You might also like
- Mujer Con Torsades de PointesDocument2 pagesMujer Con Torsades de PointesAníbal José Arroyo RodríguezNo ratings yet
- An Important Cause of Wide Complex Tachycardia: Case PresentationDocument2 pagesAn Important Cause of Wide Complex Tachycardia: Case PresentationLuis Fernando Morales JuradoNo ratings yet
- Epsilon WaveDocument3 pagesEpsilon WaveMiguel SilvaNo ratings yet
- ST Elevation in Lead aVR and Its Association With Clinical OutcomesDocument4 pagesST Elevation in Lead aVR and Its Association With Clinical OutcomesJimmy Oi SantosoNo ratings yet
- ST Elevation in Lead aVR and Its Association With Clinical OutcomesDocument4 pagesST Elevation in Lead aVR and Its Association With Clinical OutcomesshendyNo ratings yet
- Interpretasi ECG Dr. SallyDocument66 pagesInterpretasi ECG Dr. SallyRichard GunawanNo ratings yet
- Serial T-Wave Changes in A Patient With Chest PainDocument2 pagesSerial T-Wave Changes in A Patient With Chest PainsunhaolanNo ratings yet
- Cardiac Arrest and Successful Extracorporeal CardiDocument4 pagesCardiac Arrest and Successful Extracorporeal CardiDelia DeNo ratings yet
- Proximal RCA Occlusion Producing Anterior ST Segment Elevation, Q Waves, and T Wave InversionDocument5 pagesProximal RCA Occlusion Producing Anterior ST Segment Elevation, Q Waves, and T Wave InversionsunhaolanNo ratings yet
- Narrow QRS Tachycardia CaseDocument5 pagesNarrow QRS Tachycardia CaseKenWin NguyễnNo ratings yet
- Unit 6 Interpretation of EcgDocument22 pagesUnit 6 Interpretation of EcgJack TomarNo ratings yet
- Pseudonormalization of T Waves After Coronary Angioplasty A Medical Emergency 6656Document3 pagesPseudonormalization of T Waves After Coronary Angioplasty A Medical Emergency 6656Veer VajraNo ratings yet
- Materi Workshop ECG Series 4 Subtle Myocardial InfarctionDocument55 pagesMateri Workshop ECG Series 4 Subtle Myocardial InfarctionDhevi NiaNo ratings yet
- NEONARYTDocument28 pagesNEONARYToctaviena zakariaNo ratings yet
- Chyu Shah 2022 Electrocardiograms in Critical Care CardiologyDocument5 pagesChyu Shah 2022 Electrocardiograms in Critical Care Cardiologytegar ksatriaNo ratings yet
- De Winter S Pattern An Unusual But Very Important Electrocardiog - 2020 - CJC ODocument4 pagesDe Winter S Pattern An Unusual But Very Important Electrocardiog - 2020 - CJC Oastri yuniarsihNo ratings yet
- Acute Myocarditis Mimicking ST-elevation Myocardial Infarction: A Diagnostic Challenge For Frontline CliniciansDocument3 pagesAcute Myocarditis Mimicking ST-elevation Myocardial Infarction: A Diagnostic Challenge For Frontline CliniciansZazaNo ratings yet
- 2018 - Manifestaciones Electrocardiograficas de La Hiperkalemia SeveraDocument4 pages2018 - Manifestaciones Electrocardiograficas de La Hiperkalemia SeveraNANDY LUZ FERIA DIAZNo ratings yet
- Memory T-Waves, A Rare Cause of T-Wave Inversion in The Emergency Department - PMCDocument7 pagesMemory T-Waves, A Rare Cause of T-Wave Inversion in The Emergency Department - PMCfiat.2dindaNo ratings yet
- Diagnostic Examinations in Acute Ischemic Heart DiseaseDocument6 pagesDiagnostic Examinations in Acute Ischemic Heart DiseasenoemilauNo ratings yet
