You might also like
- Aortic RegurgitationFrom EverandAortic RegurgitationJan VojacekNo ratings yet
- Decoding Cardiac Electrophysiology: Understanding the Techniques and Defining the JargonFrom EverandDecoding Cardiac Electrophysiology: Understanding the Techniques and Defining the JargonAfzal SohaibNo ratings yet
- Es 01Document5 pagesEs 01Anubhav ChoudhuryNo ratings yet
- 9 IABP and Plasmapheresis (4 Files Merged)Document48 pages9 IABP and Plasmapheresis (4 Files Merged)Alaa OmarNo ratings yet
- 朱家权氯沙坦猪模型Document10 pages朱家权氯沙坦猪模型shentujin1997No ratings yet
- TEE For ImpellaDocument6 pagesTEE For ImpellaPriya Nair MenonNo ratings yet
- How To Perform A Transseptal Puncture: Mark J EarleyDocument9 pagesHow To Perform A Transseptal Puncture: Mark J EarleyAttilio Del RossoNo ratings yet
- The Blalock and Taussig Shunt Revisited: Review ArticleDocument8 pagesThe Blalock and Taussig Shunt Revisited: Review ArticlearwitarahayuNo ratings yet
- Intra-Aortic Balloon Counterpulsation Therapy and Its Role in Optimizing Outcomes in Cardiac SurgeryDocument31 pagesIntra-Aortic Balloon Counterpulsation Therapy and Its Role in Optimizing Outcomes in Cardiac SurgeryHendrik AbrahamNo ratings yet
- Cap 2013 NejmDocument7 pagesCap 2013 NejmpaulaandreavargasbNo ratings yet
- Advanced Cardiopulmonary Support For Pulmonary EmbolismDocument6 pagesAdvanced Cardiopulmonary Support For Pulmonary EmbolismJavier Enrique Barrera PachecoNo ratings yet
- Results With Continuous Cardiopulmonary Bypass For The Bidirectional Cavopulmonary Anastomosis - ProQuestDocument7 pagesResults With Continuous Cardiopulmonary Bypass For The Bidirectional Cavopulmonary Anastomosis - ProQuestWilliam WiryawanNo ratings yet
- Swan GanzDocument35 pagesSwan Ganzdrivaner1No ratings yet
- 2022 - Anesthetic Management For Open Thoracoabdominal and Abdominal Aortic Aneurysm RepairDocument14 pages2022 - Anesthetic Management For Open Thoracoabdominal and Abdominal Aortic Aneurysm RepairLaura Camila RiveraNo ratings yet
- Smith 2013 SMIIDocument9 pagesSmith 2013 SMIIGryseldaGryGryNo ratings yet
- Resuscitativeendovascular Balloonocclusionofthe Aorta:: A Practical ReviewDocument18 pagesResuscitativeendovascular Balloonocclusionofthe Aorta:: A Practical ReviewJulian SanchezNo ratings yet
- Bootsma2021 Article TheContemporaryPulmonaryArteryDocument11 pagesBootsma2021 Article TheContemporaryPulmonaryArteryElenaCondratscribdNo ratings yet
- Transesophageal Echocardiography: The Hemodynamic Monitoring UtilizingDocument14 pagesTransesophageal Echocardiography: The Hemodynamic Monitoring UtilizingvegasbabyNo ratings yet
- Procedure-IABP InsertionDocument19 pagesProcedure-IABP Insertionmohamad dildarNo ratings yet
- RushDocument28 pagesRushEdson Alanez BautistaNo ratings yet
- ANMCO POSITION PAPER Role of Intra-Aortic BalloonDocument17 pagesANMCO POSITION PAPER Role of Intra-Aortic BalloonapipNo ratings yet
- Meccanical SupportDocument19 pagesMeccanical SupportAttilio Del RossoNo ratings yet
- Hepatology - 2004 - Colle - Diagnosis of Portopulmonary Hypertension in Candidates For Liver Transplantation A ProspectiveDocument9 pagesHepatology - 2004 - Colle - Diagnosis of Portopulmonary Hypertension in Candidates For Liver Transplantation A ProspectiveYasin DeveliogluNo ratings yet
- Unit 6 Cardiac Catheterization and AngiographyDocument28 pagesUnit 6 Cardiac Catheterization and AngiographyJack Tomar100% (1)
- Arterial LineDocument2 pagesArterial LineRaghav Goyal100% (1)
- Parissis 2016 IABP - History-Evolution-Pathophysiologyindications What We Need To KnowDocument13 pagesParissis 2016 IABP - History-Evolution-Pathophysiologyindications What We Need To KnowQuincy93No ratings yet
- Heart Review Article PapworthDocument9 pagesHeart Review Article PapworthTài NguyễnNo ratings yet
