You might also like
- Clinical SignificanceDocument31 pagesClinical Significancejav israelNo ratings yet
- DiabetesDocument12 pagesDiabetessshiffanaNo ratings yet
- CukrzycaDocument52 pagesCukrzycatyhbbhhNo ratings yet
- Diabetes MellitusDocument59 pagesDiabetes Mellitusuzzal ahmedNo ratings yet
- Diabetes MellitusDocument60 pagesDiabetes MellitusVytheeshwaran Vedagiri96% (26)
- Dka (Picucourse)Document33 pagesDka (Picucourse)surasuarezlopezNo ratings yet
- Obesitas Mets DMDocument47 pagesObesitas Mets DMFathimah UswahNo ratings yet
- Nursing Care of PT With DiabetesDocument71 pagesNursing Care of PT With DiabetesEricka Lj Robles DimaculanganNo ratings yet
- Diabetes MellitusDocument59 pagesDiabetes Mellituslailatul rofiahNo ratings yet
- OMD-4 Diagnosis and Dental Managment of Diabetes Mellitus Lecture HandoutDocument13 pagesOMD-4 Diagnosis and Dental Managment of Diabetes Mellitus Lecture Handouthananalkadi94No ratings yet
- Diabetes Mellitus: - ClassificationDocument22 pagesDiabetes Mellitus: - ClassificationFernando Junior Parra UchasaraNo ratings yet
- Lecture 28 - Pathology of DiabetesDocument34 pagesLecture 28 - Pathology of Diabetesapi-3703352100% (4)
- Week4 EndocrineDocument84 pagesWeek4 EndocrineriverabeanicoNo ratings yet
- Group 2 DkaDocument73 pagesGroup 2 DkaAkio Ozaraga100% (1)
- Diabetic Ketoacidosis (Redirected From)Document11 pagesDiabetic Ketoacidosis (Redirected From)Angelyn Bombase100% (1)
- Metabolic EmergenciesDocument53 pagesMetabolic EmergenciesWengel Redkiss100% (1)
- A Presentation On: Diabetes MellitusDocument17 pagesA Presentation On: Diabetes MellitusAnil YadavNo ratings yet
- Diabetes Mellitus: Majuvy L. Sulse MSN, RN, CCRN Lola Oyedele MSN, RN, CTNDocument54 pagesDiabetes Mellitus: Majuvy L. Sulse MSN, RN, CCRN Lola Oyedele MSN, RN, CTNDaffa AfifNo ratings yet
- Presentation On Diabetes MellitusDocument47 pagesPresentation On Diabetes Mellitusankita guptaNo ratings yet
- Diabetes Mellitus and Its Emergencies 1Document35 pagesDiabetes Mellitus and Its Emergencies 1Varun R'MenonNo ratings yet
- 003 - DM - Acute ComplicationsDocument17 pages003 - DM - Acute ComplicationsLucas Victor AlmeidaNo ratings yet
- Acute Complications of DMDocument57 pagesAcute Complications of DMMalueth AnguiNo ratings yet
- DM FinalDocument58 pagesDM FinalMalueth AnguiNo ratings yet
- CH 67Document40 pagesCH 67Valentina LajqiNo ratings yet
- Chapter 4 Carbohydrate DisorderDocument26 pagesChapter 4 Carbohydrate DisorderNida RidzuanNo ratings yet
- Metabolic SyndromeDocument55 pagesMetabolic SyndromeAakash BalasubramanianNo ratings yet
- Diabetic Complication (Ketotic)Document21 pagesDiabetic Complication (Ketotic)daniyal kumarNo ratings yet
- Acute and Chronic DM ComplicationsDocument29 pagesAcute and Chronic DM ComplicationsJennicaNo ratings yet
- Presenter: Ho. Louis Dor Deng Moderator: DR Pawil Arop Consultant PhysicianDocument60 pagesPresenter: Ho. Louis Dor Deng Moderator: DR Pawil Arop Consultant PhysicianBol Dhalbeny MalualNo ratings yet
- Blood GlucoseDocument8 pagesBlood Glucoseعبدالرحمن عابدNo ratings yet
- W02 - Diabetic Emergencies in CCDocument36 pagesW02 - Diabetic Emergencies in CCHelene AlawamiNo ratings yet
- NITHISHDocument96 pagesNITHISHsj computersNo ratings yet
- Management of Diabetes Emergencies''Document85 pagesManagement of Diabetes Emergencies''Princewill SeiyefaNo ratings yet
