You might also like
- Clinically Relevant Mycoses: A Practical ApproachFrom EverandClinically Relevant Mycoses: A Practical ApproachElisabeth PresterlNo ratings yet
- Detection of Typhoid CarriersDocument6 pagesDetection of Typhoid CarriersClarestaNo ratings yet
- Cryptosporidiosis in HIV-positive Patients and Related Risk Factors A Systematic Review and Meta-AnalysisDocument19 pagesCryptosporidiosis in HIV-positive Patients and Related Risk Factors A Systematic Review and Meta-AnalysisWiwien HendrawanNo ratings yet
- Opportunistic Digestive Parasitosis in Patients Infected With Human Immunodeficiency Virus in MoroccoDocument7 pagesOpportunistic Digestive Parasitosis in Patients Infected With Human Immunodeficiency Virus in MoroccoIJAR JOURNALNo ratings yet
- Review Jurnal Varicella - Dewi Manik Aulia Fadli - 16700096Document26 pagesReview Jurnal Varicella - Dewi Manik Aulia Fadli - 16700096Lia FadliNo ratings yet
- A 12-Year Retrospective Study of Invasive Amoebiasis in Western Sydney: Evidence of Local AcquisitionDocument8 pagesA 12-Year Retrospective Study of Invasive Amoebiasis in Western Sydney: Evidence of Local AcquisitionAdistyDWNo ratings yet
- Proposal For A Screeming Protocol For Candida AurisDocument6 pagesProposal For A Screeming Protocol For Candida AurisZaenab AzzahraNo ratings yet
- 1 s2.0 S1198743X14632079 MainDocument9 pages1 s2.0 S1198743X14632079 MainAizaz HassanNo ratings yet
- Suspected Urinary Tract Infection in Primary Care, DenmarkDocument6 pagesSuspected Urinary Tract Infection in Primary Care, DenmarkImelda Nafa PawestriNo ratings yet
- LeptospirosisDocument8 pagesLeptospirosisSanda Puspa RiniNo ratings yet
- Study On Invasive Fungal Infections in Immunocompr PDFDocument7 pagesStudy On Invasive Fungal Infections in Immunocompr PDFMelody PardilloNo ratings yet
- Study On Invasive Fungal Infections in Immunocompr PDFDocument7 pagesStudy On Invasive Fungal Infections in Immunocompr PDFMelody PardilloNo ratings yet
- Epidemiological Study of Entamoeba Histolytica Among Children in Nasiriyah City, Thi-Qar, IraqDocument10 pagesEpidemiological Study of Entamoeba Histolytica Among Children in Nasiriyah City, Thi-Qar, IraqCentral Asian StudiesNo ratings yet
- Clinical Study on Strongyloides stercoralis InfectionDocument6 pagesClinical Study on Strongyloides stercoralis InfectionYisellNo ratings yet
- Blood Culture-Negative EndocarditisDocument7 pagesBlood Culture-Negative EndocarditisIkhsan Amadea9969No ratings yet
- Viral Acute Anterior Uveitis: Clinical Signs Useful For Differential DiagnosisDocument9 pagesViral Acute Anterior Uveitis: Clinical Signs Useful For Differential DiagnosisDiah Rindayani HasbiNo ratings yet
- 1 s2.0 S1473309923007569 MainDocument12 pages1 s2.0 S1473309923007569 Mainbarrientosgerman321No ratings yet
- PNTD 0007028Document16 pagesPNTD 0007028Gary Elvis TQNo ratings yet
- Characteristics of Uveitis Presenting For The First Time in The Elderly Analysis of 91 Patients in A Tertiary CenterDocument9 pagesCharacteristics of Uveitis Presenting For The First Time in The Elderly Analysis of 91 Patients in A Tertiary CenterFrancescFranquesaNo ratings yet
- Bacterial Etiology of Pediatric Subacute Hematogenous OsteomyelitisDocument6 pagesBacterial Etiology of Pediatric Subacute Hematogenous OsteomyelitismiNo ratings yet
