You might also like
- 70 Cardio Endo Rheum QuestionsDocument56 pages70 Cardio Endo Rheum QuestionslaralatifNo ratings yet
- PracticeExam1 & 2Document160 pagesPracticeExam1 & 2Arash SamieiNo ratings yet
- Masterclass Book Part 2Document367 pagesMasterclass Book Part 2Eng Kian Ng100% (5)
- Aortic dissection CT findings pathophysiologyDocument44 pagesAortic dissection CT findings pathophysiologyRoni ArmandaNo ratings yet
- PracticeExam 3 AnsDocument52 pagesPracticeExam 3 AnsBehrouz YariNo ratings yet
- QT interval drugs ECG chest painDocument7 pagesQT interval drugs ECG chest painDian ParamitaNo ratings yet
- Clin Cardiology CasesDocument34 pagesClin Cardiology CasesSunny Singh0% (1)
- INTERNAL MEDICINE - Cardiovascular SystemDocument8 pagesINTERNAL MEDICINE - Cardiovascular SystemAiswaryaNo ratings yet
- Cardiovascular Medicine Questions: Risk Assessment, Heart Failure, Chest Pain, PalpitationsDocument102 pagesCardiovascular Medicine Questions: Risk Assessment, Heart Failure, Chest Pain, PalpitationsManisha DesaiNo ratings yet
- Final Questions 2021Document8 pagesFinal Questions 2021PatrycjaSkierkaNo ratings yet
- Question 1 of 10: AAFP Board Review Clinchers Cardio Quiz 1Document60 pagesQuestion 1 of 10: AAFP Board Review Clinchers Cardio Quiz 1pramesh1No ratings yet
- Self-Assessment: BOFs for MRCP(UK) and MRCP(I) Part IFrom EverandSelf-Assessment: BOFs for MRCP(UK) and MRCP(I) Part INo ratings yet
- ACC SAP 8 Exam1&2ACC SAP 8 Exam1&2Document115 pagesACC SAP 8 Exam1&2ACC SAP 8 Exam1&2Yahya Hassan Hussein El-tamaly100% (3)
- D. ST Elevations in Lead V4RDocument4 pagesD. ST Elevations in Lead V4RDian ParamitaNo ratings yet
- Clinchers 100 Important PointsDocument21 pagesClinchers 100 Important PointsNeha GoelNo ratings yet
- ECG IMM 2020.docx.2Document25 pagesECG IMM 2020.docx.2Abdul QuyyumNo ratings yet
- Studying for the Cardiology BoardsDocument20 pagesStudying for the Cardiology BoardsDaniel Hans JayaNo ratings yet
- MCQ Cardio 3Document50 pagesMCQ Cardio 3Dian ParamitaNo ratings yet
- Cardiology - Corrected AhmedDocument23 pagesCardiology - Corrected AhmedHanadi UmhanayNo ratings yet
- NBE Cardiology Final Exam June 2020 ReviewDocument1 pageNBE Cardiology Final Exam June 2020 ReviewnarasimhahanNo ratings yet
- Cardiology 2015-mcqsDocument78 pagesCardiology 2015-mcqsAsif Newaz100% (1)
- Nuclear CardiologyDocument4 pagesNuclear CardiologysivaNo ratings yet
- MCQ Cardio 2Document54 pagesMCQ Cardio 2Dian Paramita100% (1)
- FRACP Recall Paper 2002: Part A - 70 Questions, 2 HoursDocument43 pagesFRACP Recall Paper 2002: Part A - 70 Questions, 2 HoursZH. omg sarNo ratings yet
- CT Shows Diffuse Fatty Thickening of Interatrial SeptumDocument13 pagesCT Shows Diffuse Fatty Thickening of Interatrial SeptumHaluk AlibazogluNo ratings yet
- Ecg Tutorial PDFDocument82 pagesEcg Tutorial PDFpacpacpac123No ratings yet
- 5 - Endocrinology Passmedicine Q. Bank PART I 2017Document366 pages5 - Endocrinology Passmedicine Q. Bank PART I 2017'محمد علي' محمد لافي100% (1)
- ACP Board Review Nephrology 20052ndDocument35 pagesACP Board Review Nephrology 20052nddoctormido2010100% (1)
- SABER IM PrometricDocument71 pagesSABER IM Prometricisra zaidNo ratings yet
- Nephrology ExamsDocument30 pagesNephrology Examsdhianne_garcia2001100% (1)
- ABIMDocument3 pagesABIMMohamed KhattabNo ratings yet
- Cardio Quiz Answer KeyDocument6 pagesCardio Quiz Answer KeyMark MasbadNo ratings yet