- Electrocardiographic Manifestations of Hyperkalemia: Amal Mattu, MD, William J. Brady, MD, and David A. Robinson, MDDocument9 pagesElectrocardiographic Manifestations of Hyperkalemia: Amal Mattu, MD, William J. Brady, MD, and David A. Robinson, MDLe TrungNo ratings yet
- Acute Myocardial Infarction-Part II: ABC of Clinical ElectrocardiographyDocument4 pagesAcute Myocardial Infarction-Part II: ABC of Clinical ElectrocardiographyAbdulkarim AlmansoorNo ratings yet
- 7InitialDraft 4Document8 pages7InitialDraft 4pigzeniNo ratings yet
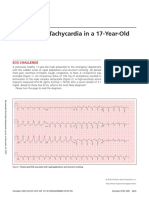
- A Wide QRS Tachycardia in A 17-Year-OldDocument4 pagesA Wide QRS Tachycardia in A 17-Year-OldTaynan MassaroNo ratings yet
- Atrioventricular Nodal Reentrant Tachycardia With 21 Atrioventricular Block.Document5 pagesAtrioventricular Nodal Reentrant Tachycardia With 21 Atrioventricular Block.Raul OrtegaNo ratings yet
- Introduction To Interpretation V10.0 (2017-2018)Document91 pagesIntroduction To Interpretation V10.0 (2017-2018)Muhammad AsrudinNo ratings yet
- Diagnosis of Acute Myocardial InfarctDocument5 pagesDiagnosis of Acute Myocardial InfarctOscar SanNo ratings yet
- Electrocardiogram Hyperkalemia: DisturbancesDocument3 pagesElectrocardiogram Hyperkalemia: DisturbancesramangNo ratings yet
- Acute Inferior Wall Myocardial Infarction: What Is The Culprit Artery?Document3 pagesAcute Inferior Wall Myocardial Infarction: What Is The Culprit Artery?Tom BiusoNo ratings yet
- Crite RiosDocument8 pagesCrite RiosNilson Morales CordobaNo ratings yet
- Arritmias VentricularesDocument11 pagesArritmias VentricularesJesusIsmaelCoronaNo ratings yet
- Im 2Document3 pagesIm 2neni budiNo ratings yet
- HSR3 10 BerlotDocument4 pagesHSR3 10 Berlotserena7205No ratings yet
- Can't Miss ECG FindingsDocument61 pagesCan't Miss ECG FindingsVikrantNo ratings yet
- Inglés Clase 1Document183 pagesInglés Clase 1Steph OsNo ratings yet
- EKG PJK Co AssDocument115 pagesEKG PJK Co AsssalmaNo ratings yet
- ECG MorphologyDocument36 pagesECG MorphologyMr Joko100% (2)
- Chapter 03Document13 pagesChapter 03matsliuNo ratings yet
- 3 Badhwar ECG VTDocument29 pages3 Badhwar ECG VTdrsanjeevsenNo ratings yet
- ECG Module 6Document28 pagesECG Module 6ibnbasheer100% (6)
- Theischemic Electrocardiogram: Daniel L. KreiderDocument16 pagesTheischemic Electrocardiogram: Daniel L. KreiderAlejandro Peñaloza TapiaNo ratings yet
- ECG InterpretationDocument5 pagesECG InterpretationjenNo ratings yet
- Ecg PDFDocument70 pagesEcg PDFlauras3005No ratings yet
- Acs HarkitDocument100 pagesAcs HarkittammypusphitarNo ratings yet
- Electrocardiographic Diagnosis of Life Threatening Stemi Equivalents Babken Asatryan MD PHD Lukas Vaisnora MD Negar Manavifar MD Full ChapterDocument26 pagesElectrocardiographic Diagnosis of Life Threatening Stemi Equivalents Babken Asatryan MD PHD Lukas Vaisnora MD Negar Manavifar MD Full Chapterwilliam.porter601100% (4)
- ECG Manifestations of Multiple Electrolyte Imbalance: Peaked T Wave To P Wave ("Tee Pee Sign")Document5 pagesECG Manifestations of Multiple Electrolyte Imbalance: Peaked T Wave To P Wave ("Tee Pee Sign")Mohammad AlzawiNo ratings yet
- EKG LanjutDocument75 pagesEKG LanjutShifa TifarinNo ratings yet
- The Ischemic Electrocardiogram: Daniel L. KreiderDocument12 pagesThe Ischemic Electrocardiogram: Daniel L. Kreidermarianagonzalezgil11No ratings yet