- OutDocument8 pagesOutapi-284695722No ratings yet
- Persistence and Complex Evolution of Fluoroquinolone-Resistant Streptococcus Pneumoniae CloneDocument7 pagesPersistence and Complex Evolution of Fluoroquinolone-Resistant Streptococcus Pneumoniae CloneMark ReinhardtNo ratings yet
- A Study On Ventilator Associated Pneumonia inDocument4 pagesA Study On Ventilator Associated Pneumonia inAl MuzakkiNo ratings yet
- Candidiasis in PICUDocument6 pagesCandidiasis in PICUMeirinda HidayantiNo ratings yet
- Jurnal 2Document12 pagesJurnal 2zingioNo ratings yet
- ManuscriptDocument13 pagesManuscriptMegbaruNo ratings yet
- Commonly Occurring Bacteria in Diabetic Foot Infections and Their Sensitivity To Various AntibioticsDocument5 pagesCommonly Occurring Bacteria in Diabetic Foot Infections and Their Sensitivity To Various Antibioticsdoctor wajiha100% (1)
- 1 s20 S1438422114000988 Main - 230810 - 044728Document4 pages1 s20 S1438422114000988 Main - 230810 - 044728lmra89No ratings yet
- Novitasari - Is Premigration Health Screening For Tuberculosis WorthwileDocument12 pagesNovitasari - Is Premigration Health Screening For Tuberculosis Worthwileontet28No ratings yet
- 6 Original CandiduriaDocument7 pages6 Original CandiduriaHarnadi WonogiriNo ratings yet
- H PyloriDocument8 pagesH PyloriHabtamu WondifrawNo ratings yet
- Pediatric Oncology Fungal InfectionsDocument6 pagesPediatric Oncology Fungal InfectionserickmattosNo ratings yet
- Comparing Widal and ELISA Tests for Diagnosing Typhoid Fever in Iraqi PatientsDocument6 pagesComparing Widal and ELISA Tests for Diagnosing Typhoid Fever in Iraqi PatientsMildred MontNo ratings yet
- Risk Factor TaiwanDocument5 pagesRisk Factor TaiwanMira ApriliaNo ratings yet
- International Journal of Infectious DiseasesDocument7 pagesInternational Journal of Infectious DiseasesyurikaNo ratings yet
- Review 01-06 PDFDocument6 pagesReview 01-06 PDFEditor IjprtNo ratings yet
- Epidemiology and Clinical Characteristics of AGE in ChildrenDocument12 pagesEpidemiology and Clinical Characteristics of AGE in ChildrenGusdek AryaNo ratings yet
- 2021 Genome-Wide Association Study of Resistance To MTBDocument18 pages2021 Genome-Wide Association Study of Resistance To MTBAntonio Jafar GarciaNo ratings yet
- H Pylori Ricci2007 PDFDocument15 pagesH Pylori Ricci2007 PDFHasbiallah YusufNo ratings yet
- 2020 Bidirectional Association Between Tuberculosis and SarcoidosisDocument8 pages2020 Bidirectional Association Between Tuberculosis and SarcoidosisLCCNo ratings yet
- Invasive Fungal Sinusitis in Patients With Hematological Malignancy: 15 Years Experience in A Single University Hospital in TaiwanDocument9 pagesInvasive Fungal Sinusitis in Patients With Hematological Malignancy: 15 Years Experience in A Single University Hospital in TaiwanAngelin LigiantoNo ratings yet
- Sepsis Abdominal ScoreDocument8 pagesSepsis Abdominal ScoreMaria Ocotlan Gonzalez herreraNo ratings yet
- 1 s2.0 S0740002017304409 Main PDFDocument8 pages1 s2.0 S0740002017304409 Main PDFDIEGO FERNANDO TULCAN SILVANo ratings yet
- Fritzell2018 PDFDocument29 pagesFritzell2018 PDFJuan Fernando BermúdezNo ratings yet
- العجز الكلوي والفطرياتDocument7 pagesالعجز الكلوي والفطرياتDhurghammNo ratings yet
