Pancreatitis Decreases Early ReadmissionsDocument19 pagesEndoscopic Intervention and Cholecystectomy in Pregnant Women With Acute Biliary Pancreatitis Decreases Early ReadmissionsCarlos Altez FernandezNo ratings yet
- New Et Al-2016-British Journal of HaematologyDocument45 pagesNew Et Al-2016-British Journal of HaematologyClara Bordes GarcíaNo ratings yet
- Abnormaluterinebleeding Inyoungwomenwithblood Disorders: Kathryn E. Dickerson,, Neethu M. Menon,, Ayesha ZiaDocument18 pagesAbnormaluterinebleeding Inyoungwomenwithblood Disorders: Kathryn E. Dickerson,, Neethu M. Menon,, Ayesha ZiaSalvador ArredondoNo ratings yet
- Verma 2009Document15 pagesVerma 2009Zorobabel AzondogaNo ratings yet
- Evaluation During Postpartum HemorrhageDocument10 pagesEvaluation During Postpartum HemorrhageNilfacio PradoNo ratings yet
- HPP Pengaruh Pada HBDocument6 pagesHPP Pengaruh Pada HBchanyundaNo ratings yet
- Aplastic Anemia During Pregnancy: A Review of Obstetric and Anesthetic ConsiderationsDocument9 pagesAplastic Anemia During Pregnancy: A Review of Obstetric and Anesthetic Considerationsalston96No ratings yet
- Jsafog 13 137Document5 pagesJsafog 13 137Elizabeth Duprat GaxiolaNo ratings yet
- Antepartum HaemorrhageDocument23 pagesAntepartum HaemorrhageSutanti Lara DewiNo ratings yet
- Prevalence of Obstetric Haemorrhage On A Teaching HospitalDocument7 pagesPrevalence of Obstetric Haemorrhage On A Teaching Hospitalodunze augustusNo ratings yet
- Venous Thromboembolism in Pregnancy Challenges and SolutionsDocument17 pagesVenous Thromboembolism in Pregnancy Challenges and Solutionsjeanx666No ratings yet
- Dines 2020 ACKD Hypertensive Disorders of PregnancyDocument9 pagesDines 2020 ACKD Hypertensive Disorders of PregnancyBCR ABLNo ratings yet
- BR J Haematol - 2016 - New - Guidelines On Transfusion For Fetuses Neonates and Older ChildrenDocument45 pagesBR J Haematol - 2016 - New - Guidelines On Transfusion For Fetuses Neonates and Older Childrensanjeev kumarNo ratings yet
- Major Postpartum Blood Loss and Massive Transfusion in A Tertiary Hospital Innorthcentral Nigeria Case Report 2161 0932 1000280Document5 pagesMajor Postpartum Blood Loss and Massive Transfusion in A Tertiary Hospital Innorthcentral Nigeria Case Report 2161 0932 1000280DownloadNo ratings yet
- Management of Atonic Post Partum HemorrhageDocument4 pagesManagement of Atonic Post Partum HemorrhageArnis Putri RosyaniNo ratings yet
- 2016 Management of Severe Hypertension in PregnancyDocument7 pages2016 Management of Severe Hypertension in PregnancyMaria del Pilar Devis MoralesNo ratings yet
- Hematological Profile of Pregnant Women at St. Paul 'S Hospital Millennium Medical College, Addis Ababa, EthiopiaDocument7 pagesHematological Profile of Pregnant Women at St. Paul 'S Hospital Millennium Medical College, Addis Ababa, Ethiopiaade lydia br.siregarNo ratings yet
- Apendicitis y Embarazo 1Document6 pagesApendicitis y Embarazo 1Bernardo RomeroNo ratings yet
- Jurnal Abrupsio PlasentaDocument13 pagesJurnal Abrupsio Plasentaperussi pranadiptaNo ratings yet
- Slide Obgyn Jurnal ReadingDocument18 pagesSlide Obgyn Jurnal Readingari naNo ratings yet