- Echocardiography Board Review: 400 Multiple Choice Questions With DiscussionFrom EverandEchocardiography Board Review: 400 Multiple Choice Questions With DiscussionNo ratings yet
- Primary and Secondary CV Prevention - Iman EvanDocument104 pagesPrimary and Secondary CV Prevention - Iman EvanFikriYTNo ratings yet
- Reading Materials in Thoracic SurgeryDocument5 pagesReading Materials in Thoracic SurgeryPradeepNo ratings yet
- Cardiology QuestionDocument63 pagesCardiology QuestionRazi Baik100% (1)
- Core V - Cardiovascular CoreDocument35 pagesCore V - Cardiovascular CoreMatthew LeiNo ratings yet
- 2007 MCQDocument67 pages2007 MCQTiffani Gutierrez100% (1)
- Guide to Cardiac Exam Findings and DiagnosesDocument58 pagesGuide to Cardiac Exam Findings and Diagnoseseliaszavaleta100% (1)
- Avinash B Kumar MD Assistant Professor Anesthesiology and Critical Care Dec 2006Document29 pagesAvinash B Kumar MD Assistant Professor Anesthesiology and Critical Care Dec 2006sgod34No ratings yet
- Nbme 2 Block 1-4Document112 pagesNbme 2 Block 1-4lk0704No ratings yet
- Assessment of Right Ventricular FunctionDocument41 pagesAssessment of Right Ventricular FunctionAditya MadhavpeddiNo ratings yet
- Cardiology 2023 FinalDocument208 pagesCardiology 2023 FinalBelinda ELISHA100% (1)
- Manual of Clinical Nephrology by Rafiqul AlamDocument12 pagesManual of Clinical Nephrology by Rafiqul AlamSELLULARNo ratings yet
- Principles of EchocardiographyDocument3 pagesPrinciples of Echocardiographys336336anl100% (1)
- MRCP(UK) and MRCP(I) Part I Best of Fives: Volume IFrom EverandMRCP(UK) and MRCP(I) Part I Best of Fives: Volume INo ratings yet
- H كدا صارDocument13 pagesH كدا صارTareq EmadNo ratings yet
- Cardiology Guide: ACS, Heart Failure, and MoreDocument260 pagesCardiology Guide: ACS, Heart Failure, and MoreDre2323No ratings yet
- 100 BCQ MRCP QuestionsDocument31 pages100 BCQ MRCP QuestionsMatin Ahmad Khan100% (1)
- Nephrology - Dr. Allam 2021Document42 pagesNephrology - Dr. Allam 2021Alokh Saha RajNo ratings yet
- Braunwald: Chronic Coronary Artery DiseaseDocument122 pagesBraunwald: Chronic Coronary Artery Diseaseusfcards100% (1)
- Comprehensive Clinical Nephrology 4th Editionl PDFDocument4 pagesComprehensive Clinical Nephrology 4th Editionl PDFJenniferNo ratings yet
- NephSAP HTNDocument88 pagesNephSAP HTNAditya JayaramanNo ratings yet
- Rokh 2e ST4 PDFDocument141 pagesRokh 2e ST4 PDFMahmud DipuNo ratings yet
- Accsap 9Document936 pagesAccsap 9Adeel Lakhiar100% (4)
- ACCSAP 10 Qs & As ReviewDocument470 pagesACCSAP 10 Qs & As ReviewAdeel Lakhiar100% (9)
- (Principles of Cardiovascular Imaging) Stuart J. Hutchison - Principles of Cardiovascular Radiology (2011, Saunders)Document461 pages(Principles of Cardiovascular Imaging) Stuart J. Hutchison - Principles of Cardiovascular Radiology (2011, Saunders)Adeel LakhiarNo ratings yet
- (Principles of Cardiovascular Imaging) Stuart J. Hutchison - Principles of Cardiovascular Radiology (2011, Saunders)Document461 pages(Principles of Cardiovascular Imaging) Stuart J. Hutchison - Principles of Cardiovascular Radiology (2011, Saunders)Adeel LakhiarNo ratings yet
- ACCA Toolkit Abridged Version PDFDocument124 pagesACCA Toolkit Abridged Version PDFNur RifqahNo ratings yet
- Dr. Anas Yasin - MDDocument58 pagesDr. Anas Yasin - MDMahfouzNo ratings yet