- Comparison of PCR, Culturing and Pap Smear Microscopy For Accurate Diagnosis of Genital ActinomycesDocument7 pagesComparison of PCR, Culturing and Pap Smear Microscopy For Accurate Diagnosis of Genital Actinomycestitaamalinda28No ratings yet
- Microbiological Study of Diabetic Foot Infections in Shaqra Hospital, Saudi ArabiaDocument10 pagesMicrobiological Study of Diabetic Foot Infections in Shaqra Hospital, Saudi Arabiaد. محمد سند راشد الحصينيNo ratings yet
- 8.A Case Report of Rabies With Long Incubation ImporDocument3 pages8.A Case Report of Rabies With Long Incubation ImporAndra CristianaNo ratings yet
- Jof 06 00216 v2Document18 pagesJof 06 00216 v2Grace Yuni Soesanti MhNo ratings yet
- Clinico - Seroepidemiological Evaluation of Toxocariasis in Asthmatic Pediatric Children in Mansoura City in EgyptDocument5 pagesClinico - Seroepidemiological Evaluation of Toxocariasis in Asthmatic Pediatric Children in Mansoura City in EgyptInternational Medical PublisherNo ratings yet
- GHFBB 15 343Document17 pagesGHFBB 15 343Chs IvankarNo ratings yet
- LeptospirosisDocument4 pagesLeptospirosisasril111No ratings yet
- Int J STD Aids 2013 Bignell 85 92Document8 pagesInt J STD Aids 2013 Bignell 85 92Ir Ardy YusriawanNo ratings yet
- OM Stafilococo (Clase Observacionales)Document7 pagesOM Stafilococo (Clase Observacionales)Jairo Camilo Guevara FaríasNo ratings yet
- PIIS1201971218345090Document9 pagesPIIS1201971218345090favorendaNo ratings yet
- 149 FullDocument10 pages149 Fullসোমনাথ মহাপাত্রNo ratings yet
- Validity of CSF Tests for Diagnosing Tuberculous MeningitisDocument5 pagesValidity of CSF Tests for Diagnosing Tuberculous MeningitismelisaberlianNo ratings yet
- 209 Full PDFDocument8 pages209 Full PDFAngga PratamaNo ratings yet
- Pathogens 12 00135Document12 pagesPathogens 12 00135Isa Andrea Aro TarquiNo ratings yet
- Ofad 120Document4 pagesOfad 120helderjamsNo ratings yet
- Hemoperitoneum in cirrhotic patients in the absence of abdominal traumaDocument11 pagesHemoperitoneum in cirrhotic patients in the absence of abdominal traumagwyneth.green.512No ratings yet
- Imaging of cerebral ischemic edema and neuronal deathDocument9 pagesImaging of cerebral ischemic edema and neuronal deathgwyneth.green.512No ratings yet
- Therapeutic plasma exchange improves short-term, but not longterm, outcomes in patients with acute-on-chronic liver failure_A propensity score-matched analysisDocument3 pagesTherapeutic plasma exchange improves short-term, but not longterm, outcomes in patients with acute-on-chronic liver failure_A propensity score-matched analysisgwyneth.green.512No ratings yet
- Dermatologic extrahepatic manifestations of Hepatitis CDocument7 pagesDermatologic extrahepatic manifestations of Hepatitis Cgwyneth.green.512No ratings yet
- A preliminary experience of plasma exchange in liver failureDocument5 pagesA preliminary experience of plasma exchange in liver failuregwyneth.green.512No ratings yet
- Clinical Management of Hyperkalemia: ReviewDocument19 pagesClinical Management of Hyperkalemia: ReviewRawan KhateebNo ratings yet
- Alcohol-Associated Liver Disease - ACG Guidelines (2024)Document25 pagesAlcohol-Associated Liver Disease - ACG Guidelines (2024)Ruber Ballesteros LoraNo ratings yet