- Workshop SCU ACIC 2020 Untuk Peserta STEMI Mimics ECGDocument81 pagesWorkshop SCU ACIC 2020 Untuk Peserta STEMI Mimics ECGYun ZhaNo ratings yet
- The Ischemic ElectrocardiogramDocument16 pagesThe Ischemic ElectrocardiogramAdiel OjedaNo ratings yet
- Clinical Relevance of ECGDocument4 pagesClinical Relevance of ECGdrfelixNo ratings yet
- Ecginami 111115073242 Phpapp02Document104 pagesEcginami 111115073242 Phpapp02ginaul100% (1)
- TSV Con Aberrancia o TVDocument7 pagesTSV Con Aberrancia o TVOliverVasconcelosNo ratings yet
- Bradytachy SyndromeDocument3 pagesBradytachy SyndromebgusjklNo ratings yet
- MiokDocument7 pagesMiokDanijela AndjelkovicNo ratings yet
- Electrocardiogram (ECG)Document25 pagesElectrocardiogram (ECG)Laraib KanwalNo ratings yet
- Basicelectrocardiogram ppt2013Document134 pagesBasicelectrocardiogram ppt2013Catalin LeonteNo ratings yet
- ECG Signals PDFDocument14 pagesECG Signals PDFTohfatul JinanNo ratings yet
- Dermatologic Extrahepatic Manifestations of Hepatitis CDocument7 pagesDermatologic Extrahepatic Manifestations of Hepatitis Cgwyneth.green.512No ratings yet
- Hemoperitoneum in Cirrhotic Patients in The Absence of Abdominal TraumaDocument11 pagesHemoperitoneum in Cirrhotic Patients in The Absence of Abdominal Traumagwyneth.green.512No ratings yet
- A Preliminary Experience of Plasma Exchange in Liver FailureDocument5 pagesA Preliminary Experience of Plasma Exchange in Liver Failuregwyneth.green.512No ratings yet
- Imaging of Cerebral Ischemic Edema and Neuronal DeathDocument9 pagesImaging of Cerebral Ischemic Edema and Neuronal Deathgwyneth.green.512No ratings yet
- Alcohol-Associated Liver Disease - ACG Guidelines (2024)Document25 pagesAlcohol-Associated Liver Disease - ACG Guidelines (2024)Ruber Ballesteros LoraNo ratings yet
- Therapeutic Plasma Exchange Improves Short-Term, But Not Longterm, Outcomes in Patients With Acute-On-Chronic Liver Failure - A Propensity Score-Matched AnalysisDocument3 pagesTherapeutic Plasma Exchange Improves Short-Term, But Not Longterm, Outcomes in Patients With Acute-On-Chronic Liver Failure - A Propensity Score-Matched Analysisgwyneth.green.512No ratings yet
- Hypertonic Saline For Sever Symptomatic Hyponatraemia - Real-World Findings From The UKDocument11 pagesHypertonic Saline For Sever Symptomatic Hyponatraemia - Real-World Findings From The UKgwyneth.green.512No ratings yet
- Pathophysiology of Takotsubo SyndromeDocument16 pagesPathophysiology of Takotsubo Syndromegwyneth.green.512No ratings yet
- Clinical Management of Hyperkalemia: ReviewDocument19 pagesClinical Management of Hyperkalemia: ReviewRawan KhateebNo ratings yet
- Population Risk Factors For Severe Disease and Mortality in COVID-19 A Global Systematic Review and Meta-AnalysisDocument30 pagesPopulation Risk Factors For Severe Disease and Mortality in COVID-19 A Global Systematic Review and Meta-AnalysisIn House Training DialisisNo ratings yet
- Cardiogenic Pulmonary Edema in Emergency Medi - 231130 - 222540Document19 pagesCardiogenic Pulmonary Edema in Emergency Medi - 231130 - 222540Dayana OviedoNo ratings yet
- Paraquat Poisonings Mechanisms of Lung Toxicity Clinical Features and TreatmentDocument60 pagesParaquat Poisonings Mechanisms of Lung Toxicity Clinical Features and TreatmentDIANA MARIA TORO GOMEZNo ratings yet
- Fundicu 2024Document14 pagesFundicu 2024gwyneth.green.512No ratings yet