- Paper ElektifDocument10 pagesPaper Elektifamyliadwi22No ratings yet
- Caso 59 DiabetesDocument4 pagesCaso 59 DiabetesLaura ContrerasNo ratings yet
- Diabetes Mellitus: Prepared by Divya Bhusal B.SC - Nursing 3 YearDocument43 pagesDiabetes Mellitus: Prepared by Divya Bhusal B.SC - Nursing 3 YearSristi LamsalNo ratings yet
- Ospe Case Discussion: Presenter - Dr. Salma Ahmed Dept. of BiochemistryDocument29 pagesOspe Case Discussion: Presenter - Dr. Salma Ahmed Dept. of BiochemistryManashi JalanNo ratings yet
- Diabetic Ketoacidosis: Presented by NG YHDocument32 pagesDiabetic Ketoacidosis: Presented by NG YHYuki NgNo ratings yet
- Diabetes MellitusDocument9 pagesDiabetes MellitusM. Joyce100% (2)
- Patologi Pankreas Endokrin & AdrenalDocument69 pagesPatologi Pankreas Endokrin & AdrenalSonia Afika AzizaNo ratings yet
- GROUP 4 - HyperglikemiDocument5 pagesGROUP 4 - Hyperglikemiamyliadwi22No ratings yet
- Diabetes MellitusDocument30 pagesDiabetes Mellitusurusha vaidyaNo ratings yet
- Diabetic EmergenciesDocument96 pagesDiabetic EmergenciesSoze KeyserNo ratings yet
- Diabetic Emergencies and ManagementDocument41 pagesDiabetic Emergencies and ManagementNali peterNo ratings yet
- Diabetes Mellitus: April 2014Document41 pagesDiabetes Mellitus: April 2014Koricho MengistuNo ratings yet
- Diabetic Ketoacidosis in ChildrenDocument39 pagesDiabetic Ketoacidosis in ChildrenRichard SiahaanNo ratings yet
- Medical EmergenciesDocument12 pagesMedical EmergenciesBSN 2 - Sasis, Rusmaryte C.No ratings yet
- L11 Diabetes MellitusDocument61 pagesL11 Diabetes MellitusYosra —No ratings yet
- Diabetic KetoacidosisDocument6 pagesDiabetic KetoacidosisRain Catan Gagarra Saquin100% (1)
- Diabetes Mellitus.U.iiDocument38 pagesDiabetes Mellitus.U.iitamtamtamtama0No ratings yet
- Diabetic KetoacidosisDocument16 pagesDiabetic Ketoacidosisjoyshe111100% (2)
- Acute Complications of Diabetes Mellitus: DR Yemane G (MD, Assis. Prof. EMCC)Document63 pagesAcute Complications of Diabetes Mellitus: DR Yemane G (MD, Assis. Prof. EMCC)yared getachewNo ratings yet
- Diabetes Mellitus: Fatimah ElianaDocument61 pagesDiabetes Mellitus: Fatimah ElianaOoy RokayahNo ratings yet
- Diabetes MellitusDocument52 pagesDiabetes MellitusMervis masatunyaNo ratings yet
- Diabetes KetoacidosisDocument35 pagesDiabetes KetoacidosisdaniejayanandNo ratings yet
- Diabetes MellitusDocument29 pagesDiabetes MellitusSyed MaazNo ratings yet
- BONISHADocument40 pagesBONISHAsj computersNo ratings yet
- Final Diabetes & Its Role in PeriodonticsDocument140 pagesFinal Diabetes & Its Role in Periodonticsvinay jainNo ratings yet
- Soluzioni al Diabete e all'Ipoglicemia - Come prevenire e disfarsene naturalmente e senza medicineFrom EverandSoluzioni al Diabete e all'Ipoglicemia - Come prevenire e disfarsene naturalmente e senza medicineNo ratings yet
- Diabetic Recipes for One and TwoFrom EverandDiabetic Recipes for One and TwoRating: 3 out of 5 stars3/5 (1)
- Morning Report Case Presentation: APRIL 1, 2019Document14 pagesMorning Report Case Presentation: APRIL 1, 2019Emily EresumaNo ratings yet
- 2007 India CBSE Fact Sheet PDFDocument2 pages2007 India CBSE Fact Sheet PDFShanthi HariharanNo ratings yet
- Shutter Island Opening Sequence AnalysisDocument5 pagesShutter Island Opening Sequence AnalysiszoiaNo ratings yet