- Pregnancy and Cirrhosis: ReviewDocument11 pagesPregnancy and Cirrhosis: ReviewBahrunNo ratings yet
- Ra4688 Reyes, Jeanneclaire Mmls2-1Document46 pagesRa4688 Reyes, Jeanneclaire Mmls2-1Jeanne ClaireNo ratings yet
- Whole-Body Vibration and Postural Stress Among Operators - CDCDocument7 pagesWhole-Body Vibration and Postural Stress Among Operators - CDCPierre BouvierNo ratings yet
- The 19th Australasian Plant Pathology Conference, 2013, Auckland, New ZealandDocument190 pagesThe 19th Australasian Plant Pathology Conference, 2013, Auckland, New Zealandamir-scribdNo ratings yet
- PathophysioDocument2 pagesPathophysioSheng DekitNo ratings yet
- Preoperative AssessmentDocument3 pagesPreoperative AssessmentStepyn SalvadorNo ratings yet
- Turnip Mosaic Virus (Tumv) Is A Virus That Commonly Infects Vegetable CropsDocument10 pagesTurnip Mosaic Virus (Tumv) Is A Virus That Commonly Infects Vegetable CropsandreNo ratings yet
- Pathology & Clinical Laboratory (M) SDN - BHD: HaematologyDocument2 pagesPathology & Clinical Laboratory (M) SDN - BHD: HaematologyHANIFNo ratings yet
- The Neuroscience On The Web SeriesDocument4 pagesThe Neuroscience On The Web SeriesAdrian FernandezNo ratings yet
- StabilityDocument21 pagesStabilityDrYashvi ShahNo ratings yet
- Benign Breast Lesions: LT Col Deep Kumar Raman., MD., DNB., Classified Specialist (Pathology)Document28 pagesBenign Breast Lesions: LT Col Deep Kumar Raman., MD., DNB., Classified Specialist (Pathology)uniquelydeep7208No ratings yet
- Rapid Neuro ExamDocument17 pagesRapid Neuro ExamJob KhanNo ratings yet
- Gastrointestinal SystemDocument9 pagesGastrointestinal SystemMikaella CondeNo ratings yet
- 2.home Based Palliative Care2-Dr. Hendri Pangestu, SpAn KICDocument18 pages2.home Based Palliative Care2-Dr. Hendri Pangestu, SpAn KICRuki HartawanNo ratings yet
- ZikaDocument3 pagesZikaapi-298247873No ratings yet
- The Effect of Covid-19 in KabaddiDocument25 pagesThe Effect of Covid-19 in KabaddiShadman RafidNo ratings yet
- Kader Presentation 2Document35 pagesKader Presentation 2Khader Axmed MaxamedNo ratings yet
- Uts 4Document16 pagesUts 4raine zapantaNo ratings yet
- Fluid, Electrolyte, Acid Base BalanceDocument42 pagesFluid, Electrolyte, Acid Base BalanceSutrisno YangNo ratings yet
- CriteriaDocument2 pagesCriteriarh 077No ratings yet
- Bonnie Prince BillyDocument43 pagesBonnie Prince Billycajun28No ratings yet
- Undescended Testes (Orchidopexy)Document9 pagesUndescended Testes (Orchidopexy)nuranysha havizNo ratings yet
- Evaluation of Atosiban Therapy in The Management of Preterm Labour in Indian PatientsDocument13 pagesEvaluation of Atosiban Therapy in The Management of Preterm Labour in Indian PatientsRereroroNo ratings yet
- Msds Potassium Chloride 0.1MDocument5 pagesMsds Potassium Chloride 0.1MNicholas Chan100% (1)
- Ielts Vocab WorksheetsDocument36 pagesIelts Vocab WorksheetsMannJotNo ratings yet
- Environmental Factors Affecting HealthDocument86 pagesEnvironmental Factors Affecting Healthsufian abdo jiloNo ratings yet
- Arun Venkatesh SDocument147 pagesArun Venkatesh SMuhammad RahmatullahNo ratings yet