- ImpellaDocument5 pagesImpellapuspaNo ratings yet
- Current Strategies of Spinal Cord Protection During Thoracoabdom 2018Document8 pagesCurrent Strategies of Spinal Cord Protection During Thoracoabdom 2018Angel VillaNo ratings yet
- Gibson 2013Document14 pagesGibson 2013Moisés Alberto CharajaNo ratings yet
- WEEK 7 - PERFUSION TECHNOLOGY v2Document44 pagesWEEK 7 - PERFUSION TECHNOLOGY v2Marc Jeff GabasaNo ratings yet
- Manejo FontanDocument11 pagesManejo FontanAngélica ContrerasNo ratings yet
- HM3 in FontonDocument2 pagesHM3 in FontonselvakumarNo ratings yet
- AblacionDocument7 pagesAblaciontomasvainsteinNo ratings yet
- Kim2012Document5 pagesKim2012Stefanie MelisaNo ratings yet
- 1 s2.0 S1053077022007510 MainDocument16 pages1 s2.0 S1053077022007510 MainCristhian BastidasNo ratings yet
- Borenstein 05Document9 pagesBorenstein 05emmanuel le bretNo ratings yet
- 480 FullDocument6 pages480 FullStamenko S. SusakNo ratings yet
- Dixon SRDocument6 pagesDixon SRG WNo ratings yet
- 1 s2.0 S0022522312009099 MainDocument9 pages1 s2.0 S0022522312009099 MainFayaNuraldaSitompulNo ratings yet
- Article - Sequential Bypass Grafting On The Beating Heart - Blood Flow CharacteristicsDocument4 pagesArticle - Sequential Bypass Grafting On The Beating Heart - Blood Flow Characteristicsfluid_man_brazilNo ratings yet
- Hypoxia and Complications of Oxygenation in Extracorporeal Membrane OxygenationDocument7 pagesHypoxia and Complications of Oxygenation in Extracorporeal Membrane Oxygenationjq4rhbh2pzNo ratings yet
- TOFPA: A Surgical Approach To Tetralogy of Fallot With Pulmonary AtresiaDocument24 pagesTOFPA: A Surgical Approach To Tetralogy of Fallot With Pulmonary AtresiaRedmond P. Burke MD100% (1)
- Cardiopulmonary Bypass: Learning ObjectivesDocument5 pagesCardiopulmonary Bypass: Learning ObjectivesAnonymous zPwXqwNo ratings yet
- Intra Aortic Balloon Pump (IABP) : Past, Present and FutureDocument10 pagesIntra Aortic Balloon Pump (IABP) : Past, Present and FutureAlladi SrujanNo ratings yet
- The RUSH Exam - Rapid Ultrasound in SHock in The Evaluation of The Critically LLLDocument28 pagesThe RUSH Exam - Rapid Ultrasound in SHock in The Evaluation of The Critically LLLCARLOSNo ratings yet
- Extracorporeal Oxygenation Prolonged Cardiopulmonary Bypass: (ECMO)Document11 pagesExtracorporeal Oxygenation Prolonged Cardiopulmonary Bypass: (ECMO)Almira IsmaryadiNo ratings yet
- CANULADocument12 pagesCANULAAlejandro Salazar TorresNo ratings yet
- Physical Exercise Reduces Transplant Arteriosclerosis in A Mouse Aorta Transplantation ModelDocument8 pagesPhysical Exercise Reduces Transplant Arteriosclerosis in A Mouse Aorta Transplantation ModelNicoleta Popa-FoteaNo ratings yet
- We Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsDocument13 pagesWe Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsAfnan MoeNo ratings yet
- Cardiac CatheterizationDocument9 pagesCardiac CatheterizationAnurag Gupta100% (1)
- Extracorporeal Membrane Oxygenation in Critically Ill ChildrenDocument16 pagesExtracorporeal Membrane Oxygenation in Critically Ill ChildrenEduardo Rios DuboisNo ratings yet
- Apm 12 151 PDFDocument4 pagesApm 12 151 PDFFityan Aulia RahmanNo ratings yet
- SN02Document11 pagesSN02Enrique San NorbertoNo ratings yet
- 00 - Physiologic Monitoring Systems, Cardiac CatheterizationDocument17 pages00 - Physiologic Monitoring Systems, Cardiac Catheterizationhabitar.unitpacNo ratings yet
- Belhajsoulami 2018Document3 pagesBelhajsoulami 2018rédaNo ratings yet
- Cardio ResusiDocument9 pagesCardio ResusiDanarFauzanAdiPrayitnoNo ratings yet
- 朱家权1Document9 pages朱家权1shentujin1997No ratings yet
- Piis0007091217459812 PDFDocument10 pagesPiis0007091217459812 PDFAnonymous 1uP0mbNo ratings yet