- Pathophysiology of Takotsubo SyndromeDocument16 pagesPathophysiology of Takotsubo Syndromegwyneth.green.512No ratings yet
- Population Risk Factors For Severe Disease and Mortality in COVID-19 A Global Systematic Review and Meta-AnalysisDocument30 pagesPopulation Risk Factors For Severe Disease and Mortality in COVID-19 A Global Systematic Review and Meta-AnalysisIn House Training DialisisNo ratings yet
- Cardiogenic Pulmonary Edema in Emergency Medi - 231130 - 222540Document19 pagesCardiogenic Pulmonary Edema in Emergency Medi - 231130 - 222540Dayana OviedoNo ratings yet
- Hypertonic Saline For Sever Symptomatic Hyponatraemia - Real-World Findings From The UKDocument11 pagesHypertonic Saline For Sever Symptomatic Hyponatraemia - Real-World Findings From The UKgwyneth.green.512No ratings yet
- Jamainternal Zhang 2021 Ce 210028 1635441147.09994Document2 pagesJamainternal Zhang 2021 Ce 210028 1635441147.09994gwyneth.green.512No ratings yet
- Fundicu 2024Document14 pagesFundicu 2024gwyneth.green.512No ratings yet
- 09 222CPD-Penatalaksanaan TetanusDocument10 pages09 222CPD-Penatalaksanaan TetanusRizka ApNo ratings yet
- Hemoglobinuria Paroxistica NocturnaDocument8 pagesHemoglobinuria Paroxistica NocturnaJesúsNo ratings yet
- Paraquat Poisonings Mechanisms of Lung Toxicity Clinical Features and TreatmentDocument60 pagesParaquat Poisonings Mechanisms of Lung Toxicity Clinical Features and TreatmentDIANA MARIA TORO GOMEZNo ratings yet
- Earth First! Climbers Guild Vol. 2Document16 pagesEarth First! Climbers Guild Vol. 2CascadiaDefenders100% (2)
- Biomechinics PDFDocument8 pagesBiomechinics PDFImran KhanNo ratings yet
- Envl 4300 Lab3Document9 pagesEnvl 4300 Lab3api-662867343No ratings yet
- GMP TD Ar FPL 11033Document1 pageGMP TD Ar FPL 11033Sammy NguyenNo ratings yet
- F.E. Campbell - Sweet Slavery - HIT 139Document115 pagesF.E. Campbell - Sweet Slavery - HIT 139HokusLocus67% (3)
- Physics Investigatory Project Class 12Document12 pagesPhysics Investigatory Project Class 12shivanginirai7No ratings yet
- Type 3730-1 Electropneumatic PositionerDocument112 pagesType 3730-1 Electropneumatic PositionerDaniel ReyNo ratings yet
- The Taste of Tradition: Submitted byDocument14 pagesThe Taste of Tradition: Submitted byvijay malikNo ratings yet
- 2.factory Price - Alarm Accessories-Complete 20150325Document15 pages2.factory Price - Alarm Accessories-Complete 20150325FREE BUSINESS INTELLIGENCENo ratings yet
- Salary Exchange... A Tax Efficient Way To Boost Your Plans For The FutureDocument4 pagesSalary Exchange... A Tax Efficient Way To Boost Your Plans For The FutureStandard Life UKNo ratings yet
- M&SDocument39 pagesM&Sgo.pushp70910% (1)
- RESOLUTION 2022-08 Denial of Setback VarianceDocument5 pagesRESOLUTION 2022-08 Denial of Setback VarianceMatt McKinneyNo ratings yet
- Ni 2 WordDocument2 pagesNi 2 WordLeigh Angelika Dela CruzNo ratings yet
- DILEM 10 G (24VDC) MoellerDocument7 pagesDILEM 10 G (24VDC) MoellerElizabeth RamirezNo ratings yet
- Order - Judgement Query Coram WiseDocument13 pagesOrder - Judgement Query Coram Wisesatish_CJNo ratings yet
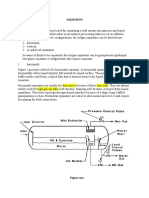
- Separators: Figure OneDocument8 pagesSeparators: Figure OneMohamed Moder100% (1)