- What Is Hormonal ImbalanceDocument2 pagesWhat Is Hormonal ImbalancestimunoNo ratings yet
- Slide Kuliah FK USU ArrhythmiaDocument40 pagesSlide Kuliah FK USU ArrhythmiaYolanda SimamoraNo ratings yet
- Cardiology MnemonicsDocument18 pagesCardiology MnemonicsAnnapurna Dangeti100% (1)
- Risk Predictors in Periodontal DiseaseDocument8 pagesRisk Predictors in Periodontal DiseaseShreyaNo ratings yet
- PREFACE: " Chronic Fatigue Syndrome: A Guide To The Homeopathic Treatment of CFS/M.E."Document5 pagesPREFACE: " Chronic Fatigue Syndrome: A Guide To The Homeopathic Treatment of CFS/M.E."Diane SolomonNo ratings yet
- Medical Terms (Prefixes Suffixes Roots)Document5 pagesMedical Terms (Prefixes Suffixes Roots)David Donovan ManuelNo ratings yet
- Ethics Uworld NotesDocument3 pagesEthics Uworld NotesActeen MyoseenNo ratings yet
- Little Orange Book v3 With Searchable Index PDFDocument52 pagesLittle Orange Book v3 With Searchable Index PDFiaxableNo ratings yet
- Water and Reproductive Health 2Document18 pagesWater and Reproductive Health 2Female calmNo ratings yet
- Final Thesis - BreastfeedingDocument19 pagesFinal Thesis - BreastfeedingNazria Gilman Kapusan75% (4)
- Critical Evaluation of Diagnostic SystemDocument6 pagesCritical Evaluation of Diagnostic SystemAnanya100% (1)
- Vaccination As A Cause of Autism-Myths and ControversiesDocument6 pagesVaccination As A Cause of Autism-Myths and ControversiesAndyNo ratings yet
- L1 Hypo, Hyperthyroidism and Hashimoto ThyroiditisDocument12 pagesL1 Hypo, Hyperthyroidism and Hashimoto ThyroiditisSivaNo ratings yet
- Assessment of The Efficacy of Surya Namaskar in Management of SthaulyaDocument10 pagesAssessment of The Efficacy of Surya Namaskar in Management of Sthaulyans.saiprashanthNo ratings yet
- Laboratory Results & InterpretationDocument11 pagesLaboratory Results & InterpretationLjae NatinoNo ratings yet
- Pathology FinalADocument72 pagesPathology FinalAvaegmundig100% (1)
- Psychiatric Nursing: What Is Mental Health Disorder? SilenceDocument11 pagesPsychiatric Nursing: What Is Mental Health Disorder? SilenceJek Dela CruzNo ratings yet
- Viral Infection AHEADDocument24 pagesViral Infection AHEADShiena Mae PelagioNo ratings yet
- Acute Arthritis: BY Dr. Mehrunnisa UmarDocument64 pagesAcute Arthritis: BY Dr. Mehrunnisa UmardrusmanjamilhcmdNo ratings yet
- Oral Hypoglycemic DrugsDocument26 pagesOral Hypoglycemic DrugsBansal Mohit100% (1)
- Medical-Surgical Nursing ArthritisDocument8 pagesMedical-Surgical Nursing ArthritisNoelyn BaluyanNo ratings yet
- Measure of The DiseaseDocument13 pagesMeasure of The DiseaseGhada ElhassanNo ratings yet
- Lecture - Chapter 7 - Environmental ToxicologyDocument31 pagesLecture - Chapter 7 - Environmental ToxicologyMarieGraceArmada-viudaDe-OrdonioNo ratings yet
- PDF DIR 456Document6 pagesPDF DIR 456Fauzan MaulanaNo ratings yet
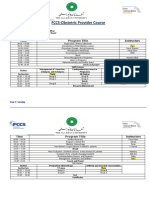
- FCCS-Obstetric Provider Course: Time Program Title InstructorsDocument2 pagesFCCS-Obstetric Provider Course: Time Program Title InstructorsSamina AyazNo ratings yet
- Medical Terminology For Health Professions 8th Edition Ehrlich Test BankDocument12 pagesMedical Terminology For Health Professions 8th Edition Ehrlich Test Bankjamesbyrdcxgsaioymf93% (15)
- MKSAP 16 - Infectious DiseaseDocument340 pagesMKSAP 16 - Infectious DiseaseBacanator75% (4)