You might also like
- Smoking Cessation Questionnaire SurveyDocument3 pagesSmoking Cessation Questionnaire SurveyAhmad Tarmizi Ahmad Zawawi100% (1)
- UNLICOMMTobacco Use TBE02182008Document3 pagesUNLICOMMTobacco Use TBE02182008ZahraNo ratings yet
- Smoking QuestionnaireDocument29 pagesSmoking QuestionnaireDefault UserNo ratings yet
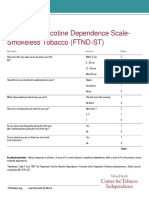
- FTND-ST Smokeless Tobacco Dependence ScaleDocument1 pageFTND-ST Smokeless Tobacco Dependence ScaleHemantNo ratings yet
- Cigarette Smoking: What It’s Doing to Smokers and NonsmokersFrom EverandCigarette Smoking: What It’s Doing to Smokers and NonsmokersNo ratings yet
- NIDA Clinical Trials Network Fagerstrom Test For Nicotine Dependence (FND)Document2 pagesNIDA Clinical Trials Network Fagerstrom Test For Nicotine Dependence (FND)Chris DubuqueNo ratings yet
- Group Counseling GuideDocument13 pagesGroup Counseling GuideNurses For Tobacco ControlNo ratings yet
- Porcupine Health Unit Quit Smoking Clinic - Intake QuestionnaireDocument7 pagesPorcupine Health Unit Quit Smoking Clinic - Intake QuestionnaireRohan PhilipsNo ratings yet
- I Don't Smoke!: A Guidebook to Break Your Addiction to NicotineFrom EverandI Don't Smoke!: A Guidebook to Break Your Addiction to NicotineNo ratings yet
- Tobacco Cess Miniworkbk Eng Final 508Document27 pagesTobacco Cess Miniworkbk Eng Final 508helfiNo ratings yet
- The Placebo Method To Quit SmokingDocument5 pagesThe Placebo Method To Quit SmokingGary SmithNo ratings yet
- Intervensi Farmakologi Berhenti Merokok (Taklimat Berhenti Merokok 17 Jul 2010)Document31 pagesIntervensi Farmakologi Berhenti Merokok (Taklimat Berhenti Merokok 17 Jul 2010)albeny j.pNo ratings yet
- Quit Smoking Success: Practical Advice to Help You Quit Smoking for Good!From EverandQuit Smoking Success: Practical Advice to Help You Quit Smoking for Good!No ratings yet
- No More Ashtrays: The pocket guide to quitting smokingFrom EverandNo More Ashtrays: The pocket guide to quitting smokingRating: 5 out of 5 stars5/5 (2)
- Appendix 1 - Vaping Questionnaire and Penn State Dependence IndexDocument2 pagesAppendix 1 - Vaping Questionnaire and Penn State Dependence IndexFadel Yusri JabariNo ratings yet
- Finally Free!: The Easy Way for Women to Stop SmokingFrom EverandFinally Free!: The Easy Way for Women to Stop SmokingRating: 3 out of 5 stars3/5 (10)
- Smoking QuestionnaireDocument4 pagesSmoking QuestionnaireChaddy Morente100% (1)
- Smoking Survey - 10 Questions: Page 1 of 2Document45 pagesSmoking Survey - 10 Questions: Page 1 of 2anirNo ratings yet
- PROJECT VAPE - Research QuestionDocument1 pagePROJECT VAPE - Research QuestionRYAN FERNANDEZNo ratings yet
- Only. Do Not Duplicate.: An OverviewDocument18 pagesOnly. Do Not Duplicate.: An OverviewOvidiu AndroneNo ratings yet
- Stopsmoking 2Document22 pagesStopsmoking 2willpccamaraNo ratings yet
- Quitting for the Life of You: A mind over matter approach to quitting smokingFrom EverandQuitting for the Life of You: A mind over matter approach to quitting smokingNo ratings yet
- Community survey examines health issues, lifestyle factors and information accessDocument7 pagesCommunity survey examines health issues, lifestyle factors and information accessRamiel Agan GuinandamNo ratings yet
- 7-Day Quit Smoking Challenge: Ways to Quit Smoking In 7 DaysFrom Everand7-Day Quit Smoking Challenge: Ways to Quit Smoking In 7 DaysNo ratings yet
- Smoking Survey - 10 Questions: 1. Page 1 of 2Document11 pagesSmoking Survey - 10 Questions: 1. Page 1 of 2Sandhya NatarajanNo ratings yet
- Easy Way to Quit Smoking: Complete Guide to Staying Off Cigarettes for GoodFrom EverandEasy Way to Quit Smoking: Complete Guide to Staying Off Cigarettes for GoodNo ratings yet
- NOT Copy: 2018-19 Student SurveyDocument6 pagesNOT Copy: 2018-19 Student SurveyWojciech PoznańskiNo ratings yet
- How I Quit Smoking in 1 Day... And How You Can Too!: A Simple, Step-By-Step Guide To Quit Smoking For Good, Without the Stress.From EverandHow I Quit Smoking in 1 Day... And How You Can Too!: A Simple, Step-By-Step Guide To Quit Smoking For Good, Without the Stress.Rating: 4.5 out of 5 stars4.5/5 (11)
- Stop SmokingDocument16 pagesStop Smokingeduardo virgilioNo ratings yet
- Pharmaco - Smoking Cessation DR Ho 2017Document55 pagesPharmaco - Smoking Cessation DR Ho 2017Keluang Man WinchesterNo ratings yet
- Psychiatry HandbookDocument86 pagesPsychiatry HandbookDIA PHONG THANGNo ratings yet