- Experiment 1 Marble Race Virtual Science Lab Chem 2Document4 pagesExperiment 1 Marble Race Virtual Science Lab Chem 2Oribe, Narciso A.100% (1)
- SimmonsDocument12 pagesSimmonsGürelBaltalıNo ratings yet
- World Bank ReportDocument14 pagesWorld Bank Reportaditya_erankiNo ratings yet
- Effectiveness of Breathing Exercise On Reducing Pain Perception and State Anxiety Among Primi ParturientsDocument8 pagesEffectiveness of Breathing Exercise On Reducing Pain Perception and State Anxiety Among Primi ParturientsPutra SpNo ratings yet
- A 1116Document15 pagesA 1116Rama S. SinghNo ratings yet
- Early Years and Childcare Safeguarding AuditDocument4 pagesEarly Years and Childcare Safeguarding AuditEarly Years Careers100% (1)
- SECTION 03380 Post-Tensioned Concrete Rev 1Document30 pagesSECTION 03380 Post-Tensioned Concrete Rev 1Abdalrahman AntariNo ratings yet
- Round-The-clock Acid Control of Rabeprazole On Acid Related DisorderDocument8 pagesRound-The-clock Acid Control of Rabeprazole On Acid Related DisorderRabeprazole SodiumNo ratings yet
- Pre-Final Exam in Audit 2-3Document5 pagesPre-Final Exam in Audit 2-3Shr BnNo ratings yet
- An Experimental Study of AcidizingDocument11 pagesAn Experimental Study of Acidizinggigi17No ratings yet
- Hector: Genuine AccessoriesDocument18 pagesHector: Genuine AccessoriesssgfdfgNo ratings yet
- Presley v. Lockwood: Respondent's Trial BriefDocument37 pagesPresley v. Lockwood: Respondent's Trial BriefTony Ortega100% (2)
- STM - Merck Case AnswersDocument2 pagesSTM - Merck Case AnswersreetayanNo ratings yet
- RV Failure: Pathophysiology, Diagnosis and TreatmentDocument16 pagesRV Failure: Pathophysiology, Diagnosis and TreatmentRizky Regia TriseynesyaNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (403)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (20)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 4 out of 5 stars4/5 (5)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- 12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosFrom Everand12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosRating: 4.5 out of 5 stars4.5/5 (207)
- Daniel Kahneman's "Thinking Fast and Slow": A Macat AnalysisFrom EverandDaniel Kahneman's "Thinking Fast and Slow": A Macat AnalysisRating: 3.5 out of 5 stars3.5/5 (130)
- Algorithms to Live By: The Computer Science of Human DecisionsFrom EverandAlgorithms to Live By: The Computer Science of Human DecisionsRating: 4.5 out of 5 stars4.5/5 (722)
- Gut: the new and revised Sunday Times bestsellerFrom EverandGut: the new and revised Sunday Times bestsellerRating: 4 out of 5 stars4/5 (392)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisFrom EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisRating: 3.5 out of 5 stars3.5/5 (2)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- Summary: How to Be an Adult in Relationships: The Five Keys to Mindful Loving by David Richo: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: How to Be an Adult in Relationships: The Five Keys to Mindful Loving by David Richo: Key Takeaways, Summary & Analysis IncludedRating: 4 out of 5 stars4/5 (11)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Sleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningFrom EverandSleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningRating: 4 out of 5 stars4/5 (3)