- 09 222CPD-Penatalaksanaan TetanusDocument10 pages09 222CPD-Penatalaksanaan TetanusRizka ApNo ratings yet
- Hemoglobinuria Paroxistica NocturnaDocument8 pagesHemoglobinuria Paroxistica NocturnaJesúsNo ratings yet
- Heart EditDocument51 pagesHeart EditCoral Srinivasa Ramalu100% (1)
- Glasgow PhysiciansGuideDocument90 pagesGlasgow PhysiciansGuideIstván Kecskés100% (1)
- Practice ECGStripsDocument300 pagesPractice ECGStripsFarid RodríguezNo ratings yet
- Erc - 2005Document58 pagesErc - 2005zulfantri1983No ratings yet
- Atrial FibrillationDocument1 pageAtrial FibrillationRizia Emery SwedberghNo ratings yet
- Daftar PustakaDocument2 pagesDaftar PustakaReza Ridho PahleviNo ratings yet
- Ea Re Ort: First Name: Last Name: GenderDocument2 pagesEa Re Ort: First Name: Last Name: GendernidhiNo ratings yet
- DR Mustika Mahbubi SPJP FIHA-How To Treat Acute Coronary Sydrome (STEMI Patient) in Pre and Post HospitalDocument59 pagesDR Mustika Mahbubi SPJP FIHA-How To Treat Acute Coronary Sydrome (STEMI Patient) in Pre and Post HospitalHiszom AsyhariNo ratings yet
- Practice ECGStripsDocument300 pagesPractice ECGStripsrobby zayendraNo ratings yet
- EKG Curs Asistenti Medicali GeneralistriDocument18 pagesEKG Curs Asistenti Medicali GeneralistriDiana IoanaNo ratings yet
- Cardiovascular Disorders IIDocument13 pagesCardiovascular Disorders IIAngel Joy CatalanNo ratings yet
- Tintinalli - Chapter 11 Sudden Cardiac DeathDocument3 pagesTintinalli - Chapter 11 Sudden Cardiac DeathGelo JosonNo ratings yet
- Normal Sinus RhythmDocument10 pagesNormal Sinus RhythmNakul GaurNo ratings yet
- ECG, EEG &, EMG: 45 Notes To PGDocument6 pagesECG, EEG &, EMG: 45 Notes To PGskycall28No ratings yet
- Heart Sound & MurmursDocument11 pagesHeart Sound & MurmursTraceyNo ratings yet
- Patient Implantable Medical DevicesDocument1 pagePatient Implantable Medical DevicesTracy100% (1)
- Reading Versola Ventricular TachycardiaDocument3 pagesReading Versola Ventricular TachycardiaRaijenne VersolaNo ratings yet
- Acls Algorithms Com ChecklistDocument1 pageAcls Algorithms Com ChecklistAlexandre CastroNo ratings yet
- 12 Lead ECG InterpretationDocument86 pages12 Lead ECG InterpretationNaolShamsuNo ratings yet
- Quiz 2Document7 pagesQuiz 2fatiNo ratings yet
- Echocardiography Assessment of Coronary Artery DiseaseDocument28 pagesEchocardiography Assessment of Coronary Artery DiseaseYibeltal AssefaNo ratings yet
- How To Read An EKG StripDocument9 pagesHow To Read An EKG StripRavi PandeNo ratings yet
- N205 - Basic EKG InterpretationDocument23 pagesN205 - Basic EKG InterpretationTinaHoNo ratings yet
- ACLS AgorithmDocument55 pagesACLS AgorithmkpsuanNo ratings yet
- Ifort Sport Fitness Screening Protocol - DR U.satyanarayanaDocument8 pagesIfort Sport Fitness Screening Protocol - DR U.satyanarayanau2satyascibdNo ratings yet
- Progression: ECG R-WaveDocument4 pagesProgression: ECG R-Wavekhangha.ptNo ratings yet
- ACC Cardiovascular Board Review MCQ 2017Document64 pagesACC Cardiovascular Board Review MCQ 2017Adeel Lakhiar100% (1)
- ACLS Review TestDocument5 pagesACLS Review Testtostc60% (5)
- Ecg Essentials 2 PDFDocument45 pagesEcg Essentials 2 PDFjaikishan marathe 69No ratings yet
- 4 BradyarrhythmiaDocument34 pages4 BradyarrhythmiaEverythingNo ratings yet