- Cardiac Surgical Operative AtlasFrom EverandCardiac Surgical Operative AtlasThorsten WahlersNo ratings yet
- Point of Care Ultrasound With Pocket Size Devices in Emergency Department - 2019Document10 pagesPoint of Care Ultrasound With Pocket Size Devices in Emergency Department - 2019ntnquynhproNo ratings yet
- Circulatory System MatchDocument2 pagesCirculatory System MatchInternational Tutoring Association50% (2)
- Bailey JMDocument9 pagesBailey JMPedro VillamorNo ratings yet
- 10 Powerful Herbs For Protection SpellsDocument6 pages10 Powerful Herbs For Protection SpellsWayne SmithNo ratings yet
- 5 Min - PTMCDocument28 pages5 Min - PTMCAsim Kumar BiswasNo ratings yet
- Vital Signs Procedures ChecklistDocument3 pagesVital Signs Procedures Checklistjuancristo91% (22)
- Blood Pressure GuidelineDocument2 pagesBlood Pressure Guidelineadequatelatitude1715No ratings yet
- Numen Program InformationDocument7 pagesNumen Program InformationysjaitawatNo ratings yet
- 1991 CuminsDocument14 pages1991 CuminsScience BrasilNo ratings yet
- PowerpointDocument12 pagesPowerpointapi-585922320No ratings yet
- Project BioDocument18 pagesProject Bioyanshu falduNo ratings yet
- Anatomy For Beginners 2 - CirculationDocument18 pagesAnatomy For Beginners 2 - CirculationDefy R PradentyNo ratings yet
- Blood Pressure ChartDocument27 pagesBlood Pressure ChartRamakrishna Kurapati100% (1)
- A Review of The Fundamental Principles and Evidence Base in The Use of Extracorporeal MembraneOxygenation (ECMO) in Critically Ill Adult PatientsDocument15 pagesA Review of The Fundamental Principles and Evidence Base in The Use of Extracorporeal MembraneOxygenation (ECMO) in Critically Ill Adult PatientsGenaro MendozaNo ratings yet
- Bencito ResumeDocument2 pagesBencito ResumeRebecca ObinsaNo ratings yet
- Cardiac Failure ChiongDocument4 pagesCardiac Failure ChiongJohn Miguel ChiongNo ratings yet
- Pathophysiology of Congenital Heart Disease in The Adult: Special ReportDocument10 pagesPathophysiology of Congenital Heart Disease in The Adult: Special ReportLwin ThantNo ratings yet
- AHA 2017 Cardiogenic ShockDocument37 pagesAHA 2017 Cardiogenic ShockAnastasyaLianNo ratings yet
- Angiografi Koroner: Indikasi, Kontraindikasi, Dan Proteksi Terhadap RadiasiDocument6 pagesAngiografi Koroner: Indikasi, Kontraindikasi, Dan Proteksi Terhadap Radiasihindri royiah fatmaNo ratings yet
- Discharge Planning For Acute Coronary Syndrome Patients in A Tertiary Hospital: A Best Practice Implementation ProjectDocument17 pagesDischarge Planning For Acute Coronary Syndrome Patients in A Tertiary Hospital: A Best Practice Implementation ProjectMukhlis HasNo ratings yet
- Adapta Versa®sensiaDocument346 pagesAdapta Versa®sensiabobo samNo ratings yet
- Dr. Sunatrio - Management Hypovolemic ShockDocument59 pagesDr. Sunatrio - Management Hypovolemic ShockArga Putra SaboeNo ratings yet
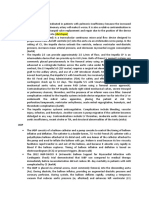
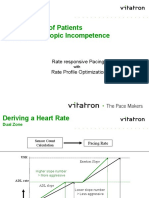
- Managing Chronotropic IncompetenceDocument9 pagesManaging Chronotropic IncompetenceCarlos PortaNo ratings yet
- Angina PectorisDocument24 pagesAngina PectorisDr AUNo ratings yet
- 3.4 Blood PressureDocument50 pages3.4 Blood Pressure091Nurul Nur AkmalNo ratings yet
- Blow Hot Blow Cold: Class VDocument2 pagesBlow Hot Blow Cold: Class VAnita PandeyNo ratings yet
- Pengaruh Latihan Basic Life Support Terhadap Pengetahuan Dan Keterampilan Tim MuhammadiyahDocument8 pagesPengaruh Latihan Basic Life Support Terhadap Pengetahuan Dan Keterampilan Tim Muhammadiyahanna sariNo ratings yet
- Esperion NEXLETOL - NEXLIZET HCP 1 PagerDocument2 pagesEsperion NEXLETOL - NEXLIZET HCP 1 PagerMoussa AmerNo ratings yet
- أدوية الضغطDocument2 pagesأدوية الضغطSamalout Specialized HospitalNo ratings yet
- RAVEL 4 AnosDocument13 pagesRAVEL 4 AnosRui FonteNo ratings yet