- I Quit!: A unique book to help you stop smoking for goodFrom EverandI Quit!: A unique book to help you stop smoking for goodRating: 5 out of 5 stars5/5 (4)
- A New Tried and Proven Formula for Quitting Smoking in Two Weeks Even As a MoronFrom EverandA New Tried and Proven Formula for Quitting Smoking in Two Weeks Even As a MoronNo ratings yet
- A Few Things About Smoking: P. Santamarta // Dpto. Educación Física // I.E.S. El Astillero // Traducido Por J. DíazDocument3 pagesA Few Things About Smoking: P. Santamarta // Dpto. Educación Física // I.E.S. El Astillero // Traducido Por J. Díazkomplease1136No ratings yet
- Static GK For Iift Snap and XatDocument19 pagesStatic GK For Iift Snap and XatnavinkumargNo ratings yet
- ) (Significant Digits Are Bounded To 1 Due To 500m. However I Will Use 2SD To Make More Sense of The Answers)Document4 pages) (Significant Digits Are Bounded To 1 Due To 500m. However I Will Use 2SD To Make More Sense of The Answers)JeevikaGoyalNo ratings yet
- Workday Studio - Complex Integration Tool OverviewDocument3 pagesWorkday Studio - Complex Integration Tool OverviewHarithaNo ratings yet
- HQ 170aDocument82 pagesHQ 170aTony WellsNo ratings yet
- Discharging A ClientDocument6 pagesDischarging A ClientNorman Batalla Juruena, DHCM, PhD, RNNo ratings yet
- Filling Out Forms Detailed Lesson Plan in English VDocument9 pagesFilling Out Forms Detailed Lesson Plan in English VAIAN CALIBAYAN0% (1)
- Basf TapesDocument3 pagesBasf TapesZoran TevdovskiNo ratings yet
- Inductive sensor technical specifications in 40 charactersDocument3 pagesInductive sensor technical specifications in 40 charactersBasarNo ratings yet
- Drive Unit TENH EH 10003, 225, 50/60Hz 400/440V: Qty. Description Specification Material Size DT Doc IdDocument1 pageDrive Unit TENH EH 10003, 225, 50/60Hz 400/440V: Qty. Description Specification Material Size DT Doc IdKarikalan JayNo ratings yet
- Balcony AnalysysDocument4 pagesBalcony AnalysysKory EstesNo ratings yet
- CH 15 QuizDocument8 pagesCH 15 QuizNelano EastNo ratings yet
- Due Diligence InvestmentsDocument6 pagesDue Diligence InvestmentselinzolaNo ratings yet
- A User's Guide to the Unihan Database: 甲 IntroductionDocument17 pagesA User's Guide to the Unihan Database: 甲 IntroductionAhmd AlfNo ratings yet
- Electrical Machine 7-26-2016Document94 pagesElectrical Machine 7-26-2016Engr. Raheel khanNo ratings yet
- 5 Short MustWatch Motivational Videos For TeachersrccymDocument4 pages5 Short MustWatch Motivational Videos For Teachersrccymfoxpeak8No ratings yet
- Dhaka Epz Factory List & List of Inspected Factories by EIMS For AllianceDocument12 pagesDhaka Epz Factory List & List of Inspected Factories by EIMS For Alliancearman chowdhury100% (4)
- DSRD Ar05Document132 pagesDSRD Ar05djon888No ratings yet
- Instruction Manual For Spider S3 and Spider S4Document6 pagesInstruction Manual For Spider S3 and Spider S4Syah KamalNo ratings yet
- GENERATOR DATA - CaterpillarDocument8 pagesGENERATOR DATA - Caterpillarschraz4575100% (2)
- AI Writing Tools For Social Media Marketing Creating Compelling PostsDocument5 pagesAI Writing Tools For Social Media Marketing Creating Compelling PostsJames DanielsNo ratings yet
- Three Wire MethodDocument4 pagesThree Wire MethodmaivizhiNo ratings yet
- Wedding Planning GuideDocument159 pagesWedding Planning GuideRituparna Majumder0% (1)
- Artificial IntelligenceDocument4 pagesArtificial IntelligencePrax DNo ratings yet
- Nimt Institute of Method & Law, Greater Noida: "Legal Bases and Issues in Scrapping Article 370"Document12 pagesNimt Institute of Method & Law, Greater Noida: "Legal Bases and Issues in Scrapping Article 370"Preetish Sahu100% (1)
- PPE Use Tool Box TalkDocument3 pagesPPE Use Tool Box Talkanon_348105361No ratings yet
- CW3 - 4Document2 pagesCW3 - 4Rigel Zabate100% (1)
- Organophosphorus Pesticide Residues in Vegetables and Soil Samples From Alau Dam and Gongulong Agricultural Areas, Borno State, NigeriaDocument7 pagesOrganophosphorus Pesticide Residues in Vegetables and Soil Samples From Alau Dam and Gongulong Agricultural Areas, Borno State, NigeriaWiro JuangNo ratings yet
- 001-Numerical Solution of Non Linear EquationsDocument16 pages001-Numerical Solution of Non Linear EquationsAyman ElshahatNo ratings yet
- Central Council For Research in Ayurvedic Sciences: CCRAS Post Doctoral Fellowship Scheme (CCRAS PDF Scheme)Document2 pagesCentral Council For Research in Ayurvedic Sciences: CCRAS Post Doctoral Fellowship Scheme (CCRAS PDF Scheme)TUSHAR DASHNo ratings yet
- 20 5880100Document2 pages20 5880100'Theodora GeorgianaNo ratings yet