- Assessment of Comorbidities and Treatment Approaches in Cardiac PatientsDocument8 pagesAssessment of Comorbidities and Treatment Approaches in Cardiac PatientsManeesha KodipelliNo ratings yet
- Left Bundle Branch Block - UpToDateDocument25 pagesLeft Bundle Branch Block - UpToDateKrull TTTeamNo ratings yet
- Pacemakers & Implantable Cardioverter-Defibrillators (Icds) - Anaesthesia Tutorial of The Week 299 25 November 2013Document8 pagesPacemakers & Implantable Cardioverter-Defibrillators (Icds) - Anaesthesia Tutorial of The Week 299 25 November 2013Anup SasalattiNo ratings yet
- Pha CPR Bls Acls Manual 2012 Edited (08 25 2012)Document30 pagesPha CPR Bls Acls Manual 2012 Edited (08 25 2012)Gene Alfonso BanawaNo ratings yet
- Medical Surgical Nursing Pre-Test 2Document6 pagesMedical Surgical Nursing Pre-Test 2Blaine ManiegoNo ratings yet
- Rundown SOC HF 16-17.nov.2019Document2 pagesRundown SOC HF 16-17.nov.2019More Than WordsNo ratings yet
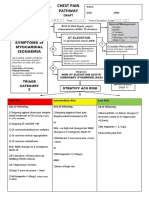
- Chest Pain Pathway GuideDocument4 pagesChest Pain Pathway GuidefauzanNo ratings yet
- Acyanotic Congenital Heart DiseaseDocument7 pagesAcyanotic Congenital Heart DiseaseSam Raj100% (1)
- ECG Minesota CodeDocument7 pagesECG Minesota CodeIman AzrbjNo ratings yet
- Peripheral Arterial Disease PADDocument27 pagesPeripheral Arterial Disease PADMd FcpsNo ratings yet
- Subarachnoid Hemorrhage With AneurysymDocument30 pagesSubarachnoid Hemorrhage With AneurysymmunaNo ratings yet
- Saudi License Exam (SLE) 3rd Edt. UQUDocument445 pagesSaudi License Exam (SLE) 3rd Edt. UQUkingmedic98% (41)
- Hypertension FamcoDocument42 pagesHypertension FamcoMusleh Al MusalhiNo ratings yet
- Thoracic Aortic AneurysmsDocument16 pagesThoracic Aortic AneurysmsdrchelluriNo ratings yet
- Emergency Cardiovascular CareDocument56 pagesEmergency Cardiovascular CareAdit PradaNaNo ratings yet
- ECG QuizDocument6 pagesECG QuizIsland Rae100% (1)
- DVT Blood Clot TestDocument4 pagesDVT Blood Clot TestvishwanathNo ratings yet
- Aortic Regurgitation Physical SignsDocument2 pagesAortic Regurgitation Physical SignsMalueth AnguiNo ratings yet
- DR Mustika Mahbubi SPJP FIHA-How To Treat Acute Coronary Sydrome (STEMI Patient) in Pre and Post HospitalDocument59 pagesDR Mustika Mahbubi SPJP FIHA-How To Treat Acute Coronary Sydrome (STEMI Patient) in Pre and Post HospitalHiszom AsyhariNo ratings yet
- 49-Year-Old Man With Chest PainDocument35 pages49-Year-Old Man With Chest PainFitriya Syaifuddin100% (1)
- Cardiovascular Tables RecommendationsDocument38 pagesCardiovascular Tables RecommendationsYesi Novia AmbaraniNo ratings yet
- Ecg ReadingsDocument11 pagesEcg ReadingsAnton Laurenciana100% (5)
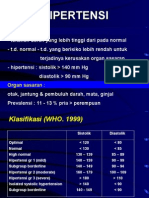
- HipertensiDocument28 pagesHipertensidokteraanNo ratings yet
- Rare and Fatal Complication of Infective Endocarditis: Emergency Case SeriesDocument3 pagesRare and Fatal Complication of Infective Endocarditis: Emergency Case SeriesVika DamayNo ratings yet
- EmbolismDocument3 pagesEmbolismprakash ramNo ratings yet
- DT AsaDocument9 pagesDT AsaReno YuandaNo ratings yet
- Blood Vessel Functions and DiseasesDocument36 pagesBlood Vessel Functions and DiseasesapplesncoreNo ratings yet
- Etiologi Dan Gejala Klinis Pneumonia RevisiDocument15 pagesEtiologi Dan Gejala Klinis Pneumonia Revisiazis purwantoNo ratings yet
- Cardiovascular For The MRCP Paces Station 3Document13 pagesCardiovascular For The MRCP Paces Station 3Ismail H A100% (1)